Abstract
The double burden of malnutrition is the coexistence of two different conditions, mainly reflected as excess or deficit in weight. Anemia is a specific nutritional deficit not always included in the double burden assessment. We reviewed overweight and/or obesity (OW/OB) and anemia studies from Latin-American Children over the last ten years up to 2019. Two authors evaluated the MEDLINE, SCOPUS, and LILACS databases. A scale of ten questions was used to assess the risk of bias in prevalence studies. Fourteen studies were selected. The population studies’ size ranged from 147 to 20,342 children with different socio-economic backgrounds, such as urban, peri-urban and rural settings, socio-economic status, schooling, population (ethnic minorities and indigenous), and environmental differences (sea level or high altitude). The prevalence of OW/OB ranged from 4.9% to 42%. The prevalence of anemia was from 3.4% to 67%. The double burden, including OW/OB and anemia, ranged from 0.7% to 67%. A higher prevalence of excess weight and anemia was found in rural and high altitude above sea level environments, extreme poverty, low education level, and indigenous communities. These heterogeneous data, before the 2020 (COVID-19 pandemic), reflect the vast inequities between countries and within each country. Food insecurity linked to poverty and the induced change in eating habits and lifestyles threaten optimal child nutrition in ongoing and future scenarios. The existence of OW/OB and anemia and their simultaneous coexistence in the community, home, and individual levels, indicates that interventions should be comprehensive to face the double burden of malnutrition.
Introduction
Double burden refers to the coexistence of two different prevalent conditions. Overweight and/or Obesity (OW/OB) and anemia seem to be opposite nutritional factors. However, there is growing evidence that these two conditions may coexist in the individual, the family, and the community levels (Popkin et al. 2020).
As proof of global concern, UNICEF offers a fresh perspective on the rapidly evolving malnutrition challenge (UNICEF 2019). Other documents also refer to children, food security, and nutrition at the international (FAO, Food and Agriculture Organization of the United Nations[Organización de las Naciones Unidas para la Alimentación y la Agricultura]2019) and the Latin American and Caribbean levels (FAO et al. 2019).
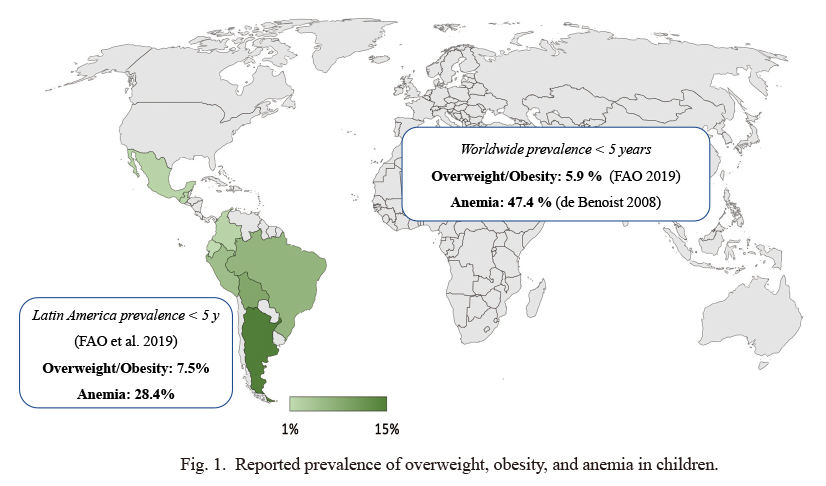
Excessive weight in Latin America and the Caribbean region is almost the highest globally, and increasing continues. The prevalence of overweight in children under five years of age in Latin American and the Caribbean is already at 7.5%, while it is 5.9% worldwide (de Benoist et al. 2008; FAO 2019). The prevalence of overweight in children under the age of five increased from 6.2% to 7.5% between 1990 and 2018. It means that four million of the child population in the region live with that condition. The most recent estimate suggests that two out of every three overweight children in the region live in a South American country (FAO et al. 2019). The observed prevalence is summarized (Fig. 1).
After a sustained reduction in the prevalence of anemia in children under five years of age until 2012, anemia again began to increase in this population group from 27.7% to 28.4 2% (FAO et al. 2019). In the same individual, obesity may coexist with stunting or anemia due to shared underlying determinants or physiological explanations (Tzioumis and Adair 2014).
Although there are many efforts for improving nutritional conditions, the so-called double burden of malnutrition, that is, underweight, wasting, anemia, or deficiency of micronutrients (vitamins and minerals) with excess weight, overweight, and obesity occurs in many socio-economical settings. The nutritional transition (Popkin 1994) is already present in low- and middle-income countries, and many of its problems are visible in Latin America.
The double burden of malnutrition exists in the Americas, specifically Latin America and the Caribbean, and can be present at the community, household, and individual levels (Rivera et al. 2014; Grajeda et al. 2019). On the other hand, the food industry plays an important role in the eating habits and diets of consumers, whose lifestyles have changed over time (Popkin and Reardon 2018).
The objective of this study was to review information about the double burden of OW/OB and anemia using available data up to 2019, prior to the COVID-19 pandemic.
Material and Methods
The MEDLINE, SCOPUS, and LILACS databases were consulted. The search for children in Latin America and the Caribbean was restricted to the past ten years. In MEDLINE, we used the “Latin America and the Caribbean Search Strategy (LACSS) (Ruiz et al. 2018), which allows us to find up to six times more bibliographic references for this region. At first, in SCOPUS, we used a complete search strategy to find information in all Latin America and the Caribbean. Still, finally, we simplified terms to the available countries in the database filters.
The search strategy at MEDLINE was:
(“obesity”[MeSH Terms] OR “obesity”[All Fields]) AND (“overweight”[MeSH Terms] OR “overweight”[All Fields]) AND (“anaemia”[All Fields] OR “anemia”[MeSH Terms] OR “anemia”[All Fields]) AND (“child”[MeSH Terms] OR “child”[All Fields]) OR “double burden”[All Fields] AND (“Anguilla”[All Fields] OR “Antigua and Barbuda”[All Fields] OR “Argentina”[All Fields] OR “Aruba”[All Fields] OR “Bahamas”[All Fields] OR “Barbados”[All Fields] OR “Bolivia”[All Fields] OR “Belice”[All Fields] OR “Belize”[All Fields] OR “Brasil”[All Fields] OR “Brazil”[All Fields] OR “British Virgin Islands”[All Fields] OR “Cayman Islands”[All Fields] OR “Chile”[All Fields] OR “Colombia”[All Fields] OR “Costa Rica”[All Fields] OR “Cuba”[All Fields] OR “Dominica”[All Fields] OR “Dominican Republic”[All Fields] OR “Republica Dominicana”[All Fields] OR “Ecuador”[All Fields] OR “El Salvador”[All Fields] OR “French Guiana”[All Fields] OR “Grenada”[All Fields] OR “Guadalupe”[All Fields] OR “Guatemala”[All Fields] OR “Guiana”[All Fields] OR “Guyana”[All Fields] OR “Haiti”[All Fields] OR “Honduras”[All Fields] OR “Leeward Islands”[All Fields] OR “Jamaica”[All Fields] OR “Martinique”[All Fields] OR “Mexico”[All Fields] OR “Montserrat”[All Fields] OR “Netherlands Antilles”[All Fields] OR “Nicaragua”[All Fields] OR “Panama”[All Fields] OR “Paraguay”[All Fields] OR “Peru”[All Fields] OR “Puerto Rico”[All Fields] OR “Saint Kitts and Nevis”[All Fields] OR “Saint Lucia”[All Fields] OR “Saint Vincent and the Grenadines”[All Fields] OR “Suriname”[All Fields] OR “Surinam”[All Fields] OR “Trinidad and Tobago”[All Fields] OR “Turks and Caicos Islands”[All Fields] OR “Uruguay”[All Fields] OR “Venezuela”[All Fields] OR “Virgin Islands of the United States”[All Fields] OR “Windward Islands”[All Fields] OR “Caribbean”[All Fields] OR “Central America”[All Fields] OR “Latin America”[All Fields] OR “South America”[All Fields] OR “West Indies”[All Fields]) AND (“2010/01/01”[PDAT] : “3000/12/31”[PDAT]).
In SCOPUS, the full search strategy was:
TITLE-ABS-KEY ((“overweight” OR “obesity” OR “double burden”) AND (“anaemia” OR “anemia”) AND “child”) AND DOCTYPE (ar) AND PUBYEAR > 2009 AND (LIMIT-TO (AFFILCOUNTRY, “Anguilla” ) OR LIMIT-TO (AFFILCOUNTRY, “Antigua and Barbuda”) OR LIMIT-TO (AFFILCOUNTRY, “Argentina”) OR LIMIT-TO (AFFILCOUNTRY, “Aruba”) OR LIMIT-TO (AFFILCOUNTRY, “Bahamas”) OR LIMIT-TO (AFFILCOUNTRY, “Barbados”) OR LIMIT-TO (AFFILCOUNTRY, “Bolivia”) OR LIMIT-TO (AFFILCOUNTRY, “Belice”) OR LIMIT-TO (AFFILCOUNTRY, “Belize”) OR LIMIT-TO (AFFILCOUNTRY, “Brasil”) OR LIMIT-TO (AFFILCOUNTRY, “Brazil”) OR LIMIT-TO (AFFILCOUNTRY, “British Virgin Islands”) OR LIMIT-TO (AFFILCOUNTRY, “Cayman Islands”) OR LIMIT-TO (AFFILCOUNTRY, “Chile”) OR LIMIT-TO (AFFILCOUNTRY, “Colombia”) OR LIMIT-TO (AFFILCOUNTRY, “Costa Rica”) OR LIMIT-TO (AFFILCOUNTRY, “Cuba”) OR LIMIT-TO (AFFILCOUNTRY, “Dominica”) OR LIMIT-TO (AFFILCOUNTRY, “Dominican Republic”) OR LIMIT-TO (AFFILCOUNTRY, “Republica Dominicana”) OR LIMIT-TO (AFFILCOUNTRY, “Ecuador”) OR LIMIT-TO (AFFILCOUNTRY, “El Salvador”) OR LIMIT-TO (AFFILCOUNTRY, “French Guiana”) OR LIMIT-TO (AFFILCOUNTRY, “Grenada”) OR LIMIT-TO (AFFILCOUNTRY, “Guadalupe”) OR LIMIT-TO (AFFILCOUNTRY, “Guatemala”) OR LIMIT-TO (AFFILCOUNTRY, “Guiana”) OR LIMIT-TO (AFFILCOUNTRY, “Guyana”) OR LIMIT-TO (AFFILCOUNTRY, “Haiti”) OR LIMIT-TO (AFFILCOUNTRY, “Honduras”) OR LIMIT-TO (AFFILCOUNTRY, “Leeward Islands”) OR LIMIT-TO (AFFILCOUNTRY, “Jamaica”) OR LIMIT-TO (AFFILCOUNTRY, “Martinique”) OR LIMIT-TO (AFFILCOUNTRY, “Mexico”) OR LIMIT-TO (AFFILCOUNTRY, “Montserrat”) OR LIMIT-TO (AFFILCOUNTRY, “Netherlands Antilles”) OR LIMIT-TO (AFFILCOUNTRY, “Nicaragua”) OR LIMIT-TO (AFFILCOUNTRY, “Panama”) OR LIMIT-TO (AFFILCOUNTRY, “Paraguay”) OR LIMIT-TO (AFFILCOUNTRY, “Peru”) OR LIMIT-TO (AFFILCOUNTRY, “Puerto Rico”) OR LIMIT-TO (AFFILCOUNTRY, “Saint Kitts and Nevis”) OR LIMIT-TO (AFFILCOUNTRY, “Saint Lucia”) OR LIMIT-TO (AFFILCOUNTRY, “Saint Vincent and the Grenadines”) OR LIMIT-TO (AFFILCOUNTRY, “Suriname”) OR LIMIT-TO (AFFILCOUNTRY, “Surinam”) OR LIMIT-TO (AFFILCOUNTRY, “Trinidad and Tobago”) OR LIMIT-TO (AFFILCOUNTRY, “Turks and Caicos Islands”) OR LIMIT-TO (AFFILCOUNTRY, “Uruguay”) OR LIMIT-TO (AFFILCOUNTRY, “Venezuela”) OR LIMIT-TO (AFFILCOUNTRY, “Virgin Islands of the United States”) OR LIMIT-TO (AFFILCOUNTRY, “Windward Island) OR LIMIT-TO (AFFILCOUNTRY, “Caribbean”) OR LIMIT-TO (AFFILCOUNTRY, “Central America”) OR LIMIT-TO (AFFILCOUNTRY, “Latin America”) OR LIMIT-TO (AFFILCOUNTRY, “South America”) OR LIMIT-TO (AFFILCOUNTRY, “West Indie”)).
In LILACS, the search strategy was:
tw:(overweight obesity anemia children) AND (db:(“LILACS”) AND (year_cluster:[2010 TO 2020]).
Two reviewers (CD, RS) used the search strategy and found 190 articles. After reviewing the titles, we selected 124 papers, and after reviewing the summaries, we chose 45 articles for full-text reading. (Flow Diagram in Fig. 2). The Cohen Kappa concordance index (Cohen 1960) was 0.61 for the title review and 0.66 for the revision of summaries, representing a substantial agreement among reviewers.
Full-text reading of selected articles allowed data extraction shown in Tables 1 and 2 in the Results section.
A scale of ten questions was used to assess the risk of bias in prevalence studies (Munn et al. 2014). The Joanna Briggs Institute’s ten-question scale was used, and each affirmative answer was counted as one point, having a minimum score of zero (0) and a maximum of ten (
The Joanna Briggs Institute 2017).
Ethics
The data sources were openly accessible to the public; thus, no ethical review was required.
Results
On March 22, 2020, the full MEDLINE search retrieves 110 articles. In SCOPUS, 70 additional articles were found (including 24 that were already identified in MEDLINE). In LILACS, ten other articles were found (including one that was already identified in MEDLINE). In total, we found 190 articles in three databases. Evaluating the titles, abstracts, and full text using previously established criteria selects 13 papers and one thesis with complete data for review (Fig. 2).
Fourteen papers with dual disease burden data were identified in children (Table 1). The average score on the critical evaluation scale for the fourteen articles was 7.9. Two articles scored 6, two scored 7, five scored 8, and five scored 9.
Table 2 shows the double-load data reported in eight countries: Argentina, Brazil, Colombia, Ecuador, Guatemala, Perú, México, and Bolivia. Mexico and Guatemala are from Central America, and the remaining six are from South America.
In Argentina, Rivas and Gotthelf (2018) reported a cross-sectional survey of children and adolescents in the Salta region in 2014. This study evaluated 147 children under the age of five, showing that 12.9% had anemia. Of these, 47.5% were overweight/obese.
In Brazil, three studies were found. Conde and Monteiro (2014) conducted a study in children aged four to 29 months in community daycare centers finding a prevalence of overweight of 22.2% and anemia of 37%. Jardim-Botelho et al. (2016) reported another study, based on a cross-sectional survey performed in a low-income community in children less than 12 months, reported a prevalence of 31.4% for OW/OB and 67% for anemia. In the third study, de Novaes Oliveira et al. (2010) found in children aged 12 to 24 months, the coexistence of obesity and anemia with a prevalence of 6.3%, and a triple load of stunting, obesity, and anemia, with a prevalence of 1.85%.
In Colombia, Sarmiento et al. (2014) showed the existence of double burden (obesity and anemia) in 1.4% of 10,317 children, slightly lower than the expected of 1.5%, in school-age children aged five to 12 years. Syed et al. (2016) found the double burden of overweight and anemia in 1.7% of 8,573 children aged five to 14 years.
In Ecuador, Freire et al. (2014) found the coexistence of obesity/overweight and anemia in 0.7% of school-age children five to 11 years, at the individual level.
In Guatemala, Ramirez-Zea et al. (2014) studied indigenous and non-indigenous populations, and the coexistence of obesity/overweight and anemia at the individual level was 1.4%. The double burden of malnutrition was more prevalent in the indigenous population, both in the household and individual levels.
In Perú, there were three studies. The thesis of Palma Gutierrez (2019) reported a prevalence of obesity and anemia of 1.8% in children from 6 to 59 months. Pajuelo Ramírez and Miranda Cuadros (2016) showed a prevalence of 5%. The work of Rodríguez-Zúñiga (2015) found a combined prevalence of overweight or obesity and anemia in 4.4% of children under five years of age. This author also found a double burden prevalence in 3.1% in the 6-11 years age group and 2.4% of those over 12 years old.
In México, Kroker-Lobos et al. (2014) found that 2.9% of 16,351 children, aged five to 11 years, were overweight/obese and had anemia. In another study, Torres Ornelas et al. (2011) reported 1.3% obesity and anemia, mainly in children less than five years of age.
In Bolivia, Jones et al. (2018) studied three types of populations: urban, peri-urban, and rural. The overall prevalence of double nutritional burden of overweight and anemic children was 6.6%, showing that peri-urban areas have a higher prevalence of double burden of overweight and anemia.
Discussion
This study reviewed the available data of double burden OW/OB and anemia in Latin-American children under five years old. We found fourteen epidemiological studies that met our selection criteria to determine the coexistence of these opposite nutritional factors.
Within nutritional transition, the double burden of malnutrition is currently faced by low-income and middle-income countries. Malnutrition involves low weight for age (underweight), low height for age (stunting), low weight for height (wasting), and micronutrient deficiencies (vitamins and minerals). Excess weight refers to overweight and obesity. The double burden of malnutrition can occur within a country, a city, a community, a household, and an individual (Popkin et al. 2020). It is important to note that the nutritional transition depends on the place of residence, whether it is urban or rural (Loret de Mola et al. 2014).
Efforts have been made to address the double burden of malnutrition in Latin America and the Caribbean (Galicia et al. 2016; Grajeda et al. 2019). Exclusive and appropriate breastfeeding protects infants against all forms of malnutrition (Wells et al. 2020). Furthermore, the first 1,000 days of life (from conception to two years of life) are crucial for the adult’s posterior health (Victora et al. 2008). One of the great challenges is to simultaneously face malnutrition with overweight/obesity, so it has been called double-duty and double task challenge (double function,) in a holistic way (Hawkes et al. 2020).
According to FAO, there are three phases in the nutritional transition: Phase 1, early-stage, when malnutrition is high and overweight/obesity is low; Phase 2, when double burden, malnutrition, and overweight/obesity are high; Phase 3, when the transition is completed, malnutrition is low and overweight/obesity is high (FAO et al. 2019).
In the case of Perú, in a national survey, Chaparro and Estrada (2012) showed that only one region was in Phase 1, 16 in Phase 2, and 7 in Phase 3. This reflects that the nutritional possibilities, must account for this diversity. Curi-Quinto et al. (2020) found that the geographical distribution of malnutrition, including OW/OB, and anemia depended on socio-economic indicators. Aparco et al. (2016) studied school children aged six to ten years in an urban center and found stunting in 5% of the children and anemia in 11.9%, while obesity/overweight affected 46.7% of them. These studies show that double burden of malnutrition is found in Perú.
Argentina faces a different nutritional transition, where socio-demographic factors play a significant role in shaping diverse nutritional transition profile factors. Most of the identified profiles were linked to the obesity burden in adults. The study included children with anemia (Tumas et al. 2019). Zapata et al. (2020) found that in 2005 Argentina had high excess weight and anemia rates, a moderate prevalence of stunting, and low frequency of wasting/underweight. All forms of malnutrition showed a strong relationship with social, economic, and educational inequalities. Cordero and Cesani (2019) showed that the non-homogenous children population from Tucuman revealed differences concerning sex, area of residence, and socio-economic status, undergoing an accelerated process of nutritional transition, manifested by the double burden of malnutrition.
In Ecuador, Houck et al. (2013) reported that market integration into the indigenous population suggests that they influence the double burden of malnutrition and excess weight. Lopez et al. (2018) expressed that even though more communities have gained more access to roads, it seems, still, that the population with less road access and more remote had better nutritional outcomes than those communities living close to a highway. Malnutrition differs significantly across socio-demographic groups, disproportionately affecting those in the low-wealth and ethnic minorities (indigenous). Double-duty actions are urgently required for the double burden (Ramírez-Luzuriaga et al. 2020). Garrido-Salazar et al. (2018) found that anemia’s prevalence was higher in children in rural communities located in the high altitudes.
In México, western and plant-based dietary patterns were simultaneously associated with a higher prevalence of overweight-obesity and at least one undernutrition indicator (Zarate-Ortiz et al. 2019). In the context of the double burden of malnutrition, dietary advice must consider malnutrition in all its forms (Zarate-Ortiz et al. 2019). Gain in height among boys, but not in girls, in early childhood, was associated with lower adiposity in late childhood compared with children with a slower rate of growth (Barrios et al. 2019).
In Brazil, a socio-epidemiological longitudinal study found marked disparities in the double burden of malnutrition (including anemia and excess weight) of the indigenous populations compared to the general population (Welch et al. 2020). In cross-sectional studies, the double burden of malnutrition (stunting in children and excess weight in the mother) was associated with the educational level and non-masonry (inadequate) houses (Gea-Horta et al. 2016). A survey on indigenous populations showed the double burden of malnutrition, stunting (26%), and anemia (51%) in children under five years of age and excess weight in women in reproductive age (WRA) (Coimbra et al. 2013). At the household level, the double burden of malnutrition(stunting) in children under five years and excess weight in WRA was associated with severe food insecurity (Gubert et al. 2017). The sample size may explain the large differences in observed prevalence in Brazil.
In Uruguay, Severi and Moratorio (2014) found a double burden of malnutrition, including anemia, even though the epidemiological transition was more advanced. They found anemia in 31% of children under two years and excess weight increase with age in 35% of adults.
Pinhas-Hamiel et al. (2003) reported more iron deficiency prevalence in overweight and obese children and adolescents in Israel. They expressed that insufficient dietary intake of iron, either absolute or relative to body mass, and increased iron needs may result from unbalanced nutrition or repetitive restrictive diets in the short term.
Concerning micronutrients, 61% of Mexicans infants, 6-11.9 months old, did not meet the estimated average iron requirement, indicating a nutritional risk (Villalpando-Carrion and Eldridge 2019). Sharply higher rates of iron deficiency in obese Mexican women and children are predicted by obesity-related inflammation rather than by differences in dietary iron intake (Cepeda-Lopez et al. 2011).
Several studies focused on indigenous populations (Coimbra et al. 2013; Ramirez-Zea et al. 2014; Welch et al. 2020; Ramírez-Luzuriaga et al. 2020). Welch et al. (2020) found that, in children under ten years old in indigenous communities in Brazil, stunting, wasting, and malnutrition, including anemia, were more notorious. In general, it is notorious that the prevalence of the double burden of malnutrition, including anemia, is disproportionately higher in indigenous groups than in the general population (Coimbra et al. 2013; Ramírez-Luzuriaga et al. 2020).
Poor hygiene conditions in communities of Bolivia highlands showed a greater prevalence of malnutrition and anemia, while children in the lowland population showed more overweight or obesity (Teran et al. 2018). Another study revealed more than double the cases of anemia in the highland rural areas than those in the lowlands (Garrido-Salazar et al. 2018). However, this difference may have been due to a better economic status in the lowland population.
Differences in the prevalence of double burden of malnutrition, including anemia, depended on whether the children came from periurban or rural areas. Periurban areas are well spread in Latin America. Periurban areas surrounding cities like Mexico City, Caracas, Bogota, Rio de Janeiro, Lima, and Sao Paulo, are confronted with violence, poverty, and environmental problems in various degrees (da Gama Torres 2008). Populations in peri-urban areas were associated with the double burden of malnutrition, more than in rural areas, showing overweight and anemia in children, overweight mothers, and stunted children (Jones et al. 2018).
The double burden of malnutrition also occurred in households with children under five years of age and mothers who were overweight/obese (Gea-Horta et al. 2016; Gubert et al. 2017). This coexistence of both conditions calls for actions aimed at addressing them simultaneously, depending on the higher or lower prevalence of double burden of malnutrition and the distribution in different regions within each country (Chaparro and Estrada 2012) or areas of residence (Cordero and Cesani 2019; Curi-Quinto et al. 2020; Zapata et al. 2020). Countries like Chile seemed to be in an advanced or outdated nutritional transition stage, with a low frequency of stunting and a high prevalence of overweight/obesity (Atalah et al. 2014).
Obesity affects children progressively, with patterns of sedentary lifestyles and frequent consumption of foods high in sugar, salt, or fats (Aparco et al. 2016; Villalpando-Carrion and Eldridge 2019).
We still do not know how the COVID-19 pandemic is going to evolve (Delgado et al. 2020), and also, we cannot advance how it will affect the nutritional status of the population. Nevertheless, we already know that obesity is one of the predisposing conditions that increase the risk of being affected by the COVID-19 infection and worsens the prognosis (Deng et al. 2020; Sanchis-Gomar et al. 2020).
Amid the development of the pandemic, it is very difficult to have a strategic plan or proposals to deal with excess weight and anemia in children. Prior to the COVID-19 pandemic, some Latin American countries, such as Ecuador, Bolivia, Perú, México, Chile, and Uruguay, which are already trying to develop public policies creating more favorable food environments to face these issues, such as the labels of industrialized foods pointing those with high quantities of sodium, sugar and saturated and trans fats. Other initiatives promote healthy eating for children and adolescents (FAO et al. 2019). The critical appraisal of ongoing interventions and detailed descriptive studies must support evidence-based public policies.
In the face of the conditions imposed to us by the COVID-19 pandemic, this review’s relevance is that it reflects the nutritional status of children before the pandemic. Food insecurity in poverty-stricken countries and the change of eating habits and lifestyles at a global level will most certainly result in changes in the nutritional status that will be interesting to study and will be of great value for ongoing or future scenarios. We do not know yet precisely what the effect of the COVID-19 pandemic will be on the nutritional indicators in children (The Lancet Global Health 2020). We even do not know how affected the millennium development goals are and the proposed targets (United Nations 2015, 2019).
However, there is little doubt that facing the challenge of dealing with the existing double burden nutritional problem and the progress amid the COVID-19 pandemic will require urgent and extraordinary efforts from all of us.
Acknowledgments
The authors (R.S. and C.A.D.) would like to thank to the Universidad Nacional Mayor de San Marcos for providing the time to write this article.
Author Contributions
C.D. and R.S. designed the research; R.S. and C.D. analyzed the data; R.S. wrote the draft paper; G.N., A.T. and P.V. gave constructive suggestions; R.S. and C.D. had primary responsibility for the final content. All authors read and approved the final manuscript.
Conflict of Interest
The authors declare no conflict of interest.
References
-
Aparco,
J.P.,
Bautista-Olortegui,
W.,
Astete-Robilliard,
L. &
Pillaca,
J.
(2016) Assessment of the nutritional status, physical activity, and eating habits of schoolchildren in Cercado de Lima. Rev. Peru. Med. Exp. Salud Publica, 33, 633-639.
-
Atalah,
E.,
Amigo,
H. &
Bustos,
P.
(2014) Does Chile’s nutritional situation constitute a double burden? Am. J. Clin. Nutr., 100, 1623S-1627S.
-
Barrios,
P.L.,
Garcia-Feregrino,
R.,
Rivera,
J.A.,
Barraza-Villarreal,
A.,
Hernandez-Cadena,
L.,
Romieu,
I.,
Gonzalez-Casanova,
I.,
Ramakrishnan,
U. &
Hoffman,
D.J.
(2019) Height trajectory during early childhood is inversely associated with fat mass in later childhood in Mexican boys. J. Nutr., 149, 2011-2019.
-
Cepeda-Lopez,
A.C.,
Osendarp,
S.J.,
Melse-Boonstra,
A.,
Aeberli,
I.,
Gonzalez-Salazar,
F.,
Feskens,
E.,
Villalpando,
S. &
Zimmermann,
M.B.
(2011) Sharply higher rates of iron deficiency in obese Mexican women and children are predicted by obesity-related inflammation rather than by differences in dietary iron intake. Am. J. Clin. Nutr., 93, 975-983.
-
Chaparro,
M.P. &
Estrada,
L.
(2012) Mapping the nutrition transition in Peru: evidence for decentralized nutrition policies. Rev. Panam. Salud Publica, 32, 241-244.
-
Cohen,
J.
(1960) A coefficient of agreement for nominal scales. Educ. Psychol. Meas., 20, 37-46.
-
Coimbra,
C.E. Jr.,
Santos,
R.V.,
Welch,
J.R.,
Cardoso,
A.M.,
de Souza,
M.C.,
Garnelo,
L.,
Rassi,
E.,
Foller,
M.L. &
Horta,
B.L.
(2013) The first national survey of indigenous people’s health and nutrition in Brazil: rationale, methodology, and overview of results. BMC Public Health, 13, 52.
-
Conde,
W.L. &
Monteiro,
C.A.
(2014) Nutrition transition and double burden of undernutrition and excess of weight in Brazil. Am. J. Clin. Nutr., 100, 1617S-1622S.
-
Cordero,
M.L. &
Cesani,
M.F.
(2019) Nutritional transition in schoolchildren from Tucuman, Argentina: a cross-sectional analysis of nutritional status and body composition. Am. J. Hum. Biol., 31, e23257.
-
Curi-Quinto,
K.,
Ortiz-Panozo,
E. &
López de Romaña,
D.
(2020) Malnutrition in all its forms and socio-economic disparities in children under 5 years of age and women of reproductive age in Peru. Public Health Nutr., 23, s89-s100.
-
da Gama Torres,
H.
(2008) Social and environmental aspects of peri-urban growth in Latin American megacities, United Nations expert group meeting on population distribution, urbanization, internal migration and development. United Nations Secretariat. https://www.un.org/en/development/desa/population/events/pdf/expert/13/P10_Torres.pdf [Accessed: July 12, 2020].
-
de Benoist,
B.,
Cogswell,
M.,
Egli,
I. &
McLean,
E.
(2008) Worldwide prevalence of anaemia 1993-2005; WHO global database of anaemia. https://www.who.int/nutrition/publications/micronutrients/anaemia_iron_deficiency/9789241596657/en/ [Accessed: September 1, 2020].
-
de Novaes Oliveira,
M.,
Martorell,
R. &
Nguyen,
P.
(2010) Risk factors associated with hemoglobin levels and nutritional status among Brazilian children attending daycare centers in Sao Paulo City, Brazil. Arch. Latinoam. Nutr., 60, 23-29.
-
Delgado,
C.A.,
Shimabuku,
R.L. &
Chiroque-Solano,
P.M.
(2020) COVID-19 waves: importance of accumulative mortality per million inhabitants. Tohoku J. Exp. Med., 251, 47-49.
-
Deng,
M.,
Qi,
Y.,
Deng,
L.,
Wang,
H.,
Xu,
Y.,
Li,
Z.,
Meng,
Z.,
Tang,
J. &
Dai,
Z.
(2020) Obesity as a potential predictor of disease severity in young COVID-19 patients: a retrospective study. Obesity (Silver Spring), 28, 1815-1825.
-
Food and Agriculture Organization of the United Nations (FAO)
(2019) The State of Food Security and Nutrition in the World 2019. Safeguarding against economic slowdowns and downturns. Rome, FAO. Licence: CC BY-NC-SA 3.0 IGO. http://www.fao.org/3/ca5162en/ca5162en.pdf [Accessed: July 12, 2020].
-
Freire,
W.B.,
Silva-Jaramillo,
K.M.,
Ramirez-Luzuriaga,
M.J.,
Belmont,
P. &
Waters,
W.F.
(2014) The double burden of undernutrition and excess body weight in Ecuador. Am. J. Clin. Nutr., 100, 1636S-1643S.
-
Galicia,
L.,
de Romana,
D.L.,
Harding,
K.B.,
De-Regil,
L.M. &
Grajeda,
R.
(2016) Tackling malnutrition in Latin America and the Caribbean: challenges and opportunities. Rev. Panam. Salud Publica, 40, 138-146.
-
Garrido-Salazar,
D.I.,
Garrido-Salazar,
S.M.,
Torres-Changoluisa,
T.,
Fuseau-Herrera,
M.,
Muyulema-Ruiz,
C.,
Palate-Nuñez,
P.,
Toapanta,
E.P. &
Gutiérrez-Tapia,
M.
(2018) Prevalence of anemia in children from two rural schools at different altitudes. A transversal study. Acta Pediatr. Mex., 39, 289-298.
-
Gea-Horta,
T.,
Silva Rde,
C.,
Fiaccone,
R.L.,
Barreto,
M.L. &
Velasquez-Melendez,
G.
(2016) Factors associated with nutritional outcomes in the mother-child dyad: a population-based cross-sectional study. Public Health Nutr., 19, 2725-2733.
-
Grajeda,
R.,
Hassell,
T.,
Ashby-Mitchell,
K.,
Uauy,
R. &
Nilson,
E.
(2019) Regional overview on the double burden of malnutrition and examples of program and policy responses: Latin America and the Caribbean. Ann. Nutr. Metab., 75, 139-143.
-
Gubert,
M.B.,
Spaniol,
A.M.,
Segall-Correa,
A.M. &
Perez-Escamilla,
R.
(2017) Understanding the double burden of malnutrition in food insecure households in Brazil. Matern. Child Nutr., 13, e12347.
-
Hawkes,
C.,
Ruel,
M.T.,
Salm,
L.,
Sinclair,
B. &
Branca,
F.
(2020) Double-duty actions: seizing programme and policy opportunities to address malnutrition in all its forms. Lancet, 395, 142-155.
-
Houck,
K.,
Sorensen,
M.V.,
Lu,
F.,
Alban,
D.,
Alvarez,
K.,
Hidobro,
D.,
Doljanin,
C. &
Ona,
A.I.
(2013) The effects of market integration on childhood growth and nutritional status: the dual burden of under- and over-nutrition in the Northern Ecuadorian Amazon. Am. J. Hum. Biol., 25, 524-533.
-
Jardim-Botelho,
A.,
Queiroz Gurgel,
R.,
Simeone Henriques,
G.,
Dos Santos,
C.B.,
Afonso Jordao,
A.,
Nascimento Faro,
F.,
Silveira Souto,
F.M.,
Rodrigues Santos,
A.P. &
Eduardo Cuevas,
L.
(2016) Micronutrient deficiencies in normal and overweight infants in a low socio-economic population in north-east Brazil. Paediatr. Int. Child Health, 36, 198-202.
-
Jones,
A.D.,
Hoey,
L.,
Blesh,
J.,
Janda,
K.,
Llanque,
R. &
Aguilar,
A.M.
(2018) Peri-urban, but not urban, residence in bolivia is associated with higher odds of co-occurrence of overweight and anemia among young children, and of households with an overweight woman and stunted child. J. Nutr., 148, 632-642.
-
Kroker-Lobos,
M.F.,
Pedroza-Tobias,
A.,
Pedraza,
L.S. &
Rivera,
J.A.
(2014) The double burden of undernutrition and excess body weight in Mexico. Am. J. Clin. Nutr., 100, 1652S-1658S.
-
Lopez,
V.K.,
Dombecki,
C.,
Trostle,
J.,
Mogrovejo,
P.,
Castro Morillo,
N.,
Cevallos,
W.,
Goldstick,
J.,
Jones,
A.D. &
Eisenberg,
J.N.S.
(2018) Trends of child undernutrition in rural Ecuadorian communities with differential access to roads, 2004-2013. Matern. Child Nutr., 14, e12588.
-
Loret de Mola,
C.,
Quispe,
R.,
Valle,
G.A. &
Poterico,
J.A.
(2014) Nutritional transition in children under five years and women of reproductive age: a 15-years trend analysis in Peru. PLoS One, 9, e92550.
-
Munn,
Z.,
Moola,
S.,
Riitano,
D. &
Lisy,
K.
(2014) The development of a critical appraisal tool for use in systematic reviews addressing questions of prevalence. Int. J. Health Policy Manag., 3, 123-128.
-
Organización de las Naciones Unidas para la Alimentación y la Agricultura (FAO); Organización Panamericana de la Salud (OPS); Programa Mundial de Alimentos (WFP); Fondo de las Naciones Unidas para la Infancia (UNICEF)
(2019) Panorama de la seguridad alimentaria y nutricional en América Latina y el Caribe 2019. Santiago. 135. Licencia: CC BY-NC-SA 3.0 IGO. http://www.fao.org/3/ca6979es/ca6979es.pdf [Accessed: July 12, 2020].
-
Pajuelo Ramírez,
J. &
Miranda Cuadros,
M.
(2016) La coexistencia de problemas nutricionales en niños menores de 5 años en el Perú 2007-2010. An. Fac. Med. (Perú), 77, 345-349.
-
Palma Gutierrez,
J.E.
(2019) Prevalencia de la coexistencia de anemia y sobrepeso u obesidad en niños de 6 a 59 meses de edad y factores sociodemográficos asociados en el Perú, Master degree thesis,The Universidad Peruana Cayetano Heredia.
-
Pinhas-Hamiel,
O.,
Newfield,
R.S.,
Koren,
I.,
Agmon,
A.,
Lilos,
P. &
Phillip,
M.
(2003) Greater prevalence of iron deficiency in overweight and obese children and adolescents. Int. J. Obes. Relat. Metab. Disord., 27, 416-418.
-
Popkin,
B.M.
(1994) The nutrition transition in low-income countries: an emerging crisis. Nutr. Rev., 52, 285-298.
-
Popkin,
B.M.,
Corvalan,
C. &
Grummer-Strawn,
L.M.
(2020) Dynamics of the double burden of malnutrition and the changing nutrition reality. Lancet, 395, 65-74.
-
Popkin,
B.M. &
Reardon,
T.
(2018) Obesity and the food system transformation in Latin America. Obes. Rev., 19, 1028-1064.
-
Ramírez-Luzuriaga,
M.J.,
Belmont,
P.,
Waters,
W.F. &
Freire,
W.B.
(2020) Malnutrition inequalities in Ecuador: differences by wealth, education level and ethnicity. Public Health Nutr., 23, s59-s67.
-
Ramirez-Zea,
M.,
Kroker-Lobos,
M.F.,
Close-Fernandez,
R. &
Kanter,
R.
(2014) The double burden of malnutrition in indigenous and nonindigenous Guatemalan populations. Am. J. Clin. Nutr., 100, 1644S-1651S.
-
Rivas,
P.C. &
Gotthelf,
S.J.
(2018) Anemia y estado nutricional en la población de la ciudad de Salta. Actual. nutr, 19, 4-11.
-
Rivera,
J.A.,
Pedraza,
L.S.,
Martorell,
R. &
Gil,
A.
(2014) Introduction to the double burden of undernutrition and excess weight in Latin America. Am. J. Clin. Nutr., 100, 1613S-1616S.
-
Rodríguez-Zúñiga,
M.J.
(2015) Obesity, overweight and anemia in children from a rural area of Lima, Peru. Medicina (B. Aires), 75, 379-383.
-
Ruiz,
E.F.,
Proano,
A.,
Proano,
D.,
Torres-Roman,
J.S. &
Miranda,
J.J.
(2018) The Latin America and the Caribbean search strategy proposal. Glob. Health Promot., 25, 60-64.
-
Sanchis-Gomar,
F.,
Lavie,
C.J.,
Mehra,
M.R.,
Henry,
B.M. &
Lippi,
G.
(2020) Obesity and outcomes in COVID-19: when an epidemic and pandemic collide. Mayo Clin. Proc., 95, 1445-1453.
-
Sarmiento,
O.L.,
Parra,
D.C.,
Gonzalez,
S.A.,
Gonzalez-Casanova,
I.,
Forero,
A.Y. &
Garcia,
J.
(2014) The dual burden of malnutrition in Colombia. Am. J. Clin. Nutr., 100, 1628S-1635S.
-
Severi,
C. &
Moratorio,
X.
(2014) Double burden of undernutrition and obesity in Uruguay. Am. J. Clin. Nutr., 100, 1659S-1662S.
-
Syed,
S.,
Addo,
O.Y.,
De la Cruz-Gongora,
V.,
Ashour,
F.A.,
Ziegler,
T.R. &
Suchdev,
P.S.
(2016) Determinants of anemia among school-aged children in Mexico, the United States and Colombia. Nutrients, 8, 387.
-
Teran,
G.,
Cuna,
W.,
Branez,
F.,
Persson,
K.E.M.,
Rottenberg,
M.E.,
Nylen,
S. &
Rodriguez,
C.
(2018) Differences in nutritional and health status in school children from the highlands and lowlands of Bolivia. Am. J. Trop. Med. Hyg., 98, 326-333.
-
The Joanna Briggs Institute
(2017) The Joanna Briggs Institute critical appraisal tools for use in JBI systematic reviews: checklist for prevalence studies.
https://joannabriggs.org/sites/default/files/2020-08/Checklist_for_Prevalence_Studies.pdf [Accessed: July 1, 2020].
-
The Lancet Global Health
(2020) Food insecurity will be the sting in the tail of COVID-19. Lancet Glob. Health, 8, e737.
-
Torres Ornelas,
P.,
Evangelista Salazar,
J.J. &
Martínez-Salgado,
H.
(2011) Coexistence of obesity and anemia in children between 2 and 18 years of age in Mexico. Bol. Med. Hosp. Infant. Mex., 68, 431-437.
-
Tumas,
N.,
Rodriguez Junyent,
C.,
Aballay,
L.R.,
Scruzzi,
G.F. &
Pou,
S.A.
(2019) Nutrition transition profiles and obesity burden in Argentina. Public Health Nutr., 22, 2237-2247.
-
Tzioumis,
E. &
Adair,
L.S.
(2014) Childhood dual burden of under- and overnutrition in low- and middle-income countries: a critical review. Food Nutr. Bull., 35, 230-243.
-
UNICEF
(2019) The state of the world’s children 2019: children, food and nutrition: growing well in a changing world. https://www.unicef.org/reports/state-of-worlds-children-2019 [Accessed: September 1, 2020].
-
United Nations
(2019) The Sustainable Development Goals Report 2019: New York: United Nations. https://unstats.un.org/sdgs/report/2019/The-Sustainable-Development-Goals-Report-2019.pdf [Accessed: September 1, 2020].
-
United Nations
(2015) Transforming our world: The 2030 agenda for sustainable development: New York: United Nations, Department of Economic and Social Affairs. https://sustainabledevelopment.un.org/post2015/transformingourworld [Accessed: September 1, 2020].
-
Victora,
C.G.,
Adair,
L.,
Fall,
C.,
Hallal,
P.C.,
Martorell,
R.,
Richter,
L. &
Sachdev,
H.S.;
Maternal and Child Undernutrition Study Group
(2008) Maternal and child undernutrition: consequences for adult health and human capital. Lancet, 371, 340-357.
-
Villalpando-Carrion,
S. &
Eldridge,
A.L.
(2019) Feeding patterns of infants and toddlers: the Mexico case study. Nestle Nutr. Inst. Workshop Ser., 91, 89-97.
-
Welch,
J.R.,
Ferreira,
A.A.,
Tavares,
F.G.,
Lucena,
J.R.M.,
Gomes de Oliveira,
M.V.,
Santos,
R.V. &
Coimbra,
C.E.A .Jr.
(2020) The Xavante Longitudinal Health Study in Brazil: objectives, design, and key results. Am. J. Hum. Biol., 32, e23339.
-
Wells,
J.C.,
Sawaya,
A.L.,
Wibaek,
R.,
Mwangome,
M.,
Poullas,
M.S.,
Yajnik,
C.S. &
Demaio,
A.
(2020) The double burden of malnutrition: aetiological pathways and consequences for health. Lancet, 395, 75-88.
-
Zapata,
M.E.,
Soruco,
A.I. &
Carmuega,
E.
(2020) Malnutrition in all its forms and socio-economic indicators in Argentina. Public Health Nutr., 23, s13-s20.
-
Zarate-Ortiz,
A.G.,
Melse-Boonstra,
A.,
Rodriguez-Ramirez,
S.,
Hernandez-Cordero,
S. &
Feskens,
E.J.M.
(2019) Dietary patterns and the double burden of malnutrition in Mexican adolescents: results from ENSANUT-2006. Nutrients, 11, 2753.