Regular Contribution
Preventive Effect of Oral Self-Care on Pneumonia Death among the Elderly with Tooth Loss: The Ohsaki Cohort 2006 Study
2019 Volume 247 Issue 4 Pages 251-257
Details
2019 Volume 247 Issue 4 Pages 251-257
Tooth loss is a risk factor for pneumonia mortality, but it is unclear whether oral care negates excess mortality due to pneumonia among community-dwelling elderly with tooth loss. The purpose of this study was to examine the influence of oral care on the association between the number of remaining teeth and the risk of pneumonia death. We analyzed for 18,098 individuals (aged ≥ 65 years) participating in a prospective cohort study. In a 2006 baseline survey, the following data were collected: the number of remaining teeth, oral care, history of disease, smoking, alcohol drinking, education level and so forth. We also obtained data on dates and causes of death between 2006 and 2014. The primary outcome was mortality due to pneumonia. Compared with those having ≥ 20 teeth, the risk of pneumonia mortality was increased among participants having 10-19 or 0-9 teeth; the multivariate hazard ratios (HRs) (95% confidence intervals [CI]) were 1.45 (1.03-2.04) and 1.38 (1.01-1.87), respectively. Among those having 0-9 teeth, a significantly increased risk of mortality due to pneumonia was disappeared for those who brushed their teeth ≥ 2 times per day, for those with visiting a dentist, and for those with use of denture, whereas the risk persisted among those who brushed their teeth ≤ 2 times per day, for those without visiting a dentist, and for those without use of denture. Tooth-brushing, visiting a dentist or use of denture may negate the increased risk of pneumonia death among the elderly with tooth loss.
With the aging of the Japanese population, the rate of mortality due to pneumonia has been increasing rapidly. Since 2011, pneumonia has ranked third highest among causes of death in Japan. In 2016, about 119,000 people died of pneumonia, accounting for 9.1% of all deaths. In addition, over 95% of deaths due to pneumonia were in individuals over 65 years old (Ministry of Health, Labour and Welfaere in Japan 2017).
Accordingly, various measures to prevent pneumonia are being considered. Recently, in this context, interest in the importance of oral health has been growing. The “Stop Pneumonia Campaign” launched by the Japanese Respiratory Society has emphasized oral care offered by health care workers as a preventive measure against pneumonia (The Japanese Respirator Society 2014). The World Health Organization has indicated that oral health is particularly important in disadvantaged older people and that avoiding tooth loss is crucial for healthy ageing (World Health Organization 2015).
Tooth loss is known to be a risk factor for not only mortality (Abnet et al. 2005; Holm-Pedersen et al. 2008) but also incident functional disability (Bando et al. 2017) and dementia (Takeuchi et al. 2017) among community-dwelling elderly. In addition, it has been reported that tooth loss is a risk factor for morbidity (Azarpazhooh and Leake 2006) and mortality due to pneumonia (Aida et al. 2011; Suma et al. 2018). Suma et al. (2018) have reported that the multivariate-adjusted hazard ratio was 2.07 (95% CI, 1.09-3.95) for edentulous individuals and 1.60 (95% CI, 0.83-3.10) for loss of 15-27 teeth relative to loss of 0-14 teeth (P trend = 0.026).
A randomized controlled trial by Yoneyama et al. (1999) has proved that oral care lowers the risk of pneumonia among institutionalized elderly: the relative risk of developing pneumonia in individuals with no active oral care was 1.67 (95% CI, 1.01-2.75 P = 0.04) in comparison with oral care such as tooth cleaning and visiting a dentist.
However, it is still unclear whether oral care negates excess mortality due to pneumonia among community-dwelling elderly with tooth loss. We therefore propose a hypothesis that individuals without taking oral care are associated with an increased risk of pneumonia mortality among community-dwelling elderly with tooth loss. As morbidity and mortality due to pneumonia have been rapidly increasing in Japan as society ages, any influence of oral care on mortality due to pneumonia would be a significant finding in the context of healthy aging.
The purpose of this study was to examine the influence of oral care such as tooth brushing, visiting a dentist and use of denture on the relationship between the number of remaining teeth and the risk of mortality due to pneumonia. For this purpose, we conducted a 7.2-year prospective cohort study involving more than 18,000 community-dwelling elderly subjects.
The study was based on data from the Ohsaki Cohort 2006 Study, whose design has been described in detail already (Kuriyama et al. 2010; Hayasaka et al. 2013; Bando et al. 2017). Briefly, the source population for the baseline survey comprised all men and women aged 65 years and older living in Ohsaki City, Miyagi Prefecture, northeastern Japan, on December 1, 2006. The survey included questions about the number of remaining teeth and oral care status such as tooth brushing and visiting a dentist, as well as items on history of disease, smoking, alcohol drinking, education level, time spent walking per day, psychological distress, body weight, height, and food intake frequency.
The baseline survey was conducted between December 1 and December 15, 2006. A questionnaire was distributed by the heads of individual administrative districts to all individuals aged 65 years and older living in Ohsaki city, and then collected by mail. Among 31,694 eligible subjects (12,750 men and 18,944 women), 23,091 (9,605 men and 13,486 women) provided valid responses and formed the study cohort. Among the valid respondents, we excluded 11 individuals who died or moved away during the baseline survey, 1,350 who failed to give data on the number of remaining teeth, and 3,632 who reported a history of stroke, ischemic heart disease or cancer. The remaining 18,098 participants were analyzed for the purpose of this study.
Follow upThe endpoint was death due to pneumonia. We counted the person-years of follow-up for each subject from December 16, 2006 until the date of the primary outcome, the date of death due to any cause except pneumonia, the date of emigration from Ohsaki City, or the end of the study period (March 31, 2014), whichever occurred first. In this analysis, deaths from any cause other than pneumonia were treated as censored.
Causes of death in the Vital Statistics Record (Death Certificate Notification) were assessed and classified by a trained researcher based on the International Classification of Diseases, version 10 (ICD-10). The ICD-10 codes for death caused by pneumonia are J10-18 and J69. We did not include death caused by chronic obstructive pulmonary disease (J40-44).
During the 7.2 years of follow up, information on mortality and emigration was obtained from the Residential Registry of Osaki City. During this period, only 340 individuals were lost to follow-up due to emigration; thus, the follow-up rate was 98.1%. From 119,356 person-years, the number of deaths due to pneumonia was 432 out of 3,511 all-cause deaths.
Measurement of dental health statusIn the baseline self-reported questionnaire, we asked participants “Please select the number of your remaining teeth,” and then they chose one out of six categories according to the number of their remaining teeth: all (28 teeth), most (25-27 teeth), moderate (20-24 teeth), about half (10-19 teeth), few (1-9 teeth), and none (0 teeth). Then, similarly to previous studies (Hayasaka et al. 2013; Bando et al. 2017), we divided the respondents into three groups: ≥ 20 teeth, 10-19 teeth, and 0-9 teeth.
Regarding oral self-care, we asked participants “Did you visit a dental clinic at least once a year? (including as reasons “treatment” and “other reasons such as dental check-ups and scaling”)” and then they were asked to mark “yes” or “no” in reply. We also asked participants “How many times do you brush your teeth per day?” We also asked participants “Do you usually use your denture?” and then they were asked to mark “yes” or “no” in reply.
Measurements of other variablesK6 was used as an indicator of psychological distress. Its Japanese version has been fully validated (Kessler et al. 2003; Furukawa et al. 2008). Participants were asked six questions about their mental status over the last month. Point scores ranged from 0 to 24 in total. According to the optimal cut-off point for mental illness in the validation study, we classified individuals with scores of 13 and greater as having psychological distress (Kuriyama et al. 2009).
Information on age, sex, education level, smoking and alcohol drinking status, time spent walking per day, body height and weight, psychological distress, and medical history of hypertension or diabetes mellitus was also obtained from the baseline survey.
Ethical issuesThe return of completed questionnaires was considered to imply consent to participate in the study involving the baseline survey data and subsequent follow-up of death and emigration.
The Ethics Committee of Tohoku University Graduate School of Medicine reviewed and approved the study protocol (approval code: 2006-206).
Statistical analysisBaseline characteristics were evaluated using the chi-squared test for variables of proportion and one-factor analysis of variance for continuous variables. We used these methods to compare variables among groups with different numbers of teeth.
First, we examined the relationship between the number of remaining teeth and the number of deaths due to pneumonia. The Cox proportional hazards model was used to calculate the hazard ratios (HRs) and 95% confidence intervals (CIs) for mortality from pneumonia according to the categories for different numbers of remaining teeth. Participants having ≥ 20 teeth were used as a reference category. The multivariate models were adjusted for the following variables: age (65-69, 70-74, 75-79, 80-84, and ≥ 85 years), sex (male, female), education level (age upon final graduation from school < 16, 16-18, ≥ 19 years, missing), smoking status (never, former, current, missing), alcohol drinking status (never, former, current, missing), time spent walking per day (< 30 minutes, 30 minutes-1 hour, > 1 hour, missing), history of disease (hypertension and/or diabetes mellitus), psychological distress score (< 13, ≥ 13, missing), and body mass index (kg/m2; < 18.5, 18.5-24.9, ≥ 25.0, missing).
Second, in this analysis, we examined whether the higher risk of mortality due to pneumonia among participants with fewer teeth would persist irrespective of whether they practiced oral self-care (tooth brushing ≥ 2 times per day, visiting a dentist ≥ 1 time per year or use of denture). For this, participants were divided into the following five categories based on three oral self-care measures: 1) “having ≥ 20 teeth,” 2) “practicing oral self-care and having 10-19 teeth,” 3) “non-practicing and having 10-19 teeth,” 4) “practicing and having 0-9 teeth,” and 5) “non-practicing and having 0-9 teeth,” excluding participants who failed to give data on each oral self-care. Cox proportional hazards models were used to calculate the HRs and 95% CIs for incident functional disability to compare the four categories of missing teeth with the ≥ 20 teeth category.
All statistical analyses were performed using SAS version 9.4 (SAS Inc., Cary, NC, USA), and all statistical tests were 2-sided. Differences at P < 0.05 were considered to be statistically significant.
In the study population, women accounted for 60.7% and the mean (standard deviation) age was 74.5 (6.5) years.
Table 1 shows the baseline characteristics of the participants according to the number of remaining teeth. Those who had more teeth were younger and less likely to be women, current smokers, or psychologically distressed. Having more teeth was also related to being a current drinker, being better educated, spending more time walking, and having a higher BMI.
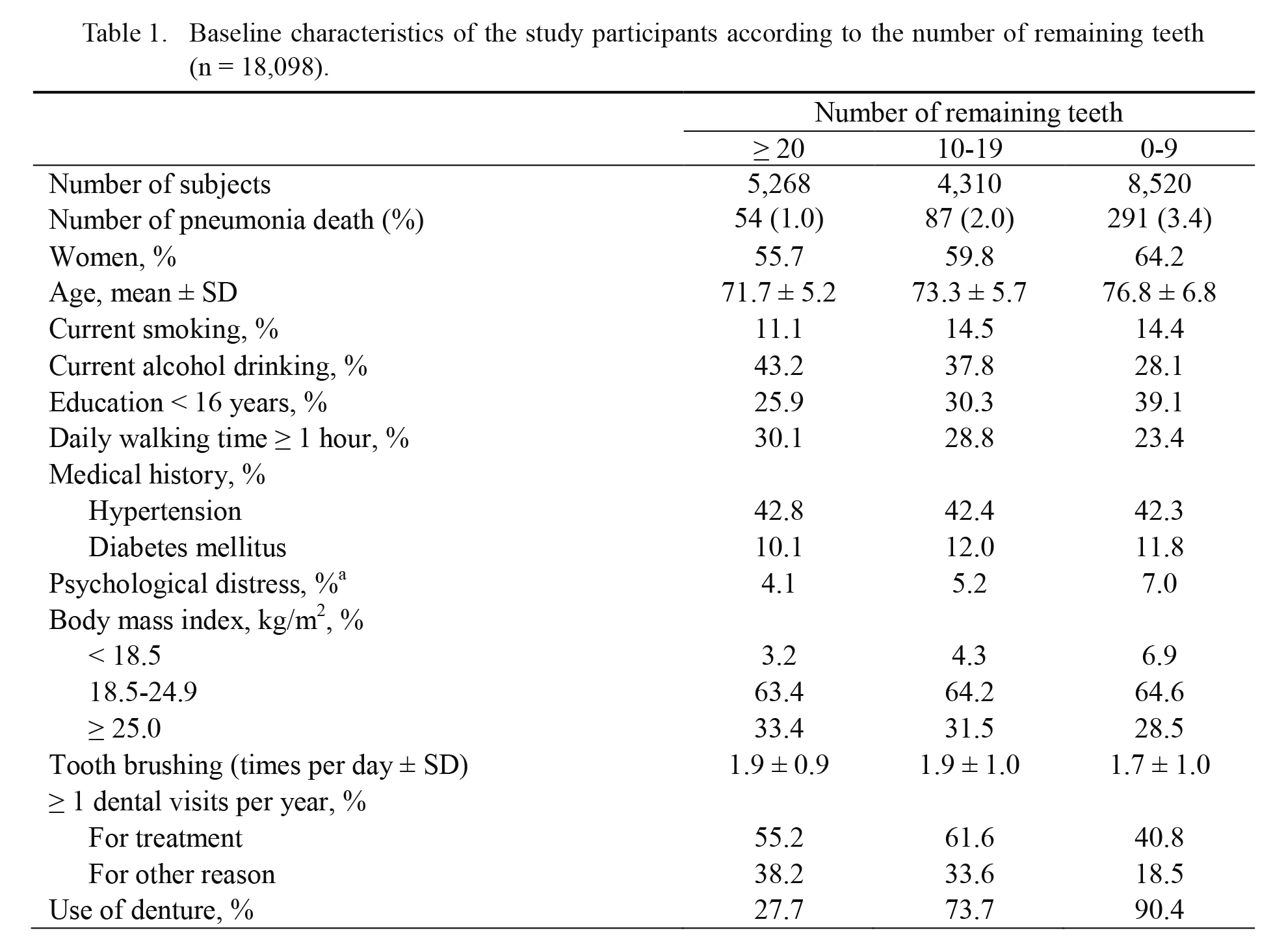
Baseline characteristics of the study participants according to the number of remaining teeth (n = 18,098).
aKessler six-item psychological distress scale score ≥ 13.
SD, standard deviation.
The total number of deaths due to pneumonia was 432; 54, 87, and 291 of these deaths occurred in individuals having ≥ 20, 10-19 and 0-9 teeth, respectively.
Table 2 shows the relationship between the number of teeth and mortality due to pneumonia. The mortality risk due to pneumonia was significantly increased among participants having 0-9 teeth, as compared with those having ≥ 20 teeth; multiple adjusted HRs (95% CIs) were 1.65 (1.22-2.23) in model 1, 1.40 (1.03-1.90) in model 2 and 1.38 (1.01-1.87) in model 3. For those having 10-19 teeth, mortality risk due to pneumonia also significantly increased: 1.56 (1.11-2.19) in model 1, 1.47 (1.04-2.07) in model 2 and 1.45 (1.03-2.04) in model 3.

Association between number of remaining teeth and mortality due to pneumonia, the Ohsaki Cohort 2006, Japan, 2006-2014 (n = 18,098).
aModel 1: Adjusted for age (65-69, 70-74, 75-79, 80-84, and ≥ 85 y) and sex.
bModel 2: Adjusted for model 1 + education level (age upon final graduation from school < 16, 16-18, ≥ 19 y, missing), smoking status (never, former, current, missing), alcohol drinking status (never, former, current, missing), time spent walking daily (< 30 min/d, 30 min/d-1 h/d, > 1 h/d, missing), history of disease (hypertension and/or diabetes mellitus), psychological distress score (< 13, ≥ 13, missing).
cModel 3: Adjusted for model 2 + body mass index (kg/m2; < 18.5, 18.5-24.9, ≥ 25.0, missing).
Table 3 shows the relationship between oral self-care (tooth-brushing, dental visits or use of denture) and mortality due to pneumonia in the five categories. Compared with participants who had 20 or more teeth, a significantly increased risk of mortality due to pneumonia was observed only among those having 0-9 teeth and brushing their teeth < 2 times per day [multivariate HR (95% CI) = 1.47 (1.06-2.04)]. Mortality risk tended to increase among other three groups (0-9 for brushing ≥ 2 times per day; 10-19 for brushing ≥ 2 times per day; and 10-19 for brushing < 2 times per day), but this was not significant.
Compared with participants who had 20 or more teeth, a significantly increased risk of mortality due to pneumonia was observed among those having 0-9 teeth and without visiting a dentist [multivariate HR (95% CI) = 1.52 (1.09-2.12)] and having 10-19 teeth and without visiting a dentist [multivariate HR (95% CI) = 1.65 (1.07-2.53)]. Mortality risk tended to increase among the other two groups, but this was not significant.
Compared with participants who had 20 or more teeth, a significantly increased risk of mortality due to pneumonia was observed among those having 0-9 teeth without use of denture [multivariate HR (95% CI) = 1.58 (1.03-2.41)]. For those having 10-19 teeth and with use of denture, a significantly increased risk of mortality due to pneumonia was also observed [multivariate HR (95% CI) = 1.46 (1.01-2.10)].

Association between oral self-care and mortality due to pneumonia according to number of remaining teeth, the Ohsaki Cohort 2006, Japan, 2006-2014.
aModel 1: Adjusted for age (65-69, 70-74, 75-79, 80-84, and ≥ 85 y) and sex.
bModel 2: Adjusted for model 1 + education level (age upon final graduation from school < 16, 16-18, ≥ 19 y, missing), smoking status (never, former, current, missing), alcohol drinking status (never, former, current, missing), time spent walking daily (< 30 min/d, 30 min/d-1 h/d, > 1 h/d, missing), history of disease (hypertension and/or diabetes mellitus), psychological distress score (< 13, ≥ 13, missing).
cModel 3: Adjusted for model 2 + body mass index (kg/m2; < 18.5, 18.5-24.9, ≥ 25.0, missing).
HR, hazard ratio; CI, confidence interval.
In this prospective cohort study of community-dwelling elderly in Japan, we found that having 20 teeth or less was significantly associated with an increased risk of death due to pneumonia, in agreement with previous studies. This increase in risk was observed among those who did not practice oral care such as regular tooth brushing, preventive dental visits or use of denture. To our knowledge, this has never been reported previously. Among participants with 0-9 teeth, a significantly increased risk of mortality due to pneumonia was observed among those brushing their teeth < 2 times per day, without visiting a dentist or without use of denture.
Our findings are consistent with previous studies indicating an inverse association between tooth loss and risk of mortality due to pneumonia in the general older population. Aida et al. (2011) reported that in comparison with respondents who had 20 or more teeth, respondents with 19 or fewer teeth and with eating difficulty had a 1.85-fold higher hazard ratio for respiratory disease mortality. Suma et al. (2018) investigated the association between tooth loss and pneumonia mortality in 19,775 Japanese dentists (mean age 51.4; 8% women), and reported that the multivariate-adjusted HRs were 2.07 for the edentulous group and 1.60 for those with loss of 15-27 teeth relative to those with loss of 0-14 teeth. In the present cohort study, among 18,098 elderly subjects in the general population, the HR of mortality due to pneumonia for participants who had 0-19 remaining teeth was significantly higher than for those had 20 or more teeth. This result is consistent with the above previous findings.
In addition, this is the first report to have demonstrated a significantly increased risk of mortality due to pneumonia among individuals with 0-9 remaining teeth who did not practice oral self-care (brushing, visiting a dentist, or use of denture). On the other hand, the risk of pneumonia mortality did not significantly increase among those having 0-9 teeth with use of denture. This result was consistent with a previous study (Hayasaka et al. 2013). Our result implies that oral self-care is desirable for elderly people with fewer teeth to prevent death due to pneumonia. For participants with 10-19 teeth, a significantly increased risk of pneumonia mortality was observed among those with use of denture but not among those without. The elderly wearing denture might have fewer teeth than those without denture, thus closer to having 0-9 teeth. Thus, the risk of pneumonia mortality among participants who had 10-19 teeth with use of denture might have increased in the same way as among those having 0-9 teeth.
Several studies including ours have agreed that tooth loss is associated with an increased risk of mortality due to pneumonia in community-dwelling populations. Those studies suggested possible mechanisms for the association between tooth loss and mortality due to pneumonia. First, periodontal disease is the one of the main reasons for tooth extraction (Suma et al. 2018), and the increase in cytokines induced by inflammation in periodontal disease may promote systemic inflammation including the lungs (Wilson et al. 1996). Second, oral bacteria propagating in the periodontal region may be associated with an increase in the risk of pneumonia (Paju and Scannapieco 2007). Another explanation could be that tooth loss would cause undernutrition and poorer immune function among the elderly, thus promoting pneumonia. Our findings, however, did not support this undernutrition hypothesis because there was no significant difference in relevance to BMI.
On the other hand, some reports have demonstrated an association between oral care and pneumonia among institutionalized or hospitalized people (Yoneyama et al. 1999; Tada and Miura 2012). Better oral hygiene through tooth brushing and dental visits may prevent death due to pneumonia, especially aspiration pneumonia. Yoneyama et al. (1999) carried out a randomized controlled trial involving 366 elderly subjects at a nursing home. The participants were randomly assigned to an oral care group and a group receiving no active treatment. The oral care group received tooth-brushing after meals by caregivers, scrubbing of the pharynx with an applicator and povidone iodine, and dental checks every week. The relative risk of developing pneumonia in the no active oral care group was 1.67 compared with the oral care group. Those previous studies involved institutionalized or hospitalized elderly. However, the present cohort study found that even among a general elderly population with fewer teeth, oral care reduced the risk of death due to pneumonia.
There is a possibility that socio-economic status might explain the association between insufficient practice of oral care and the risk of mortality due to pneumonia, because the SES including education level was reportedly associated with the frequency of dental visits in Danes (Christensen et al. 2007) and Hispanic Americans (Eke et al. 2011). However, Japan has a universal health care insurance system that covers dental services, and no significant association between regular dental visits and income has been reported in elderly Japanese (Murata et al. 2010). In addition, our results (HRs in Models 2 and 3 of Tables 2 and 3) were obtained after adjustment for education level.
The main strength of this study was that it included a large number of subjects (18,098 individuals). Second, it had a high follow-up rate of almost 100%. Third, many confounding factors were adjusted for: not only age and sex, but also education level and psychological status. Fourth, it is the first reported study to have demonstrated an association between mortality due to pneumonia and the number of remaining teeth in an elderly population in relation to oral care habits.
There were also some limitations to this study. First, misclassification of the number of remaining teeth and practicing oral self-care might have occurred as a result of self-reporting. Especially, participants might have reported the number of their remaining teeth including dental implants or long-span fixed partial denture. However, the validity of self-reporting of the number of teeth has been confirmed by previous studies (Matsui et al. 2016), and the validity of self-reporting of dental visits has also been confirmed (Gilbert et al. 2002). Second, this study was unable to take into account changes in the number of remaining teeth and oral self-care status during the 6.6 years of follow-up. Third, the number of deaths due to pneumonia observed during the relatively short follow-up period might not have been sufficient for stratified analysis. Fourth, we did not measure the strength of oral muscles, cognitive ability, respiratory function, or swallowing function. These pieces of information would have led to better understanding of the mechanism for relation between the number of remaining teeth, oral self-care and pneumonia mortality. Furthermore, we did not measure the other oral health variables such as dental plaque or tongue bacterial volume, which would affect the association between oral self-care and pneumonia mortality.
In conclusion, this study has shown that oral self-care may partially negate the increased risk of death due to pneumonia among elderly who have fewer remaining teeth. This is an important finding because the number of deaths due to pneumonia is increasing rapidly worldwide with population aging.
This work was supported by grants from the Foundation for Health Sciences Research grants (H29-Junkankitou [Seishuu]-Ippan-003 and H28-Junkankitou-Ippan-008) from the Ministry of Health, Labour and Welfare of Japan.
We would like to thank Yoshiko Nakata and Fukuko Kano for their technical assistance.
The authors declare no conflict of interest.