Introduction
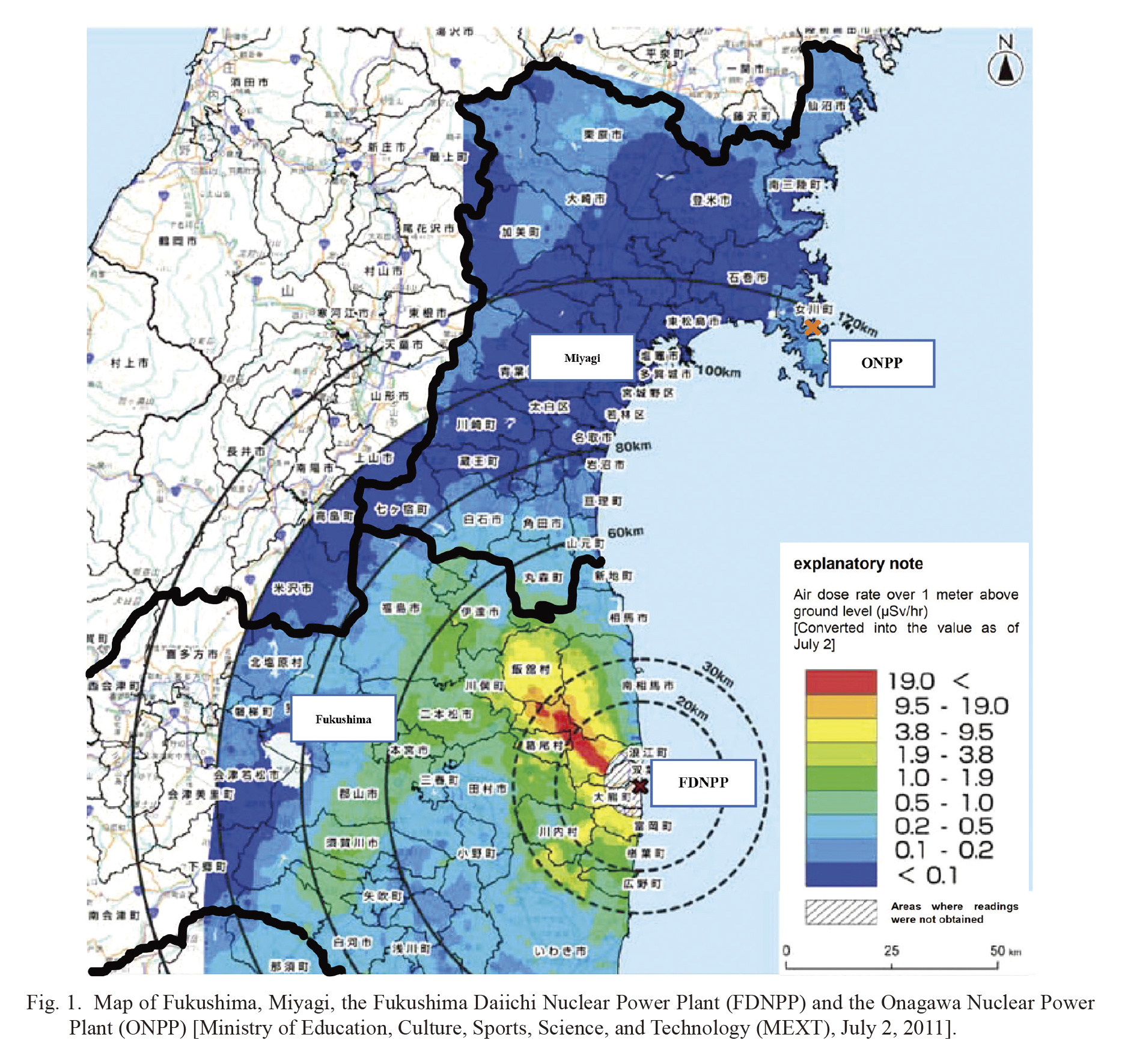
On March 11, 2011, the Great East Japan Earthquake and Tsunami occurred, during which a large tsunami damaged the nuclear reactors at the Fukushima Daiichi Nuclear Power Plant (FDNPP) (Shibahara 2011, 2012). As a result of the damage, large amounts of radioactive isotopes were released from the damaged reactors at the FDNPP (Suzuki et al. 2019; Sun et al. 2020, 2021). As a result, radioactive nuclides were widely deposited on the ground not only in Fukushima but also from northern Japan to eastern Japan outside of Fukushima (UNSCEAR, United Nations Scientific Committee on the Effects of Atomic Radiation 2013). After the nuclear accident, the Japanese government implemented various countermeasures; however, for a while, they were only provided for the areas near the FDNPP and residents in Fukushima. As the measures taken by the Japanese government were not implemented at locations other than Fukushima immediately after the accident, many residents outside Fukushima, including those in southern Miyagi, also became extremely anxious about radiation exposure. Miyagi is adjacent to the northern part of Fukushima and is located approximately 50-120 km from the FDNPP (Nuclear Regulation Authority 2011) (Fig. 1).
At the time of the FDNPP accident, the Japanese government’s recommended evacuation area was all territory within a 30 km range of the FDNPP. Nevertheless, some residents in southern Miyagi, located within 80 km of the FDNPP, also evacuated out of fear of the radiation effects from the nuclear accident, although some residents who chose not to evacuate were also extremely worried about the effects. As the Onagawa Nuclear Power Plant (ONPP) was installed in the Miyagi Prefecture (Fig. 1), nuclear disaster drills had been conducted Onagawa Town, Ishinomaki City and Miyagi prefectural office once a year before the FDNPP accident. In November 2009 and 2010, some radiological technologists who belong to the Miyagi Association of Radiological Technologists (MART) participated in the nuclear disaster drill to learn how to respond to the residents’ anxieties in the event of a nuclear accident at Ishinomaki City (Miyagi Prefectural Government 2010). Those drills were performed in Fukushima Prefecture, but did not include to respond to the residents’ anxieties (Fukushima Prefectural Government 2010).
Radiologic technologists are healthcare worker who specializes in imaging tests, such as X-ray, Magnetic Resonance Imaging (MRI), and Computerized Tomography (CT) scans, performed primarily in diagnostic capacities. They must obtain specialized education—such as radiography, anatomy, physiology, radiation physics, radiation protection, radiation therapy, psychology, and ethics—and pass a national examination to receive a license to practice as radiologic technologists. They also consider radiation exposure of patients and staff (Chida et al. 2010a, b; Kato et al. 2012, 2017, 2021; Morishima et al. 2018; Nemoto and Chida 2020; Haga et al. 2020a; Kawauchi et al. 2021; Inaba et al. 2021; Endo et al. 2021; Matsunaga et al. 2021), perform radiation management work (Morishima et al. 2016a, b; Kato et al. 2019a, b; Ishii et al. 2019; Inaba et al. 2020a, b), and are responded to the patients’ anxieties on radiation exposure in the medical field. Therefore, we think that radiologic technologists can respond to residents’ anxieties in nuclear disaster.
Immediately after the FDNPP accident, from March to April 2011, we participated as counselor for phone consultations regarding radiation risk at the Miyagi Prefectural Office (Yashima and Chida 2014). On May 18, 2011, it was found that radioactive cesium exceeding the standard value was detected in beef, and we learned that a municipality in southern Miyagi requested Miyagi Prefecture to introduce persons to explain for residents. We proposed the municipality to conduct consultation activities with the residents on May 2011. We also proposed to another municipality on July 2011, which was nearby the municipality, to conduct consultation activities for residents’ anxieties. Each local government and MART member discussed to cope with the stress of residents due to the nuclear accident. Through discussion, we decided to conduct individual consultations with pregnant women and parents of infants.
We had conducted consultation activities for residents based on the knowledge and experience of medical exposure consultation cultivated over many years. We also had participated in training course on radiation emergency medicine so far. However, probably because we did not expect that food contamination like this would actually occur, and did not have the opportunity to listen to expert lectures on internal exposure and food intake standards, it was very difficult understanding. We held a study session before consultation activities in local governments to check the health and environmental impacts by disaster radiation exposure.
Since the occurrence of the FDNPP accident, radiologists, nurses, and public health nurses have published many reports on individual consultations with residents inside and outside of Fukushima (Fujii et al. 2015; Orita et al. 2015; Murakami et al. 2017a), but few have been reported by the radiologic technologists (Yashima and Chida 2014). As radiologic technologists, we engaged in individual consultations with pregnant women and infants’ parents in southern Miyagi near Fukushima accident and conducted a survey about these activities within one year of the FDNPP accident. In this paper, we review and report the survey data retrospectively.
Methods
From June 2011 to February 2012, we conducted individual face-to-face consultations on the radiation effects of the nuclear accident in two local governments in southern Miyagi. The activities were conducted at the facilities of the local governments, and radiologic technologists were in charge of the consultations.
Let two local governments be Municipality A and Municipality B. In Municipality A, prior to the individual consultations, we gave a basic lecture on radiation exposure (e.g., background radiation, radiation exposure from medical exams, radiation health effects, and radioactive materials), and conducted risk communication activities individually for pregnant women and infants’ parents. We did not ask and answer questions when we gave a lecture, and answered questions during individual consultation. The contents of the basic lecture included types of radiation, background radiation, human exposure to ionizing radiation, environmental radiation monitoring, health effects of radiation exposure, probabilistic and deterministic effects, causes of cancer, food radioactivity control, Chernobyl nuclear accident, radioactive iodine, and radioactive cesium. The activity period was approximately three months, from June 2011 to August 2011. In Municipality B, we did not give a basic lecture, and conducted individual consultations for pregnant women and parents with babies under one year of age. The activity period was approximately six months, from August 2011 to February 2012. We consulted with the municipalities and targeted pregnant women and parents with infants for individual consultations, taking into account the level of anxiety about disaster radiation exposure and the health effects of the stress. We set the time for each individual consultation to 30 min, but we responded to the questions from the parents without being bound by the set time. At each location, a temporary daycare center was set up by the municipality to make it possible to talk with the participants without having to worry about the infants.
After the end of the individual consultations, we conducted a questionnaire survey on the activities. The questionnaire surveys were conducted using a de-identified document that was anonymous and did not include age and sex. Questionnaire survey items were prepared in discussion with each municipality. Therefore, the questionnaire items differ depending on the municipality. Questionnaire surveys were voluntary, and agreement was obtained by answering the questionnaires. We have made clear the participants’ rights regarding their withdrawal of consent (Dubois et al. 2021).
Ethics approval
This study protocol was approved by the Ethics Review Committee of the Miyagi Cancer Society on October 2, 2018 (No. 1805). This study is a retrospective survey.
Municipality A
The questionnaire survey items in Municipality A were as follows;
A- Q1. Did you understand the contents of risk communication activity today?
(a) Understood, (b) Almost understood, (c) Didn’t understand much, (d) Didn’t understand at all, (e) Others ____________________, (f) No response.
A- Q2. How have you felt about participating in today’s activities?
(a) Relieved, (b) Relieved a little, (c) Slightly anxious, (d) Anxious,
(e) Others ________________________________________, (f) No response.
A- Q3. If you feel anxious, what do you feel anxious about?
________________________________________
A- Q4. We would like to continue the communication activities with today’s structure and content. What do you think about it?
(a) Today’s structure and content are good, (b) The different structures are good ______________________________, (c) No response.
A- Q5. What administrative efforts do you think are necessary to eliminate your anxiety?
________________________________________
Municipality B
The questionnaire survey items in Municipality B were as follows;
B- Q1. How was the time length for the communication activity today?
(a) Very good, (b) Good, (c) Neither, (d) Not very good, (e) Not good.
________________________________________
B- Q2. How easy was it to understand the communication activity today?
(a) Very easy, (b) Easy, (c) Neither, (d) Not very easy, (e) Not easy.
________________________________________
B- Q3. In terms of the contents of communication activities, how applicable (good) are the references to your daily life?
(a) Very good, (b) Good, (c) Neither, (d) Not very good, (e) Not good.
________________________________________
B- Q4. What was your level of satisfaction with the communication activity today?
(a) Very good, (b) Good, (c) Neither, (d) Not very good, (e) Not good.
________________________________________
B- Q5. If you have any other comments or opinions about today’s activities, please add below.
________________________________________
Results
We conducted communication activities on radiation risks four times in Municipality A and six times in Municipality B. See Tables 1 and 2 for the details.
Municipality A
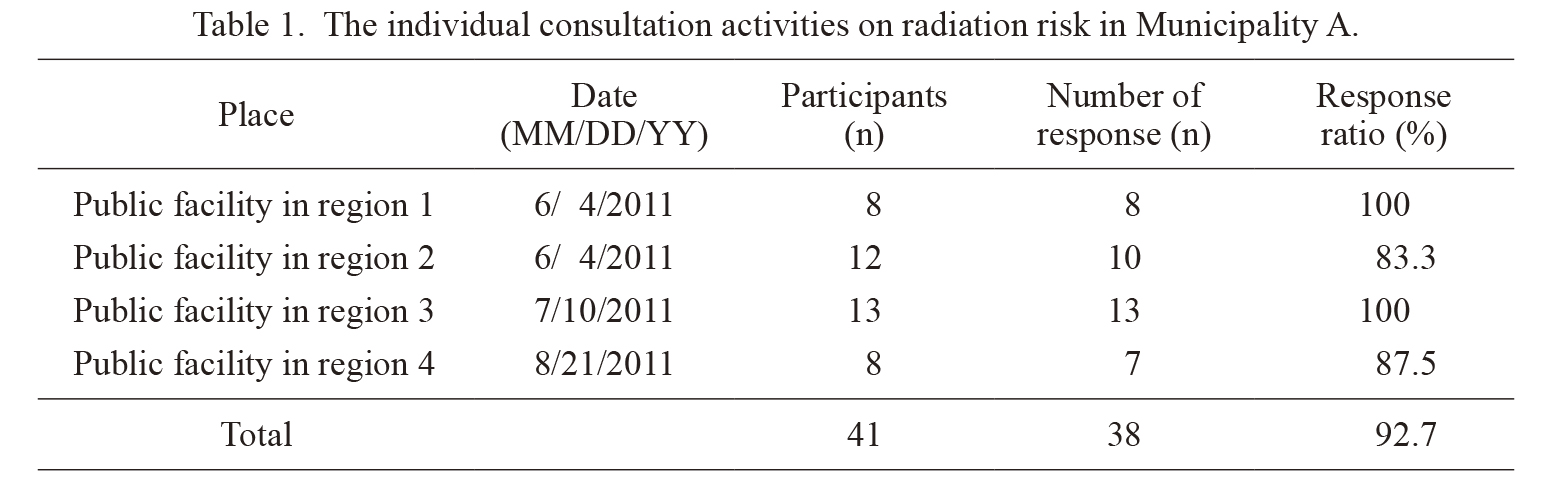
Pregnant women, parents, or mothers of 41 families participated in the lecture and communication activities with radiologic technologists held in Municipality A. The number of responses to the questionnaire survey was 38, and the response ratio was 92.7% (Table 1). The results of each answer from A-Q1 to A-Q5 are shown in Fig. 2.
In A-Q1, the answer “Understood” was 31%, “Almost understood” was 63% (Fig. 2A). Regarding the answers to A-Q2, 26% answered “Relieved” and 50% answered “Relieved a little” (Fig. 2B). In A-Q3, we asked the participants about anxiety factors. Of the 38 total responses, 22 responses were obtained, indicating that 57.9% of the respondents felt anxiety. The anxiety factors were 32% for “Child health effect,” 18% for “Food safety,” and 36% for “Radiation effects on the environment” (Fig. 2C). We have extracted the focuses of opinions from 22 responders to summarize the A-Q3 results in Fig. 2C, considering that A-Q3 is free writing. Examples of comments on anxiety factors are presented below:
・“Will parents, i.e., we and our children, have symptoms of radiation effects some years later?”
・“Of course, daily life (i.e., washing, ventilation, etc.) is uneasy, and I am also concerned about the food sold at the supermarket, and about eating out.”
・“Since the house backs up to a mountain, I would normally like to make it possible for my children to play a lot. However, I am worried about radiation, so I cannot let the children play there.”
・“I am worried about my child’s DNA (whether the DNA is destroyed). Can my child have children?”
・“I am uneasy about vegetables from the affected areas or the vegetables that I made myself because there has not been any investigation of their potential radioactive substances after all.”
・“Today, my anxiety has been largely resolved. However, I am anxious because I do not know about radiation. I believe information that is generally reported.
In A-Q4, we obtained 81% approval when we asked the participants for pros and cons on the structure and contents that conducted lectures and individualized communication activities (Fig. 2D). The opinions of the answer “The different structure is good” (14%) are presented below:
・“It would be nice if we (all parents) could casually discuss our requests with specialists, municipality officials, and teachers at the nursery.”
・“Please do study sessions and lectures on the effects on children etc.”
・“It may be better to exchange information in a group that we created by ourselves.”
・“I want to listen to the contents of other people’s questions in an activity with a few more participants.”
In A-Q5, the answers about what seems to be necessary to eliminate the anxiety about the effects of radiation were mainly “Decontamination,” “Radiation control measures,” “Provide accurate and detailed information on radiation effects,” “Measure radiation dose details” and “Consultation meeting (individual)” (Fig. 2E). We have extracted the focuses of opinions from 38 responders to summarize the A-Q5 results in Fig. 2E, considering that A-Q5 is free writing. Here are some opinions of participants in A-Q5:
・“I want you to decontaminate a schoolyard and a nursery garden. It is inconvenient that I cannot go out with my children, and I am also anxious about letting my children play outside.”
・“I think that municipality takes the situation more seriously about radiation pollution and putting it into action for children will give a sense of security to people raising children in the future. If I leave this as it is, I think the number of children will decrease.”
・“Please publish it without hiding anything. Thank you in advance. I want to continue raising children here all the time. Please do your best for the future. Thank you very much.”
・“The individual communication activity was good because it was easy to ask about uneasy things.”
・“It is to measure radiation dose more finely (soil, water, food).”
It means that radiation levels on drinking water, home grown vegetables, fields, school routes, parks, schoolyards can be measured and known. They wanted to know the radiation doses that affect their lives, the future safety of children.
・“I want to have an opportunity to be able to listen to more about the municipality’s way of thinking, such as what measures are being taken at nursery schools and elementary schools.”
・“I want you to measure daily the presence or absence of radioactive material of vegetables and ingredients which use for school lunch and show numerical value. (Because it’s every day, I am worried.)”
・“It would be grateful to have a communication activity regularly as short intervals as possible (once every month or two months).”
・“I would like these communication activities and lectures to be held for the general public (in addition to pregnant women and parents of infants).”
Municipality B
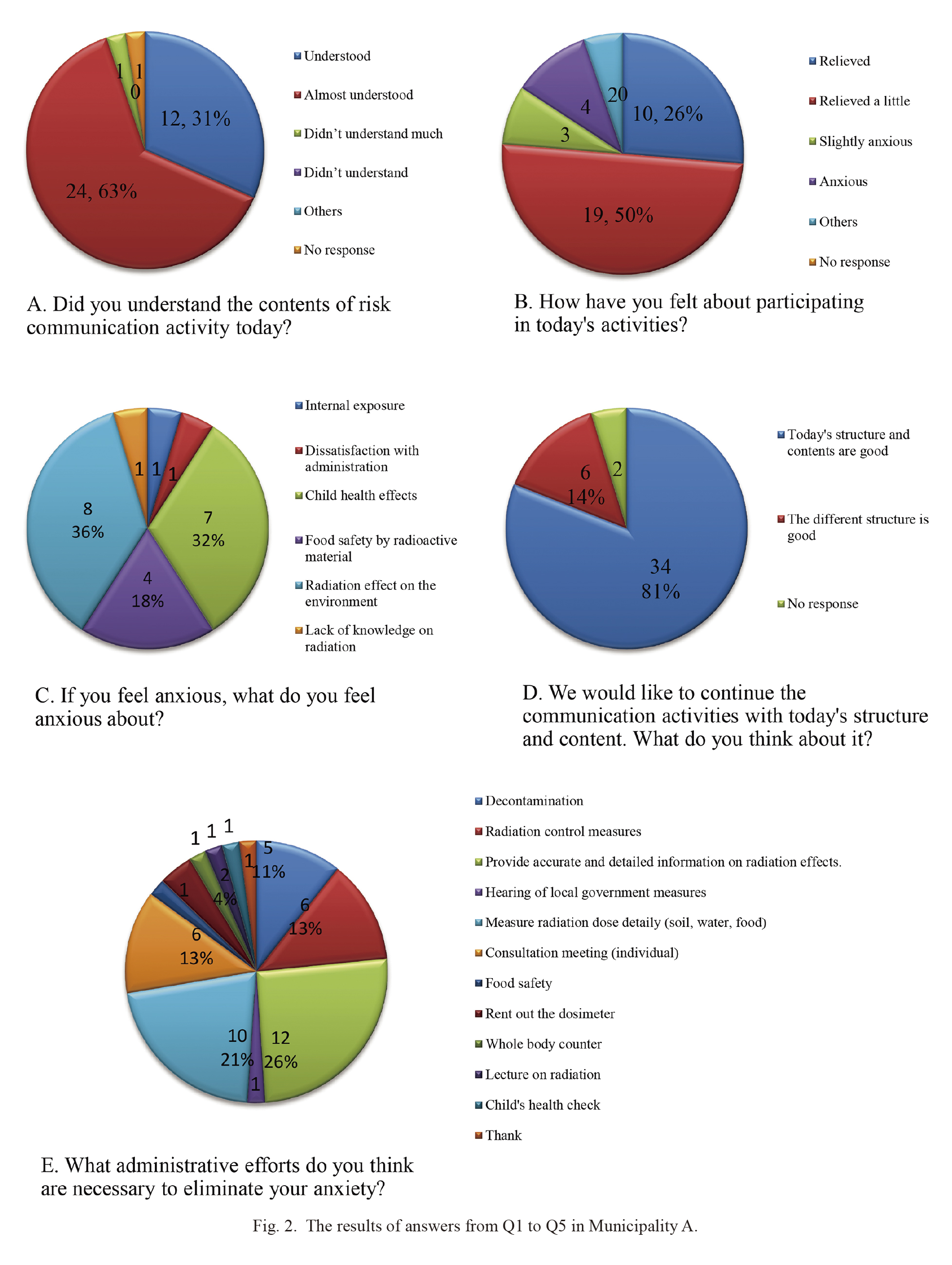
Pregnant women, parents, or mothers from 53 families participated in the communication activities held in Municipality B. There were 53 responses to the questionnaire survey, and the response ratio was 100% (Table 2).
The results of answers from B-Q1 to B-Q5 are shown in Fig. 3. In B-Q1, the answer “Very good” was 55%, “Good” was 34% (Fig. 3A). Some comments or opinions about “Very good” or “Good” are as follows:
・“Because I had you explain what I wanted to know in detail.”
・“It was good to be able to ask many questions.”
・“I think each one was good.”
・“They listened to me until I was satisfied.”
・“I was allowed to ask questions without minding the time, so I could ask and stay calm.”
The comments or opinions about “Neither” are as follows:
・“I want some more time. Half-hour is short.”
・“Because we cannot end decades of talk in one day.”
・“I thought it was better not to provide a limit in the time.”
In B-Q2, 47% answered “Very good” and 41% answered “Good” concerning the understandability of the contents in the communication activity (Fig. 3B). Some comments about “Very good” or “Good” are as follows:
・“It was explained so that I, an amateur, could understand it.”
・“It was easy to understand because they answered my question politely.”
・“I could understand even the radiation dose units that I did not understand very much.”
・“It was easy to understand because they explained using figures and tables.”
・“I had you talk in plain language.”
An answer “Neither” was 8%, the comments or opinions in the answer are as follows:
・“There is no precedent on the effects from the FDNPP accident, so there is no accuracy on the contents of this activity.”
・“There was an easy-to-understand part and a part that I thought was difficult to understand.”
・“I think it was easy to understand, but because it's hard to understand about the radiation originally.”
There were no comments in an answer, “Not very good.” The comment in an answer “Not good” was “Because the content of discourse in communication activity was vague.”
In B-Q3, the answer to the question of whether the content to be helpful in daily life was 51% for “Very good,” 38% for “Good,” and 11% for “Neither.” There was no answer “Not very good” and “Not good” (Fig. 3C). Some comments about “Very good” or “Good” are as follows:
・“I was relieved because I could confirm from the contents and the charts during the communication activity that natural radiation exists in general.”
・“I found out that the dose of ‘0.5 μSv’ is not a value that actually affects humans.”
・“Because I was able to hear about things to pay attention to in my daily life and about places where it is easier for radioactive cesium to accumulate.”
・“I was relieved because I had you tell me in a professional opinion what I had been worried about from before.”
・“I used to be too sensitive to what we eat (we haven’t eaten the food from Fukushima). However, it was explained to me why the food being distributed was safe, so I could confirm the safety of food, which made me feel a little better.”
・“I was able to know more about external exposure and internal exposure (food etc.).”
In B-Q3, some comments about “Neither” are follows:
・“Because I was not concerned about food.”
・“Because I had already read a book about radioactive contamination and decontamination of both food and soil by myself beforehand; I had already taken measures.”
・“I thought that I wanted to be a little careful because cesium easily sticks to leaves and soil.”
In B-Q4, the response to the degree of satisfaction regarding the communication activities was 57% for “Very good,” 34% for “Good,” 7% for “Neither” and one for “Not good.” There was no answer “Not very good” (Fig. 3D). Some comments about “Very good” or “Good” are as follows:
・“It was very good because I could ask directly what I wanted to ask.”
・“At the lectures where a large number of people participated, it was not easy to ask, even if I had any questions. I was glad that I could consult individually and ask questions.”
・“I wasn’t able to consult with anyone, so I had been at a loss alone. Because I was able to consult today, a huge weight has been lifted off my shoulders.”
In B-Q4, the comment for “Neither” was “I wanted to know future measures against radiation,” and for “Not good” was “I want to discuss with you again.”
In B-Q5, thirty-eight out of fifty-three participants filled comments and opinions. The breakdown is shown in Fig. 3E. The comments on the continuation of the activities were 21%, and 45% of the comments indicated that they were relieved or helped. Some comments or opinions were entered as follows:
・“I had no chance to consult about my baby, so you were a big help. I want you to do this activity again.”
・“I hope such a day when family, friends and people can live with peace of mind without much influence of radiation. I want you to check because the radioactivity of vegetables in the field is the most worrying! I hope peace of mind comes back to our daily diet.”
・“I want you to continue this activity in the future. I also want the elderly to have this activity.”
・“The individual consultation was very good because I could ask what I wanted to ask. I was relieved of because I could talk about what I was always worried and wondered, etc. I thought that it would be better to expand the subject a bit more than just the parents with children under one year old (e.g., parents with children under 7 years old). Not only this time; I want you to continue such a communication activity for a long time. I am worried because I think the impact will last long, even if the accident converges in the future. I think that it is difficult, but I want you to increase the targeted personal communication activities a little more.”
・“I was given some polite explanations, but they were still specialized and difficult. I understood that natural background radiation is present in the environment, and that even if we live here, we do not immediately get sick or increase the risk of carcinogenesis. However, if we have any risk even a little, I am as a parent worried about my children. Through this activity, I thought it was necessary to collect information by myself and live while thinking about my children’s health.”
・“I want you to tell me, because I want to know where we can get thyroid cancer screening by ourselves and how much the cost is.”
Discussion
After the FDNPP accident occurred in 2011, we cooperated with the two local governments to conduct individual consultation activities with pregnant women and parents with infants (mostly mothers only) to reduce their anxieties. The activities in Municipality A took place within half a year of the FDNPP accident. The activities in Municipality B were conducted about half a year to one year after the accident.
In Municipality B, there were 26 participants on the first day of activities; on the last day of activities, the number of participants decreased significantly to two. Although the number of participants decreased, the opinion stated in the questionnaire survey indicated concern about children’s health, which was not different from the main concerns expressed when the activity started. As for the decrease in the number of participants, we thought this might be due to the influence of the amount of time that had elapsed since that accident occurred.
In the activities, we were able to obtain many opinions from the participants of both municipalities that the individual consultation activity was good. We think that individual consultation through dialog was extremely effective. This result is in agreement with a previous study (Murakami et al. 2017a). The activity time was set at 30 min, but communication activities continued until the participants were satisfied, even if the set time was exceeded, which has also been seen as good. A previous study (Fujii et al. 2015) reported negative feedback regarding activity times that were limited to 15 min. We found the same result in this study. Another point of interest is that, in addition to what was planned, the participants requested measurement of the environment, soil, water, and food. We believe that this is because Miyagi Prefectural Government and municipal governments could not carry out tests of the water, food, and soil responding to requests from residents due to the various impacts of the tsunami disaster, although they wished they could have provided a quicker response.
In 2015, the Third United Nations World Conference on Disaster Reduction was held. During the conference, the Sendai Framework for Disaster Risk Reduction 2015-2030 was adopted (UNDRR, United Nations Office for Disaster Risk Reduction 2015). This framework established that “Understanding disaster risks and sharing of information” is clearly stated at the top of its “4 Priorities for Action.” We believe that the survey results showed the importance of providing and sharing information on potential risks to reduce actual disaster risks and anxieties of the participants (Egawa 2021; Fujii et al. 2021). In 2021, World Health Organization published guidance on research methods for health emergency and disaster risk management. The guidance describes how to plan, conduct, and report various studies under diverse circumstances. Ethics in research is mentioned in Chapter 3 of the Guidance (Dubois et al. 2021). As described in the guidelines, emergencies and disasters have a major impact on people’s health and livelihoods. We think that ethical point is assessing its contribution to social good, potential to save lives and reduce suffering, and the significance of knowledge outcomes.
In a previous study conducted at Fukushima (Orita et al. 2015; Murakami et al. 2017b), participants who are residents outside Fukushima were deeply afflicted with various fears of the radiation exposure effects from the FDNPP accident, and we recognized that the response would be necessary for wide range of population in a nuclear disaster. In previous studies (Orita et al. 2015; Fujii et al. 2015; Murakami et al. 2017a), radiologists, public health nurses, and nurses’ activities were reported in risk communications with residents. We, radiologic technologists, in daily work, have performed medical imaging exams (Chida et al. 2006; Matsunaga et al. 2017, 2019, 2021), manage the quality control of medical imaging equipment including dosimetry (Chida et al. 2011, 2013; Haga et al. 2017; Morishima et al. 2018, 2019; Kato et al. 2019c; Haga et al. 2020b), and explain radiation exposure due to radiology exams for patients (Chida et al. 2009; SCoR, The Society & College of Radiographer 2019). We sometimes also respond to patients’ anxiety about medical exposure, and attempt to reduce any anxiety (Chida et al. 2010a, b). In this study, we believe that radiologic technologists can also be specialists in dealing with residents’ anxieties in a nuclear disaster just like radiologists, public health nurses, and nurses.
Every time a nuclear accident has occurred, affected residents suffer from heartbreaking uneasiness and anxiety. In September 1999, Japan experienced the Tokai Village Nuclear Accident, which was classified as an International Nuclear and Radiological Event Scale (INES) Level 4 (IAEA, International Atomic Energy Agency 1999; Sato 2003; Hore-Lacy et al. 2009; Yaginuma 2013). In that event, two people died from accidental radiation exposure. Although the scale of that accident varies greatly from that of the FDNPP, the anxieties and concerns of residents near the nuclear fuel processing facility were almost the same as those of residents after the FDNPP accident. As radiologic technologists who understand people’s anxieties due to the 1999 JCO accident, we participated in the nuclear disaster drill for responding to anxieties about medical radiation exposure and accident-induced radiation exposure that was offered before the FDNPP accident occurred. The participation appears to have been beneficial to our training and to our actions taken following the accident. In the 2009 drill, responding to residents’ anxieties was included, and MART members participated that. We got the opportunity to learn about nuclear disaster exposure. In 2010, we participated with local health nurses, and learned that residents made it easier to talk about their anxieties.
This study does have some limitations. First, the activity area was limited, and the study involved a relatively small number of participants. However, we believe that the strength of this study is hearing directly from citizens to learn their opinions about the relevant communications.
In conclusion, after the FDNPP accident, we cooperated with the two local governments to conduct individual consultation activities and a questionnaire survey with pregnant women and parents of infants. As a result of the survey, we were able to obtain reliable evaluations and various opinions on individual consultation activities. The results of this study indicate that radiologic technologists must respond to the anxieties of disaster radiation exposure as soon as possible in the event of a nuclear disaster and carry out individual communication activities to contribute to the alleviation of residents’ anxieties.