Abstract
In situations of a disaster, it has been observed that the damage suffered by women and men is not equal. The vulnerability of women during disasters has been the focus of several studies and disaster management guidelines. Records show that there were more women victims than men victims in both the Great Hanshin-Awaji Earthquake in 1995 and the Great East Japan Earthquake (GEJE) in 2011. Biologically speaking, women are physically less fit than men are; hence, they are more susceptible to physical disabilities induced by disasters and may be disadvantaged in evacuation situations. However, vulnerability of women during disasters is a complex problem that involves physical fitness, as well as other various factors. In the Sendai Framework for Disaster Risk Reduction 2015-2030 (SFDRR) adopted in 2015, prioritized actions such as “Build Back Better” were defined based on the GEJE experiences. In the SFDRR, in addition to vulnerability of women during disasters, medical services including maternal, newborn, and child health and sexual and reproductive health are considered the key factors for disaster risk reduction. This has been discussed in all phases of disaster risk reduction planning and post-disaster response. These findings suggest that the role of obstetrics and gynecology is comprehensive and important as a part of disaster medicine at the local and national levels, as recommended in the SFDRR. In this review, we summarized the management of women’s health and gynecological responses during disasters and considered the importance of women as stakeholders in disaster risk reduction.
Introduction
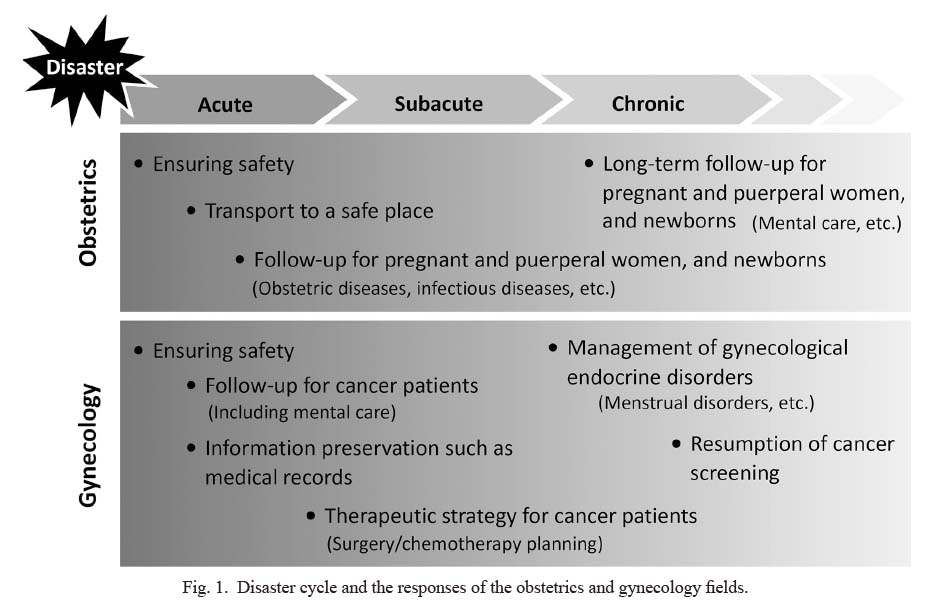
Disaster medicine is divided into three phases: acute, subacute, and chronic; both phase-specific and consistent responses are required. The first week of the disaster is the acute phase that focuses on rescue and emergency medical care. In the next 2-3 weeks, the subacute phase follows, which includes internal medicine and treatment of infectious diseases. The chronic phase of the disaster cycle comprises reconstruction and recovery, with consideration for rehabilitation and mental care (Yamamoto 2007). The disaster cycle and the responses of the obstetrics and gynecology fields are summarized in Fig. 1.
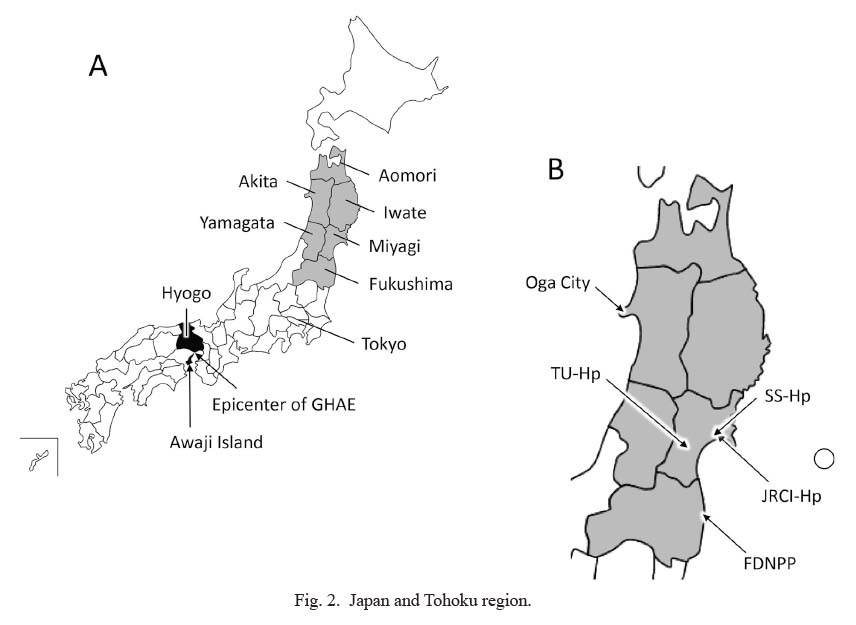
The efficacy of maternal and child health (MCH) handbooks, which originated in Japan, is known in various countries (Nakamura 2014; Yoshida 2021a). In the aftermath of the Great East Japan Earthquake (GEJE), the loss of MCH handbook exposed the vulnerabilities of paper-based medical information management during disasters (Uebayashi et al. 2014). In the earthquake-stricken area of Iwate Prefecture (Fig. 2), the Electronic Perinatal Record Network System-Ihatov via the internet was established in 2009, and the MCH handbook data has been saved in the electronic form (JICA 2014; Uebayashi et al. 2014). There is an urgent need to build and deploy disaster-resilient systems, including digitization of medical information and establishment of a network system for its management (Yoshida 2021b). Verification and discussions have been held on the topic of “Disaster and Obstetrics” from various perspectives in the field of obstetrics (Nishigori et al. 2014; Sugawara et al. 2016; Kyozuka et al. 2018; Yoshida 2021b).
In the field of gynecology, extensive care is required for the physiological problems of women from every age group, both young and old. Furthermore, gynecological gaps including oncological ones in disaster still need to be identified and solved. Therefore, this review focused on “Disasters and Women” and “Disasters and Gynecology” as the key terms and considered the measures for the management of women’s health during a disaster.
Disaster and Women
The 1995 Southern Hyogo Prefecture earthquake caused enormous damage in the Kinki region, especially Kobe City, Hyogo Prefecture, which was close to the epicenter of the earthquake (Fig. 2). It is called the Great Hanshin-Awaji Earthquake. Ten years after this earthquake, the 2nd United Nations (UN) World Conference on Disaster Risk Reduction was held in Kobe in 2005. At the meeting, the “Hyogo Framework for Action” was adopted as a basic guideline for disaster prevention activities for the next 10 years (UNDRR 2007). According to the guidelines, disaster risk reduction has been given priority by the national and local governments, and emergency responses in the event of a disaster have been strengthened. It was found that the actions based on this guideline suppressed the increase in the number of deaths due to disasters in the next 10 years (UNDRR 2015). On the other hand, in these 10 years, large-scale disasters cost the deaths of many people worldwide. Small-scale disasters associated with climate change in recent years have continued to affect the economy and human health of the community seriously. Moreover, it has been pointed out that vulnerable populations, such as women and children, are significantly affected by these disasters (UNDRR 2015).
The 2011 earthquake off the Pacific coast of Tohoku was a huge earthquake that originated in the Pacific Ocean off Sanriku, Japan on March 11, 2011 (Fig. 2). The disasters, including the Fukushima Daiichi Nnuclear Power Plant accident caused by this huge earthquake, are collectively called the GEJE. In 2015, 4 years after the GEJE, the 3rd UN World Conference on Disaster Risk Reduction was held in Sendai City, one of the disaster-stricken areas. The “Sendai Framework for Disaster Risk Reduction” was adopted as a 15-year global disaster-risk reduction guideline (UNDRR 2015). One of the basic policies of the guideline is the importance of leadership exercised by women and young people, and women are expected to play the role of stakeholders in various responses and in the prevention of disasters (UNDRR 2015; Obi-Aso et al. 2021).
Globally, women have been identified as being the vulnerable population during disasters, and it has been reported that women and children are many times more likely to die in the event of a disaster as compared to men (Saito 2014; Habtezion 2016). As of March 2012, the total number of deaths of men and women in Iwate, Miyagi, and Fukushima Prefectures after the GEJE (Fig. 2) was 7,360 and 8,363, respectively (Cabinet Office 2012). The sex differences in the number of deaths over the age of 80 years were striking (1,290 men vs. 2,091 women) (Cabinet Office 2012). Additionally, the same tendency was observed in the Great Hanshin-Awaji Earthquake, and the death toll in Hyogo Prefecture was 2,713 men and 3,680 women, of which 471 men and 776 women were aged 80 years or above (Cabinet Office 2012). For these evaluations, the results should be corrected by the ratio of men and women in the population at that time. On the other hand, the population of women aged 80 years or above was less than 10% of the total in the areas affected by the Great East Japan Earthquake; however, the number of victims was more than a quarter of the total. Biological, physical, and physiological sex differences are directly associated with the number of disaster victims (Neumayer and Plümper 2007). Moreover, social status, economic potential, and behavioral patterns are believed to contribute to the vulnerability of women during disasters (Neumayer and Plümper 2007).
Disaster and Gynecology
A survey of the 2008 Wenchuan earthquake in China reported that more women complained of gynecological disorders, such as pelvic inflammatory disease, menstrual disorders, and lower genital tract infections, after the disaster (Liu et al. 2010a). Menstrual disorders in particular were thought to be due to mental health disorders such as obsessive-compulsive traits and sleep disorders (Liu et al. 2010b). Furthermore, about 30% of the surviving women who suffered significant losses in the Wenchuan earthquake complained of post-earthquake menstrual irregularities, indicating that mental stress such as loss of children, property, and social resources are strongly associated with such complaints (Li et al. 2011). Symptoms of premenstrual syndrome (PMS) are known to interfere with work, study, and interpersonal relationships, affecting normal daily activities (Rapkin and Winer 2009). Nine months after the GEJE, the association between premenstrual syndrome (PMS) and posttraumatic stress disorder (PTSD) was investigated in 1,489 female students belonging to two high schools in Sendai, but their locations were unrelated to the damage caused by the tsunami (Takeda et al. 2013a). Among the 1,180 respondents, 10% were strongly suspected of having PTSD, which was markedly higher than the commonly seen 0.4%. PMS with severe psychiatric symptoms is called premenstrual dysphoric disorder (PMDD). Among the respondents, moderate/severe PMS and PMDD were found in only 11% of the group without suspected PTSD and in 42% of the group with suspected PTSD. It was also reported that there was a significant association between GEJE-induced PTSD and the severity of dysmenorrhea (Takeda et al. 2013b). Psychiatric symptoms such as anxiety and post-traumatic stress reactions induced by the disaster is not improved even after several years after the disaster (Okuyama et al. 2017, 2021). In women’s health care, it has been considered that close cooperation between psychosomatic medicine and gynecology can have various benefits, such as expanding treatment options for patients. In disaster medicine, it is necessary to provide both mental and physical care for women at the same time. It is also necessary to investigate the causes of impaired women’s mental health during and after a disaster and to eliminate them.
In the 2014 post-GEJE survey, the three determinants of increased tobacco consumption after a disaster were female sex, working age (20-59 years), and experience of disaster-related unemployment (Koyama et al. 2021). It is well established that smoking including passive smoking is associated with various health hazards such as carcinogenesis, cardiovascular diseases, and respiratory disorders (Trofor et al. 2019; Sharma and Khapre 2021). Smoking is also known to cause disturbances in the endocrine systems, such as hormonal imbalance. Female premenopausal smokers have high progesterone and testosterone levels, low estrogen levels, and less menstrual phase-related variations of estrogen levels (Dušková et al. 2012; Gu et al. 2013). It has been reported that in young Japanese female smokers, smoking status affected the menstrual cycle, but not the menstrual duration. In addition, the incidence of PMS in women has been reported to be significantly higher in smokers than in nonsmokers (Sakai et al. 2011). Smoking was also associated with an increased risk of PMS in a previous meta-analysis (Choi and Hamidovic 2020). Mental stress caused by drastic changes in the living environment, such as living in a shelter after a disaster, may encourage smoking or its resumption (Osaki et al. 2020). Passive smoking is also known to be associated with menstrual disorders (Sakai and Ohashi 2021); hence, providing smoking cessation counseling to both male and female smokers in the disaster-affected areas is important for maintaining the menstrual and overall health of women.
Disaster and Gynecologic Oncology
Disaster and treatment for cancer patients
After the GEJE, a questionnaire was administered to cancer patients who were prescribed cancer drug therapy at the following three hospitals in Miyagi Prefecture: Tohoku University Hospital, Sendai; Japanese Red Cross Ishinomaki Hospital, Ishinomaki; and Senseki Hospital, Higashimatsushima (Fig. 2) (Akiyama et al. 2013). The number of chemotherapies conducted reverted to the number before the earthquake in April 2011 at Tohoku University Hospital and Senseki Hospital in the month following the disaster and in June at the Red Cross Hospital. At Senseki Hospital, the number of chemotherapies conducted continued to increase, reaching 180% of that before the earthquake in November 2011. This finding may be attributed to the division of roles among the three hospitals. Ishinomaki Red Cross Hospital prioritized disaster medicine during the acute phase and Senseki Hospital accepted patients who requested chemotherapy. Tohoku University Hospital provided support for cancer treatment by dispatching specialists to these two hospitals in the Ishinomaki area. However, the burden on Senseki Hospital was not reduced even after the resumption of chemotherapy at Ishinomaki Red Cross Hospital, which suggests that long-term support is required after a major disaster. Patients with chronic diseases, including cancer, are hospital-dependent, and hospital collapse is considered a serious problem with respect to their treatment (Akiyama et al. 2013; Gorji et al. 2018). Furthermore, the collapse of transportation infrastructure prevents patients from going to the hospital (Akiyama et al. 2013; Gorji et al. 2018). In the above survey, among the 85 cancer patients (61 patients residing in coastal areas at the time of the disaster), 62.3% had to discontinue their cancer treatment (Akiyama et al. 2013).
The challenge in cancer treatment during a disaster is the concentration of the medical care facilities on the treatment of injuries, prevention of infectious diseases, and treatment of evacuees. This process affects the services usually available to cancer patients and reduces access to routine medical services for those with cancer and other chronic diseases (Gorji et al. 2018; Rodriguez-Rabassa et al. 2020). Arao et al. (2007) conducted a survey for the nurses present during the Great Hanshin-Awaji Earthquake. They found that the challenges in providing treatment and nursing care to cancer patients during a disaster were “difficulty in keeping track of patients,” “adjustment in treatment,” and “care for patients and their families before and after the last moment in the case of terminally ill patients.”
In the event of a disaster, cancer patients need to be identified as a vulnerable population requiring additional attention and assistance. This is not just a problem in Japan but throughout the world. Incorporating patient care into the event management framework will improve resilience, reduce distress, and save lives (Alcalde-Castro et al. 2018; De Guzman and Malki 2019; Verna et al. 2019; Sahar et al. 2020). In addition to establishing a relief and support system for cancer patients in the event of a disaster at the government level, it is also important for patients to acquire knowledge regarding cancer medicine, be aware of disaster prevention, and prepare for disasters (Akiyama et al. 2013; Gorji et al. 2018). It is important for cancer patients to keep a track of the medication and treatment information. In the event of a disaster, there is no guarantee that the patients will be treated at the medical institution that they usually visit; hence, patients need to be prepared to provide the following personal medical information correctly: (1) the drug they are taking, (2) name of the disease, and (3) any allergies to drugs. It is also useful in an emergency to keep photos of the medicine and prescriptions on your mobile phone as well as the record on paper. In fact, in the responses to the aforementioned survey after the GEJE (Akiyama et al. 2013), the proportion of cancer patients who could explain their disease (89%) and provide the name of the disease (82%) was high, but that of patients who could provide the name of the drug (40%) and the number of treatments (51%) was low. It is also important to confirm the contact information and evacuation destinations. It is necessary to consult with the doctor or nurse in charge to decide whom and how to contact in the event of a disaster. To the best extent possible, sharing such information with cohabitants and relatives residing in remote areas should also be considered.
Disaster and patient’s delay
Although both early detection and early treatment are important in cancer cases, some women do not visit a medical institution at the appropriate time, even if they are aware of breast cancer signs such as lumps. In breast cancer patients, hesitation to visit a medical institution for more than 3 months after recognizing symptoms significantly affects the 5-year survival rate (Richards et al. 1999). The clinical stage of breast cancer progresses if there is a delay in visiting a medical institution (Richards et al. 1999). The delay in becoming a patient, called “Patient’s Delay,” is associated with various factors such as psychological, financial, and domestic factors. Additionally, conflicts and disasters are known to disrupt the medical system and result in delays in the diagnosis and treatment of cancer patients (Ozaki et al. 2017a, b; El Saghir et al. 2018). A woman living in Fukushima noticed a lump in her right breast in April 2011 immediately after the GEJE, but she visited a medical institution after 3 years and 3 months (Ozaki et al. 2016). She was diagnosed with stage 3B advanced breast cancer. It has been suggested that one of the causes of her presenting “Patient’s Delay” was social isolation after the disaster (Ozaki et al. 2016). In a survey of breast cancer patients in Fukushima Prefecture, a significant increase in the risk of excessive patient’s delay, which was more than 12 months from symptom recognition to consultation, was observed at 2 years, 4 years, and 5 years after the disaster (Ozaki et al. 2017b). It was also found that most such patients did not live with their children (Ozaki et al. 2017b). Epidemiological studies have revealed that the rate of social isolation increased after the GEJE (Yokoyama et al. 2014). In women, mental health problems are associated with a lack of social networks and relocation experiences (Yokoyama et al. 2014), suggesting that social isolation affects their health. Since “Patient’s Delay” in cancer is a problem that continues after a disaster, long-term care by a supporter with specialized knowledge, such as cancer screening, is required.
Cytopathology is known worldwide to reduce the incidence of both cervical cancer and cancer-related mortality (Aoki et al. 2020). It has been reported that the rate of uterine cancer screening in the United States and the United Kingdom is about 70-80%, while that in Japan is 40% (Komiyama and Hasegawa 2017; Aoki et al. 2020). Thus, the number of patients with cervical cancer is declining in many developed countries, but it has been increasing in Japan since the late 1990s (Utada et al. 2019). These facts also show that it is important to conduct regular cervical cancer screening for women to reduce the risk. In a study in New Orleans after Hurricane Katrina, the mean time from the last cytology of the Papanicolaou trial to the diagnosis of cervical cancer was significantly longer after the hurricane than that before it (7.7 years vs. 4.2 years). Furthermore, the clinical stage of cervical cancer at diagnosis was significantly more severe after the hurricane than that before the hurricane (Kanjanvaikoon et al. 2011). We had previously analyzed the cervical cancer screening rates in 45 areas of Miyagi Prefecture from 2009 to 2016 before and after the GEJE (Miki et al. 2020). In 2011, when the earthquake struck, there was a significant decrease in the rate of cervical cancer screening in many areas. Furthermore, in some coastal areas affected by the tsunami, the rate of cervical cancer screening did not recover until 2016, and there were regional disparities in the reconstruction of health management for residents of the affected areas (Miki et al. 2020). After the GEJE, which occurred in the spring, cancer screening promptly resumed in most of the affected areas, but it took until winter in the severely damaged coastal areas. It was thought that cancer screening would be restored by the rapid restoration of clinics and screening systems, but in reality, it was not. This could be because health management cannot be reconstructed only by restoring medical software and hardware. Social capital, as described in the next section, is considered important for health promotion (Tsunoda et al. 2008; Nishigori et al. 2017). Further investigations are needed, but the sufficient accumulation of social capital during normal times could help in the healthcare management of women after a disaster.
Disaster and Women’s Health Communication
In 2013, a survey was conducted on the trends of health examinations and cancer examinations in Oga City, Akita Prefecture (Fig. 2), which was the area affected by the GEJE (Taguchi and Natsuhara 2014). In normal times, those who were attached to their area of residence showed a high tendency to undergo health examinations and cancer screenings, especially women; when “There are many examinees in their neighbors and acquaintances,” the rate of examinees was high (Taguchi and Natsuhara 2014). Additionally, a survey conducted in Fukushima Prefecture revealed that groups who had strong bonds with other local people were more likely to undergo health examinations (Hasegawa et al. 2018). It is suggested that active district events and voluntary participation in them can promote health care. Furthermore, it is necessary to maintain the community when relocating affected people from the evacuation site for better health management so that they are not isolated in an unfamiliar environment. Social capital has been known to play an important role in various disaster processes such as disaster prevention for communities and individuals, evacuation behavior, evacuating life, sending/receiving support, and reconstruction (Aldrich 2011; Aldrich and Kyota 2017; Akbar and Aldrich 2018; Ozaki et al. 2018; Horiuchi et al. 2019). In terms of sex differences in social capital, women, especially the elderly, are predominantly of the bonding type, i.e., dependent on their family, neighbors, and close friends, and men are predominantly the bridging type, i.e., dependent on the workplace and its affiliates (Hsueh 2019). The role of social capital for both men and women was also recognized in their evacuation behavior during a disaster. In the survey conducted for the three aforementioned prefectures of the Tohoku region (Cabinet Office 2012), 82% of women evacuated as a group, while 64% of men evacuated alone. The proportion of men who evacuated alone was higher than that of women (29% vs. 13%). In order to maintain the health of the affected people in the affected areas, it is important to strengthen and revitalize regional cooperation by accumulating social capital during normal times and to maintain it in the event of a disaster. In addition to women’s medical care and disaster medicine, it is necessary to build a comprehensive care system for self-care, informal care, and formal care.
Conclusion
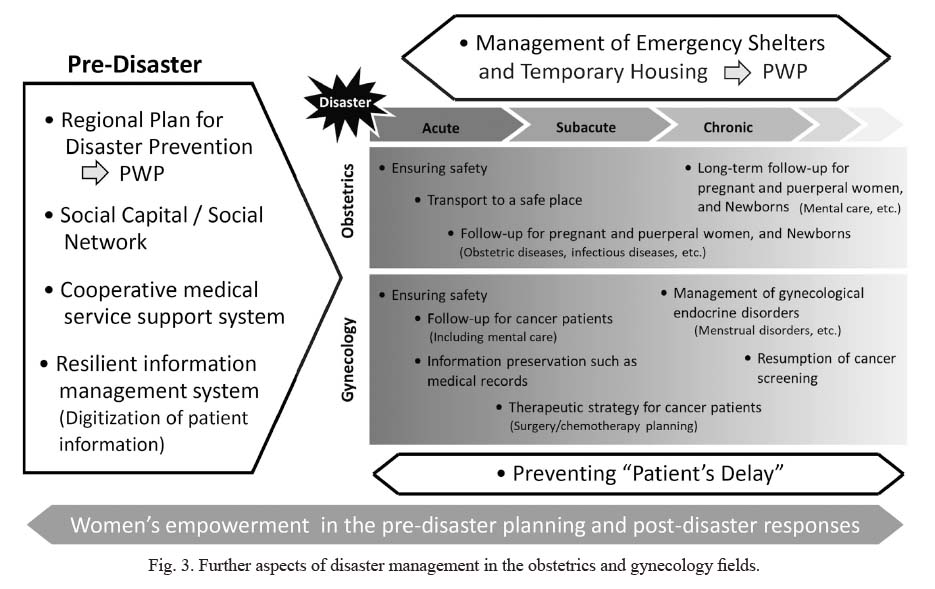
“Health” is the focus of the SFDRR and is considered a key factor in disaster risk reduction (Egawa et al. 2018; Egawa 2021). One of the key issues in “Priority action: Investing in disaster risk reduction for resilience” was access to basic healthcare services including maternal, newborn, and child health and sexual and reproductive health (UNDRR 2015). Therefore, the role of obstetrics and gynecology in disaster medicine and disaster prevention has increased. Further aspects of disaster obstetrics and gynecology are summarized in Fig. 3. In preparation for disasters, it is necessary to build cooperation between hospitals and develop a medical information management system that is resilient to disasters. Moreover, the activation of social capital and social networks in the region is important. For the establishment and operation of disaster medicine that is more resilient, it is necessary to consider a system that operates comprehensively rather than one that functions separately. In all the pre-disaster to post-disaster phases, promotion of women’s participation is required not only for disaster medicine, but also for other aspects such as planning and operation of evacuation shelters and temporary housing and disaster risk reduction. Demonstrating women’s empowerment in all aspects of disaster management may be the key to establishing a comprehensive disaster medical system.
Conflict of Interest
The authors declare no conflict of interest.
References
-
Akbar,
M.S.P. &
Aldrich,
D.P.
(2018) Social capital’s role in recovery: evidence from communities affected by the 2010 Pakistan floods. Disasters, 42, 475-497.
-
Akiyama,
S.,
Seya,
Y.,
Murayama,
M.,
Ogasawara,
K.,
Kisara,
S.,
Ishii,
T.,
Sugawara,
M.,
Chida,
Y.,
Kanbe,
M.,
Kakudo,
Y.,
Mano,
N. &
Ishioka,
C.
(2013) A multicenter trial of regional medical cooperation for cancer chemotherapy after the great East Japan earthquake. Gan To. Kagaku Ryoho, 40, 343-348.
-
Alcalde-Castro,
J.,
Hernandez-Gilsoul,
T.,
Dominguez-Rosado,
I.,
Chavarri-Guerra,
Y. &
Soto Perez-de-Celis,
E.
(2018) Cancer care after the 2017 Central Mexico earthquake. J. Glob. Oncol., 4, 1-4.
-
Aldrich,
D.P.
(2011) The power of people: social capital’s role in recovery from the 1995 Kobe earthquake. Nat. Hazards, 56, 595-611.
-
Aldrich,
D.P. &
Kyota,
E.
(2017) Creating community resilience through elder-led physical and social infrastructure. Disaster Med. Public Health Prep., 11, 120-126.
-
Aoki,
E.S.,
Yin,
R.,
Li,
K.,
Bhatla,
N.,
Singhal,
S.,
Ocviyanti,
D.,
Saika,
K.,
Suh,
M.,
Kim,
M. &
Termrungruanglert,
W.
(2020) National screening programs for cervical cancer in Asian countries. J. Gynecol. Oncol., 31, e55.
-
Arao,
H.,
Numata,
Y.,
Kawasaki,
Y.,
Makino,
S.,
Kobayashi,
T.,
Sakashita,
R. &
Uchinuno,
A.
(2007) Actual circumstances of treatment and nursing care for cancer patients in disaster situations: a survey of nurses who experienced the Great Hanshin-Awaji Earthquake. Jpn. J. Nurs. Sci., 4, 111-119.
-
Cabinet Office, Government of Japan
(2012) Disaster Prevention and Reconstruction from a Gender Equal Society Perspective - Lessons from the Great East Japan Earthquake - : White Paper on Gender Equality 2012. https://www.gender.go.jp/english_contents/about_danjo/whitepaper/pdf/ewp2012.pdf [Accessed: November 22, 2021].
-
Choi,
S.H. &
Hamidovic,
A.
(2020) Association between smoking and premenstrual syndrome: a meta-analysis. Front. Psychiatry, 11, 575526.
-
De Guzman,
R. &
Malik,
M.
(2019) Global cancer burden and natural disasters: a focus on Asia’s vulnerability, resilience building, and impact on cancer care. J. Glob. Oncol., 5, 1-8.
-
Dušková,
M.,
Simunkova,
K.,
Hill,
M.,
Velikova,
M.,
Kubatova,
J.,
Kancheva,
L.,
Kazihnitkova,
H.,
Hruskovicova,
H.,
Pospisilova,
H.,
Racz,
B.,
Salatova,
M.,
Cirmanova,
V.,
Kralikova,
E.,
Starka,
L. &
Parizek,
A.
(2012) Chronic cigarette smoking alters circulating sex hormones and neuroactive steroids in premenopausal women. Physiol. Res., 61, 97-111.
-
Egawa,
S.
(2021) Progress of disaster medicine during ten years after the 2011 Great East Japan arthquake. Tohoku J. Exp. Med., 253, 159-170.
-
Egawa,
S.,
Jibiki,
Y.,
Sasaki,
D.,
Ono,
Y.,
Nakamura,
Y.,
Suda,
T. &
Sasaki,
H.
(2018) The correlation between life expectancy and disaster risk. J. Disaster Res., 13, 1049-1061.
-
El Saghir,
N.S.,
Soto Perez de Celis,
E.,
Fares,
J.E. &
Sullivan,
R.
(2018) Cancer care for refugees and displaced populations: Middle East conflicts and global natural disasters. Am. Soc. Clin. Oncol. Educ. Book, 38, 433-440.
-
Gorji,
H.A.,
Jafari,
H.,
Heidari,
M. &
Seifi,
B.
(2018) Cancer patients during and after natural and man-made disasters: a systematic review. Asian Pac. J. Cancer Prev., 19, 2695-2700.
-
Gu,
F.,
Caporaso,
N.E.,
Schairer,
C.,
Fortner,
R.T.,
Xu,
X.,
Hankinson,
S.E.,
Eliassen,
A.H. &
Ziegler,
R.G.
(2013) Urinary concentrations of estrogens and estrogen metabolites and smoking in caucasian women. Cancer Epidemiol. Biomarkers Prev., 22, 58-68.
-
Habtezion, S. (2016) Gender dynamics around adaptation and disaster risk reduction. In TRAINING MODULE 2 Gender, climate change adaptation and disaster risk reduction. United Nations Development Programme, New York, NY, pp. 17-21.
-
Hasegawa,
M.,
Murakami,
M.,
Takebayashi,
Y.,
Suzuki,
S. &
Ohto,
H.
(2018) Social capital enhanced disaster preparedness and health consultations after the 2011 Great East Japan Earthquake and nuclear power station accident. Int. J. Environ. Res. Public Health, 15, 516.
-
Horiuchi,
S.,
Ozaki,
A.,
Inoue,
M.,
Aida,
J. &
Yamaoka,
K.
(2019) Relation of high social capital to preferable emotional response to news media broadcasting of natural disasters: a nationwide cross-sectional study in Japan. Tohoku J. Exp. Med., 247, 129-137.
-
Hsueh H.
(2019) A review of post-disaster recovery and reconstruction for the elderly from the individual social capital perspective. Journal of Information Studies, Interfaculty Initiative in Information Studies, The University of Tokyo, 96, 75-90.
-
JICA (Japan International Cooperation Agency)
(2014) IT Utilization in the Field of Healthcare: 2.2.1 Case examples of eHealth for MCH in developed countries, (3) “Electronic Perinatal Record Network System (Ihatov)” in Iwate Prefecture. In Project Study on Utilization of Information Technologies for Maternal and Child Health-Final Report. pp. 17-18. https://openjicareport.jica.go.jp/pdf/12148631.pdf [Accessed: November 22, 2021].
-
Kanjanvaikoon,
P.,
Gerber,
D. &
Robison,
W.R.
(2011) Long term impact of natural disaster on cervical cancer demographics. Gynecol. Oncol., 123, 446.
-
Komiyama,
M. &
Hasegawa,
K.
(2017) Comparison of preventive care for cervical cancer between Japan and western countries: a review. J. Pharma. Care Health Sys., 4, 185.
-
Koyama,
S.,
Tabuchi,
T.,
Aida,
J.,
Osaka,
K. &
Miyashiro,
I.
(2021) Determinants of increased tobacco consumption following a major disaster. Disaster Med. Public Health Prep., 15, 20-24.
-
Kyozuka,
H.,
Fujimori,
K.,
Hosoya,
M.,
Yasumura,
S.,
Yokoyama,
T.,
Sato,
A. &
Hashimoto,
K.
(2018) The Japan Environment and Children’s Study (JECS) in Fukushima Prefecture: pregnancy outcome after the Great East Japan Earthquake. Tohoku J. Exp. Med., 246, 27-33.
-
Li,
X.H.,
Qin,
L.,
Hu,
H.,
Luo,
S.,
Li,
L.,
Fan,
W.,
Xiao,
Z.,
Li,
Y.X. &
Li,
S.W.
(2011) Influence of the Wenchuan earthquake on self-reported irregular menstrual cycles in surviving women. Gynecol. Endocrinol., 27, 706-710.
-
Liu,
S.,
Han,
J.,
Xiao,
D.,
Ma,
C. &
Chen,
B.
(2010a) A report on the reproductive health of women after the massive 2008 Wenchuan earthquake. Int. J. Gynaecol. Obstet., 108, 161-164.
-
Liu,
X.,
Yang,
Y.,
Yuan,
P.,
Zhang,
X.,
Han,
Y.,
Cao,
Y. &
Xiong,
G.
(2010b) A study of the relationship between mental health and menstrual abnormalities in female middle school students from postearthquake Wenchuan. Biosci. Trends, 4, 4-8.
-
Miki,
Y.,
Tase,
T.,
Tokunaga,
H.,
Yaegashi,
N. &
Ito,
K.
(2020) Cervical cancer screening rates before and after the Great East Japan Earthquake in the Miyagi Prefecture, Japan. PLoS One, 15, e0229924.
-
Nakamura,
Y.
(2014) Maternal and child health: - work together and learn together for maternal and child health handbook. Japan Med. Assoc. J, 57, 19-23.
-
Neumayer, E. & Plümper T. (2007) The gendered nature of natural disasters: the impact of catastrophic events on the gender gap in life expectancy, 1981-2002. Ann. Assoc. Am. Geogr., 97, 551-566.
-
Nishigori,
H.,
Nishigori,
T.,
Sakurai,
K.,
Mizuno,
S.,
Obara,
T.,
Metoki,
H.,
Watanabe,
Z.,
Iwama,
N.,
Ishikuro,
M.,
Tatsuta,
N.,
Nishijima,
I.,
Sugawara,
J.,
Kuriyama,
S.,
Fujiwara,
I.,
Arima,
T.,
et al.(2017) Pregnant women’s awareness of social capital in the Great East Japan Earthquake-affected areas of Miyagi Prefecture: the Japan environment and children’s study. Disaster Med. Public Health Prep., 11, 355-364.
-
Nishigori,
H.,
Sugawara,
J.,
Obara,
T.,
Nishigori,
T.,
Sato,
K.,
Sugiyama,
T.,
Okamura,
K. &
Yaegashi,
N.
(2014) Surveys of postpartum depression in Miyagi, Japan, after the Great East Japan Earthquake. Arch. Womens Ment. Health, 17, 579-581.
-
Obi-Aso,
N.,
Ewurum,
N. &
Kenechi,
I.
(2021) Appraising the Sendai Framework: place of women in disaster risk mitigation. British Journal of Environmental Sciences, 9, 41-53.
-
Okuyama,
J.,
Funakoshi,
S.,
Seto,
S.,
Fukuda,
Y.,
Ito,
K.,
Imamura,
F. &
Izumi,
S.
(2021) Importance of psychological support for disaster-affected adolescents: 10 years after the Great East Japan Earthquake. J. Disaster Res., 16, 914-921.
-
Okuyama,
J.,
Funakoshi,
S.,
Tomita,
H.,
Yamaguchi,
T. &
Matsuoka,
H.
(2017) School-based interventions aimed at the prevention and treatment of adolescents affected by the 2011 Great East Japan Earthquake: a three-year longitudinal study. Tohoku J. Exp. Med., 242, 203-213.
-
Osaki,
Y.,
Maesato,
H.,
Minobe,
R.,
Kinjo,
A.,
Kuwabara,
Y.,
Imamoto,
A.,
Myoga,
Y.,
Matsushita,
S. &
Higuchi,
S.
(2020) Changes in smoking behavior among victims after the great East Japan earthquake and tsunami. Environ. Health Prev. Med., 25, 19.
-
Ozaki,
A.,
Horiuchi,
S.,
Kobayashi,
Y.,
Inoue,
M.,
Aida,
J.,
Leppold,
C. &
Yamaoka,
K.
(2018) Beneficial roles of social support for mental health vary in the Japanese population depending on disaster experience: a nationwide cross-sectional study. Tohoku J. Exp. Med., 246, 213-223.
-
Ozaki,
A.,
Leppold,
C.,
Sawano,
T.,
Tsubokura,
M.,
Tsukada,
M.,
Tanimoto,
T.,
Kami,
M. &
Ohira,
H.
(2017a) Social isolation and cancer management - advanced rectal cancer with patient delay following the 2011 triple disaster in Fukushima, Japan: a case report. J. Med. Case Rep., 11, 138.
-
Ozaki,
A.,
Leppold,
C.,
Tsubokura,
M.,
Tanimoto,
T.,
Saji,
S.,
Kato,
S.,
Kami,
M.,
Tsukada,
M. &
Ohira,
H.
(2016) Social isolation and cancer management after the 2011 triple disaster in Fukushima, Japan: a case report of breast cancer with patient and provider delay. Medicine (Baltimore), 95, e4027.
-
Ozaki,
A.,
Nomura,
S.,
Leppold,
C.,
Tsubokura,
M.,
Tanimoto,
T.,
Yokota,
T.,
Saji,
S.,
Sawano,
T.,
Tsukada,
M.,
Morita,
T.,
Ochi,
S.,
Kato,
S.,
Kami,
M.,
Nemoto,
T.,
Kanazawa,
Y.,
et al.(2017b) Breast cancer patient delay in Fukushima, Japan following the 2011 triple disaster: a long-term retrospective study. BMC Cancer, 17, 423.
-
Rapkin,
A.J. &
Winer,
S.A.
(2009) Premenstrual syndrome and premenstrual dysphoric disorder: quality of life and burden of illness. Expert Rev. Pharmacoecon. Outcomes Res., 9, 157-170.
-
Richards,
M.A.,
Westcombe,
A.M.,
Love,
S.B.,
Littlejohns,
P. &
Ramirez,
A.J.
(1999) Influence of delay on survival in patients with breast cancer: a systematic review. Lancet, 353, 1119-1126.
-
Rodriguez-Rabassa,
M.,
Hernandez,
R.,
Rodriguez,
Z.,
Colon-Echevarria,
C.B.,
Maldonado,
L.,
Tollinchi,
N.,
Torres-Marrero,
E.,
Mulero,
A.,
Albors,
D.,
Perez-Morales,
J.,
Flores,
I.,
Dutil,
J.,
Jim,
H.,
Castro,
E.M. &
Armaiz-Pena,
G.N.
(2020) Impact of a natural disaster on access to care and biopsychosocial outcomes among Hispanic/Latino cancer survivors. Sci. Rep., 10, 10376.
-
Sahar,
L.,
Nogueira,
L.M.,
Ashkenazi,
I.,
Jemal,
A.,
Yabroff,
K.R. &
Lichtenfeld,
J.L.
(2020) When disaster strikes: the role of disaster planning and management in cancer care delivery. Cancer, 126, 3388-3392.
-
Saito,
Y.
(2014) Progress or repetition? Gender perspectives in disaster management in Japan. Disaster Prev. Manag., 23, 98-111.
-
Sakai,
H.,
Kawamura,
C.,
Cardenas,
X. &
Ohashi,
K.
(2011) Premenstrual and menstrual symptomatology in young adult Japanese females who smoke tobacco. J. Obstet. Gynaecol. Res., 37, 325-330.
-
Sakai,
H. &
Ohashi,
K.
(2021) Effects of past environmental tobacco smoke exposure on the menstrual cycle and menstrual phase-related symptoms: a cross-sectional study. J. Obstet. Gynaecol. Res., 47, 243-253.
-
Sharma,
T. &
Khapre,
M.
(2021) Exposure of second hand smoke in women and children: a narrative review. J. Family Med. Prim. Care, 10, 1804-1807.
-
Sugawara,
J.,
Hoshiai,
T.,
Sato,
K.,
Tokunaga,
H.,
Nishigori,
H.,
Arai,
T.,
Okamura,
K. &
Yaegashi,
N.
(2016) Impact of the Great East Japan Earthquake on regional obstetrical care in Miyagi Prefecture. Prehosp. Disaster Med., 31, 255-258.
-
Taguchi,
K. & Natsuhara K.
(2014) Social capital and residentsʼ consultation behavior for medical checkups and/or cancer screening: research in a provincial area of Japan. Journal of the Japanese Red Cross Akita College of Nursing and the Japanese Red Cross Junior College of Akita, 19, 17-26.
-
Takeda,
T.,
Tadakawa,
M.,
Koga,
S.,
Nagase,
S. &
Yaegashi,
N.
(2013a) Premenstrual symptoms and posttraumatic stress disorder in Japanese high school students 9 months after the great East-Japan earthquake. Tohoku J. Exp. Med., 230, 151-154.
-
Takeda,
T.,
Tadakawa,
M.,
Koga,
S.,
Nagase,
S. &
Yaegashi,
N.
(2013b) Relationship between dysmenorrhea and posttraumatic stress disorder in Japanese high school students 9 months after the Great East Japan Earthquake. J. Pediatr. Adolesc. Gynecol., 26, 355-357.
-
Trofor,
A.C.,
Papadakis,
S.,
Lotrean,
L.M.,
Radu-Loghin,
C.,
Eremia,
M.,
Mihaltan,
F.,
Driezen,
P.,
Kyriakos,
C.N.,
Mons,
U.,
Demjen,
T.,
Nogueira,
S.O.,
Fernandez,
E.,
Tountas,
Y.,
Przewozniak,
K.,
McNeill,
A.,
et al.(2019) Knowledge of the health risks of smoking and impact of cigarette warning labels among tobacco users in six European countries: findings from the EUREST-PLUS ITC Europe Surveys. Tob. Induc. Dis., 16, A10.
-
Tsunoda,
H.,
Yoshino,
R. &
Yokoyama,
K.
(2008) Components of social capital and socio-psychological factors that worsen the perceived health of Japanese males and females. Tohoku J. Exp. Med., 216, 173-185.
-
Uebayashi,
M.,
Kishi,
E.,
Sato,
M.,
Abe,
A.,
Kuroda,
Y.,
Sato,
M.,
Nakaita,
I.,
Fukushima,
F.,
Yokoyama,
Y. &
Hirano,
K.
(2014) Problems with maternal and child health activities during the Great East Japan Earthquake in Iwate Prefecture. Journal of the Faculty of Nursing, Iwate Prefectural University, 16, 19-28.
-
UNDRR (United Nations Office for Disaster Risk Reduction)
(2007) Hyogo Framework for Action 2005-2015: Building the Resilience of Nations and Communities to Disasters. Extract from the final report of the World Conference on Disaster Reduction. https://www.unisdr.org/2005/wcdr/intergover/official-doc/L-docs/Hyogo-framework-for-action-english.pdf [Accessed: November 22, 2021].
-
UNDRR (United Nations Office for Disaster Risk Reduction)
(2015) Sendai Framework for Disaster Risk Reduction 2015-2030. https://www.preventionweb.net/files/43291_sendaiframeworkfordrren.pdf [Accessed: November 22, 2021].
-
Utada,
M.,
Chernyavskiy,
P.,
Lee,
W.J.,
Franceschi,
S.,
Sauvaget,
C.,
de Gonzalez,
A.B. &
Withrow,
D.R.
(2019) Increasing risk of uterine cervical cancer among young Japanese women: comparison of incidence trends in Japan, South Korea and Japanese-Americans between 1985 and 2012. Int. J. Cancer, 144, 2144-2152.
-
Verna,
L.,
Cortellini,
A.,
Giusti,
R.,
Ficorella,
C. &
Porzio,
G.
(2019) Cancer care after natural disaster: different countries, similar problems. J. Glob. Oncol., 5, 1-2.
-
Yamamoto,
Y.
(2007) Disaster management in the acute phase. Japan Med. Assoc. J., 50, 72-79.
-
Yokoyama,
Y.,
Otsuka,
K.,
Kawakami,
N.,
Kobayashi,
S.,
Ogawa,
A.,
Tannno,
K.,
Onoda,
T.,
Yaegashi,
Y. &
Sakata,
K.
(2014) Mental health and related factors after the Great East Japan earthquake and tsunami. PLoS One, 9, e102497.
-
Yoshida H.
(2021a) Maternal and Child Health History and Public Health System at the Time of Disasters in Japan. In Lessons Learned from the Great East Japan Earthquake - Birth Outcomes in a Catastrophe in a Highly Aged Society. Springer, Singapore, pp. 1-12.
-
Yoshida H.
(2021b) Personal Health Record (PHR) System for Maternal and Child Health Care in Disaster. In Lessons Learned from the Great East Japan Earthquake - Birth Outcomes in a Catastrophe in a Highly Aged Society. Springer, Singapore, pp. 79-88.