Abstract
Asthma and atopic dermatitis are common among schoolchildren. The Great East Japan Earthquake of 2011 caused serious damage to buildings and infrastructure as well as the total or partial collapse of many hospitals and medical clinics. The aim of this study was to examine the association between recurrence or exacerbation (recurrence/exacerbation) of asthma or atopic dermatitis at the time of disaster and allergic symptoms several years later in schoolchildren. A cross-sectional survey was conducted via a parent-administered questionnaire between 2013 and 2015 in Miyagi Prefecture, northeast Japan. We analyzed the data of 2,399 schoolchildren with a diagnosis of asthma and 2,107 with a diagnosis of atopic dermatitis. Among those who had experienced recurrence/exacerbation of their symptoms soon after the disaster, the prevalence of later wheezing and eczema was 71.2% (N = 195) and 81.9% (N = 379), respectively. Recurrence/exacerbation of allergic symptoms just after the disaster was positively associated with wheezing (odds ratio, OR 6.54, 95% confidence interval, 95% CI 4.94-8.67) and eczema (OR 8.12, 95% CI 6.25-10.55) several years later. Disasters might have long-term effects on the allergy symptoms of children. It is necessary to prepare for prevention of recurrence/exacerbation, to treat allergic symptoms, and to support children to continue their allergy treatments and daily care when a disaster strikes.
Introduction
Asthma and atopic dermatitis are common in children (Lai et al. 2009; Futamura et al. 2011). Although childhood asthma and atopic dermatitis often resolve with age, previous reports have indicated that severe wheezing and eczema in childhood are likely to be persistent into adulthood (Margolis et al. 2014; Kim et al. 2016; McGeachie et al. 2016; Fuchs et al. 2017). Therefore, it is necessary to identify and address the symptoms of asthma and atopic dermatitis in early childhood.
The Great East Japan Earthquake of 2011 and subsequent tsunami caused such serious damage in northeast Japan where lifelines were not restored until more than one month after the disaster. During this time, people living in the affected area were unable to carry out many activities of daily living, including taking a bath. Moreover, 128/147 (87.1%) hospitals and 627/1,626 (38.6%) medical clinics in Miyagi Prefecture suffered total or partial collapse, and some limited their services to outpatients for several months after the disaster (Ministry of Health, Japan 2011).
Yamaoka et al. (2011) reported that in children aged 0-16 years, the symptoms worsened just after the Great East Japan Earthquake in 22% of those with asthma and in 55% of those with atopic dermatitis, and that 14% of those with allergies ran out of their regular prescription medications. Ishikuro et al. (2017) reported that experiencing the tsunami and staying in an evacuation area after the Great East Japan Earthquake were associated with a high prevalence of atopic dermatitis among boys, and the experience of having their house destroyed and moving between houses was associated with a high prevalence of asthma among girls. Although these studies are highly valuable, the data were collected at a specific point in time after the disaster, and there are no data regarding the allergy symptoms of children who did not visit clinics or medical institutions, and no long-term data.
We have previously reported the prevalence of wheezing and eczema as symptoms of asthma and atopic dermatitis (Kikuya et al. 2015), and also the prevalence among schoolchildren from a survey conducted in the southern part of Miyagi Prefecture (Miyashita et al. 2015). The aim of this study was to examine the associations between recurrence or exacerbation (recurrence/exacerbation) that occurred during the Great East Japan Earthquake and allergic symptoms several years later in schoolchildren who had a diagnosis of asthma or atopic dermatitis.
Methods
Design
This report was based on the Tohoku Medical Megabank Organization (ToMMo) Child Health Study, a cross-sectional observation of schoolchildren conducted in 28 of the 35 municipalities in Miyagi Prefecture: Higashimatsushima, Iwanuma, Kakuda, Kami, Kawasaki, Kesennuma, Kurihara, Marumori, Minamisanriku, Misato, Murata, Natori, Ogawara, Ohira, Onagawa, Osaki, Osato, Shibata, Shichigahama, Shichikashuku, Shikama, Shiroishi, Taiwa, Tome, Wakuya, Watari, Yamamoto, and Zao (Kikuya et al. 2015). Schoolchildren were examined in the 2nd, 4th, 6th, and 8th grades and the study area was changed every two years from 2012 to 2015, in the 28 municipalities (Fig. 1). Therefore, there was very little duplication of the survey targets.
Ethical approval was obtained from the Institutional Review Board of Tohoku University Graduate School of Medicine on September 24, 2012 (No. 2012-1-278). A completed and returned questionnaire was considered to indicate consent to participate in the investigation.
Study population and data collection
Questionnaires were distributed to 62,895 schoolchildren in cooperation with the Board of Education of each municipality and 624 public schools. The schoolchildren took the questionnaires home for their parents or guardians to complete within two weeks, and 1,369 (39.1%), 4,080 (32.0%), 7,197 (25.6%), and 4,374 (23.7%) questionnaires were returned for Survey 2012, Survey 2013, Survey 2014, and Survey 2015, respectively, for a total of 17,020 (collection rate 27.1%). Grade-specific response rates were 32.9%, 31.7%, 28.1%, and 21.5% for the 2nd, 4th, 6th, and 8th grades, respectively.
After excluding 1,925 questionnaires that had missing data and responses for schoolchildren outside the target grades, 15,095/62,895 questionnaires (24.0%) were available for all four years. Of these, we collected information for 13,799 schoolchildren in Surveys 2013-2015, because in Survey 2012 we did not ask about symptoms in the aftermath of the Great East Japan Earthquake. Among these 13,799 schoolchildren, 2,399 schoolchildren who had a diagnosis of asthma and 2,107 with atopic dermatitis were included in the study (Fig. 2).
Questionnaire items
To assess symptoms of asthma and eczema at the survey point, we adopted the Japanese version of the International Study of Asthma and Allergies in Childhood (ISAAC) questionnaire (Nishima and Odajima 2002), an international standardized epidemiological questionnaire used to assess allergic symptoms (Asher et al. 1995). Wheezing was defined as a positive response to the item “Has your child had wheezing or whistling in the chest in the last 12 months?” (Lai et al. 2009). Severe wheezing was defined as wheezing with ≥ 4 attacks, or ≥ 1 night per week of sleep disturbance from wheezing, or wheezing affecting the speech (Lai et al. 2009). Eczema was defined as a positive response to the item “Has your child had an itchy rash at any time during the past 12 months?”, which was further refined by “Has this itchy rash at any time affected any of the following places: the folds of the elbows, behind the knees, in front of the ankles, under the buttocks, or around the neck, ears, or eyes?” Severe eczema was defined as eczema accompanied by sleep disturbance ≥ 1 night per week (Odhiambo et al. 2009). We added the following questions regarding allergic symptoms and treatment conditions for asthma and atopic dermatitis that occurred in the aftermath of the disaster: “Did your child, diagnosed with asthma, have their asthma treatment interrupted for more than one month after the disaster?”, “Did your child, diagnosed with asthma, have recurrent or exacerbated symptoms within 1 year after the disaster?”, and “Did your child, diagnosed with atopic dermatitis, have their treatment for atopic dermatitis interrupted for more than one month after the disaster?”, and “Did your child, diagnosed with atopic dermatitis, have recurrent or exacerbated symptoms within 1 year after the disaster?”.
Also included in the questionnaire were items regarding birth year, birth month, history of hospitalisation, history of being diagnosed with an allergic disease, the Japanese language version of the Strengths and Difficulties Questionnaire (SDQ) (Matsuishi et al. 2008), and disaster experience. A history of hospitalization was defined as hospitalization for any reason, including asthma, atopic dermatitis, or other diseases or symptoms. The SDQ is a brief questionnaire composed of 25 items designed to investigate mental health difficulties in the daily and social lives of children (Goodman 1997; Matsuishi et al. 2008). An SDQ total difficulties score greater than 16/40 points was considered to be in the “high need” range (Matsuishi et al. 2008). The questionnaire item regarding disaster experience was “At the time of the disaster, please choose all that your child experienced”, with the choices provided as “earthquake”, “tsunami”, “both”, or “none”.
Data analysis
For descriptive statistics, we calculated the prevalence of wheezing and eczema symptoms and then used the chi-square test and one-way analysis of variance (ANOVA) for analysis.
To examine associations of recurrence or exacerbation of asthma or atopic dermatitis within a year after the Great East Japan Earthquake and the symptoms of asthma or atopic dermatitis at the survey point, we performed multivariate logistic regression analysis adjusted for statistically significant variables in single regression analyses and computed the odds ratios (ORs) at several years after the disaster. The variable “coastal municipality” was defined by the location of the public school affiliation of the children. If the school was located in a coastal municipality, i.e., Higashimatsushima, Iwanuma, Kesennuma, Minamisanriku, Natori, Onagawa, Shichigahama, Watari, or Yamamoto, “coastal municipality” was coded as “yes”. P values less than 0.05 were considered statistically significant. All statistical analyses were performed using SAS (version 9.4; SAS Institute Inc., Cary, NC, USA).
Results
Among the 2,399 schoolchildren with a diagnosis of asthma and the 2,107 with a diagnosis of atopic dermatitis, almost all (N = 2,365, 98.6% and 2,081, 98.7%, respectively) had experienced an earthquake, and 714 schoolchildren had diagnoses of both asthma and atopic dermatitis.
Table 1 lists the number of schoolchildren with wheezing and severe wheezing at each survey point. There was a significant association of wheezing with age, school grade at the survey point, and recurrence/exacerbation of asthma symptoms in the aftermath of the disaster. 195 (71.2%) schoolchildren had wheezing at the survey point among 274 who had experienced recurrence/exacerbation of asthma symptoms. Severe wheezing was significantly associated with age, school grade, clinical range of SDQ score, and the recurrence/exacerbation of asthma symptoms in the aftermath of the disaster.
Table 2 lists the number of schoolchildren with eczema and severe eczema at each survey point. There was a significant association of eczema with survey year, age, school grade, history of hospitalisation, clinical range of SDQ score, experience of tsunami, school location at the survey point, and recurrence/exacerbation of atopic dermatitis symptoms in the aftermath of the disaster. 379 (81.9%) schoolchildren had eczema at the survey point among 463 who had experienced recurrence/exacerbation of atopic dermatitis symptoms. There was a significant association of severe eczema with survey year, age, school grade, sex, clinical range of SDQ, school location at the survey point, and recurrence/exacerbation of atopic dermatitis symptoms in the aftermath of the disaster. The proportion of schoolchildren living in coastal municipalities showed a decrease with time [Total: 804/2,107 (38.2%), Survey 2013: 375/603 (62.2%), 2014: 292/964 (30.3%), 2015: 137/540 (25.4%), P < 0.0001]; whereas the proportion of 2nd grade schoolchildren among the survey respondents [Total: 461/2,107 (21.9%), Survey 2013: 139/603 (23.1%), 2014: 215/964 (22.3%), 2015: 107/540 (19.8%), P =0.5826] and the proportion of schoolchildren under no treatment among those with eczema [Total: 290/947 (30.6%), Survey 2013: 89/300 (30.0%), 2014: 130/413 (31.5%), 2015: 71/234 (30.3%), P = 0.8695] showed no increase with time.
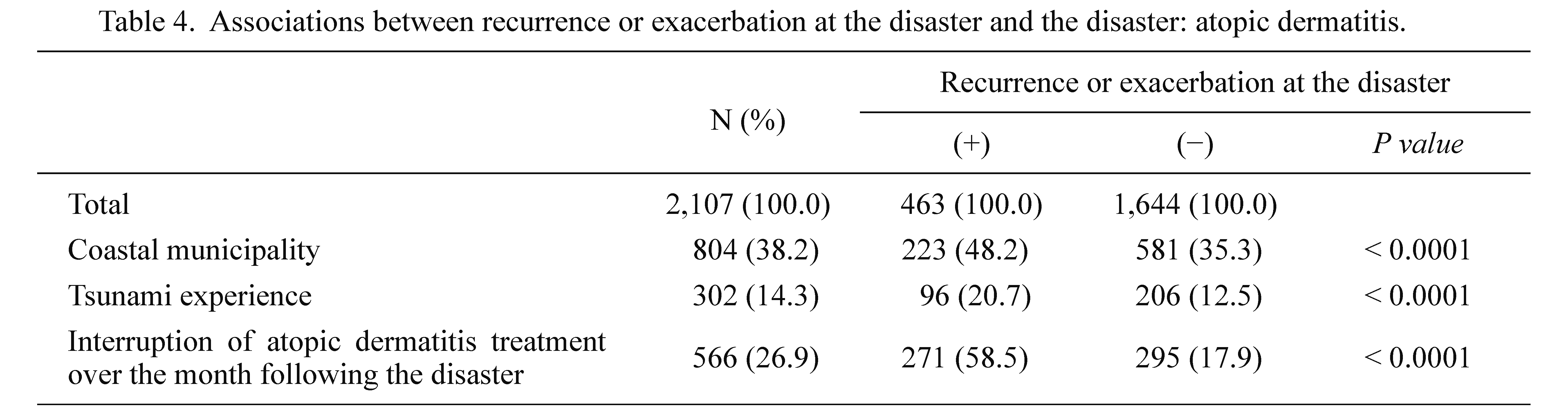
We confirmed significantly positive associations of experience of tsunami, living in a coastal municipality, and interruption of treatment following the disaster with recurrence/exacerbation (Tables 3 and 4). Of the 274 schoolchildren with recurrence/exacerbation of asthma, 111 (40.5%) had interruption of their asthma treatment over the month following the disaster (Table 3). Of the 463 schoolchildren with recurrence/exacerbation of atopic dermatitis 271 (58.5%) had interruption of their treatment for atopic dermatitis over the month following the disaster (Table 4).
Among the 2,399 schoolchildren with asthma, children in the “high need” range on the SDQ were 152/860 (17.7%) schoolchildren in the coastal municipalities, 293/1,539 (19.0%) in the inland municipalities, 72/364 (19.8%) of schoolchildren with tsunami experience, and 373/2,035 (18.3%) without tsunami experience (P = 0.4098, P = 0.5119, respectively) (Table 5).
Among the 2,107 schoolchildren with atopic dermatitis, 144/804 (17.9%) schoolchildren in the coastal municipalities, 241/1,303 (18.5%) in the inland municipalities, 66/302 (21.9%) schoolchildren with tsunami experience, and 319/1,805 (17.7%) without tsunami experience were in the “high need” range on the SDQ (P = 0.7356, P = 0.0818, respectively) (Table 5).
The multivariate logistic regression analysis revealed that wheezing and severe wheezing at the survey point were positively associated with recurrence/exacerbation of symptoms in the aftermath of the disaster, and the odds ratio of wheezing and recurrence/exacerbation of asthma symptoms was 6.54 (95% confidence interval, 95% CI 4.94-8.67) (Table 6).
There was a positive association of eczema and severe eczema at the survey point with recurrence/exacerbation of symptoms in the aftermath of the disaster, and the odds ratio of eczema and recurrence/exacerbation of atopic dermatitis symptoms was 8.12 (95% CI 6.25-10.55) (Table 7).
The odds ratio of wheeze and severe wheeze a few years after the disaster and the experience of recurrence/exacerbation showed no significant difference between with and without directive exposure to the disaster by such as experience of tsunami and living in a coastal municipality (Table 6). In contrast, the odds ratio of eczema and severe eczema after the experience of recurrence/exacerbation were higher among schoolchildren with experience of tsunami and who lived in a coastal municipality (Table 7).
Discussion
We examined associations between the recurrence/exacerbation of symptoms within a year after the Great East Japan Earthquake and the symptoms of asthma or atopic dermatitis several years after the disaster in schoolchildren who had a diagnosis of asthma or atopic dermatitis.
The prevalence of wheezing and severe wheezing was significantly higher in younger children. The fact that allergic symptoms were more frequent in younger children has already been pointed out (Futamura et al. 2011), and the results among children with a diagnosis of asthma were also similar to results from previous reports among schoolchildren in the southern area of Miyagi Prefecture (Miyashita et al. 2015). One of the reasons for the high prevalence of wheezing and severe wheezing among younger children might be that respiratory function is underdeveloped in early childhood (Martinez et al. 1995; Stein et al. 1999).
The prevalence of eczema was slightly higher in 2013, which might be partly because the study area comprised mainly coastal municipalities in that year. However, the prevalence of severe eczema was slightly lower in 2013, which may be due to a random error because of the small number of schoolchildren in this group (N = 22). In line with our previous paper (Kuniyoshi et al. 2018), the present analyses demonstrated that the “high need” range on the SDQ was positively associated with eczema and severe eczema (Table 2). Severe eczema itself was associated with high total SDQ score and sleep disturbance due to itchy, scratching skin. Severe wheezing might also cause mental health problems, including affective disorders, anxiety disorders, and pervasive developmental disorders (Baglioni et al. 2016).
The finding of the higher prevalence of “high need” level difficulty after the earthquake and tsunami (Kikuya et al. 2015) indicates that after a disaster, children with severe wheezing and severe eczema need support for mental difficulties in daily life.
The prevalence and adjusted odds ratios of wheezing and severe wheezing were significantly higher in schoolchildren who had recurrence/exacerbation in the aftermath of the disaster compared with those who had no recurrence/exacerbation at that time. The prevalence of exacerbation of asthma symptoms was previously found to be higher among patients whose treatment with inhaled corticosteroids was interrupted during the disaster compared with those who continued their treatment in the time following the Great East Japan Earthquake (Fukuhara et al. 2012). There were fewer exacerbations of asthma in adult patients who continued their asthma management during the Chuetsu Earthquake in 2004 than in those who did not continue (Suzuki et al. 2007). Several other reports have also reported that the exacerbation of asthma symptoms might have been caused by interruption of treatment just after the Great East Japan Earthquake (Takakura et al. 1997; Ohkouchi et al. 2013; Yamanda et al. 2013), and another found a positive association between a history of asthma and the severity of respiratory symptoms after the 1997 Haze Disaster in Indonesia (Kunii et al. 2002). In studies of the World Trade Center Disaster of September 11, 2001, the prevalence or diagnosis of asthma in children who had been exposed to dust clouds was also high a few years after the disaster (Thomas et al. 2008; Trye et al. 2018). These results suggest that among children, symptoms of asthma recur easily or are exacerbated and prolonged by exposure to disasters. Therefore, the effect on asthma symptoms after the Great East Japan Earthquake might also be long-term, especially among schoolchildren who experienced recurrence/exacerbation of symptoms in the aftermath of the disaster.
The prevalence of eczema or severe eczema was significantly higher in schoolchildren of younger age and in those with a history of hospitalisation. Possible reasons for the high prevalence among younger children could include underdeveloped skin barrier function in early childhood or pre-existing health problems associated with skin disorders (Garg and Silverberg 2015; Weidinger and Novak 2016). It is necessary that after a disaster, the symptoms of atopic dermatitis should be attended to immediately in young children and children with a history of hospitalisation.
The prevalence of severe eczema was significantly low in schoolchildren from schools in coastal municipalities. There was a difference in prevalence of a few percent among the school locations, although the classification of school location as coastal or inland among the municipalities was itself vague. For these reasons, it is difficult to conclude that the prevalence of severe eczema was slightly lower in coastal municipalities than in inland municipalities.
The ORs of wheezing, severe wheezing, eczema, and severe eczema were significantly higher in schoolchildren who had recurrence/exacerbation of symptoms just after the disaster compared with schoolchildren who had no recurrence/exacerbation. Almost all schoolchildren experienced the Great East Japan Earthquake, which caused serious damage to lifelines and medical services throughout Miyagi Prefecture. We confirmed that exposure to the disaster, including experiencing the tsunami and living in coastal municipality, might be strongly associated with recurrence/exacerbation within 1 year after the Great East Japan Earthquake, and that exposure to the disaster and recurrence/exacerbation might be also associated with allergic symptoms experienced several years after the disaster.
A previous study based on medical records reported that atopic dermatitis patients with interruption of treatment experienced exacerbation of their symptoms after the Great East Japan Earthquake (Ozawa et al. 2015). In the present study, schoolchildren with recurrence/exacerbation of asthma or atopic dermatitis in the aftermath of the disaster also had interrupted treatment at more than one month after the disaster. Although poor adherence to treatment for asthma or atopic dermatitis might also have affected treatment interruption (Krejci-Manwaring et al. 2007; Suzuki et al. 2011; Torrelo et al. 2013; Murota et al. 2015), the shortage or absence of drugs and the impossibility of bathing following damage to lifelines might be the main reasons for treatment interruption just after the Great East Japan Earthquake. Previous studies have also indicated that the persistence of asthma and atopic dermatitis are prolonged in children with severe symptoms (Kim et al. 2016; Fuchs et al. 2017).
This study has several limitations. First, the response rate for the questionnaire was only 24.0%. Although no differences in age or sex were found among the years of the survey (P > 0.5), our results may have been affected by self-selection bias; e.g., parents or caregivers whose child had wheezing or eczema might have been more likely to respond. Second, as our results relied exclusively on a retrospective, parent-administered questionnaire, we might not have been able to grasp accurate symptoms, particularly those from just after the disaster. Third, it is difficult to determine a causal relationship between wheezing and eczema at several years after the Great East Japan Earthquake and recurrence/exacerbation of asthma and atopic dermatitis that occurred just after the disaster because we conducted cross-sectional surveys rather than longitudinal cohort studies. However, the strengths of our study are that it is one of the few studies with a large sample size that targeted mid- and long-term allergy symptoms among schoolchildren living in a region seriously damaged by a natural disaster. Therefore, we consider that the results of the present study indicate the mid- and long-term influences of the Great East Japan Earthquake on allergic diseases in children.
In conclusion, significant association was found between recurrence/exacerbation of asthma and atopic dermatitis within one year after the Great East Japan and the symptoms of asthma and atopic dermatitis at the survey point several years after the disaster. This finding indicates that preparation is necessary to prevent recurrence/exacerbation, and the importance of identifying and treating allergic symptoms, and supporting children to continue their allergy treatments and daily care in the immediate aftermath of a natural disaster.
Acknowledgments
This work was supported by the MEXT Tohoku Medical Megabank Project and the Japan Agency for Medical Research and Development (AMED), Nos. and JP20km0105001. We wish to express our appreciation to the Prefectural Board of Education in Miyagi and the Municipal Boards of Education in Higashimatsushima, Iwanuma, Kakuda, Kami, Kawasaki, Kesennuma, Kurihara, Marumori, Minamisanriku, Misato, Murata, Natori, Ogawara, Ohira, Onagawa, Osaki, Osato, Shibata, Shichigahama, Shichikashuku, Shikama, Shiroishi, Taiwa, Tome, Wakuya, Watari, Yamamoto, and Zao. We would also like to thank Mr. Shoji Tanaka for technical assistance.
Conflict of Interest
The authors declare no conflict of interest.
References
-
Asher,
M.I.,
Keil,
U.,
Anderson,
H.R.,
Beasley,
R.,
Crane,
J.,
Martinez,
F.,
Mitchell,
E.A.,
Pearce,
N.,
Sibbald,
B.,
Stewart,
A.W.,
Strachan,
D.,
Weiland,
S.K. &
William,
H.C.
(1995) International Study of Asthma and Allergies in Childhood (ISAAC): rationale and methods. Eur. Respir. J., 8, 483-491.
-
Baglioni,
C.,
Nanovska,
S.,
Regen,
W.,
Spiegelhalder,
K.,
Feige,
B.,
Nissen,
C.,
Reynolds,
C.F. &
Riemann,
D.
(2016) Sleep and mental disorders: a meta-analysis of polysomnographic research. Psychol. Bull., 142, 969-990.
-
Fuchs,
O.,
Bahmer,
T.,
Rabe,
K.F. &
von Mutius,
E.
(2017) Asthma transition from childhood into adulthood. Lancet Respir. Med., 5, 224-234.
-
Fukuhara,
A.,
Sato,
S.,
Uematsu,
M.,
Misa,
K.,
Nikaido,
T.,
Inokoshi,
Y.,
Fukuhara,
N.,
Wang,
X.,
Kanazawa,
K.,
Tanino,
Y.,
Ishida,
T. &
Munakata,
M.
(2012) Impacts of the 3/11 disaster in fukushima on asthma control. Am. J. Respir. Crit. Care Med., 186, 1309-1310.
-
Futamura,
M.,
Ohya,
Y.,
Akashi,
M.,
Adachi,
Y.,
Odajima,
H.,
Akiyama,
K. &
Akasawa,
A.
(2011) Age-related prevalence of allergic diseases in Tokyo schoolchildren. Allergol. Int., 60, 509-515.
-
Garg,
N. &
Silverberg,
J.I.
(2015) Epidemiology of childhood atopic dermatitis. Clin. Dermatol., 33, 281-288.
-
Goodman,
R.
(1997) The Strengths and Difficulties Questionnaire: a research note. J. Child Psychol. Psychiatry, 38, 581-586.
-
Ishikuro,
M.,
Matsubara,
H.,
Kikuya,
M.,
Obara,
T.,
Sato,
Y.,
Metoki,
H.,
Isojima,
T.,
Yokoya,
S.,
Kato,
N.,
Tanaka,
T.,
Chida,
S.,
Ono,
A.,
Hosoya,
M.,
Yokomichi,
H.,
Yamagata,
Z.,
et al. (2017) Disease prevalence among nursery school children after the Great East Japan earthquake. BMJ Glob. Health, 2, e000127.
-
Kikuya,
M.,
Miyashita,
M.,
Yamanaka,
C.,
Ishikuro,
M.,
Sato,
Y.,
Obara,
T.,
Metoki,
H.,
Nakaya,
N.,
Nagami,
F.,
Tomita,
H.,
Kiyomoto,
H.,
Sugawara,
J.,
Hozawa,
A.,
Fuse,
N.,
Suzuki,
Y.,
et al. (2015) Protocol and research perspectives of the ToMMo Child Health Study after the 2011 Great East Japan Earthquake. Tohoku J. Exp. Med., 236, 123-130.
-
Kim,
J.P.,
Chao,
L.X.,
Simpson,
E.L. &
Silverberg,
J.I.
(2016) Persistence of atopic dermatitis (AD): a systematic review and meta-analysis. J. Am. Acad. Dermatol., 75, 681-687 e11.
-
Krejci-Manwaring,
J.,
Tusa,
M.G.,
Carroll,
C.,
Camacho,
F.,
Kaur,
M.,
Carr,
D.,
Fleischer,
A.B. Jr.,
Balkrishnan,
R. &
Feldman,
S.R.
(2007) Stealth monitoring of adherence to topical medication: adherence is very poor in children with atopic dermatitis. J. Am. Acad. Dermatol., 56, 211-216.
-
Kunii,
O.,
Kanagawa,
S.,
Yajima,
I.,
Hisamatsu,
Y.,
Yamamura,
S.,
Amagai,
T. &
Ismail,
I.T.
(2002) The 1997 haze disaster in Indonesia: its air quality and health effects. Arch. Environ. Health, 57, 16-22.
-
Kuniyoshi,
Y.,
Kikuya,
M.,
Miyashita,
M.,
Yamanaka,
C.,
Ishikuro,
M.,
Obara,
T.,
Metoki,
H.,
Nakaya,
N.,
Nagami,
F.,
Tomita,
H.,
Hozawa,
A.,
Tsuji,
I.,
Kure,
S.,
Yaegashi,
N.,
Yamamoto,
M.,
et al. (2018) Severity of eczema and mental health problems in Japanese schoolchildren: The ToMMo Child Health Study. Allergol. Int., 67, 481-486.
-
Lai,
C.K.,
Beasley,
R.,
Crane,
J.,
Foliaki,
S.,
Shah,
J. &
Weiland,
S.;
International Study of Asthma and Allergies in Childhood Phase Three Study Group
(2009) Global variation in the prevalence and severity of asthma symptoms: phase three of the International Study of Asthma and Allergies in Childhood (ISAAC). Thorax, 64, 476-483.
-
Margolis,
J.S.,
Abuabara,
K.,
Bilker,
W.,
Hoffstad,
O. &
Margolis,
D.J.
(2014) Persistence of mild to moderate atopic dermatitis. JAMA Dermatol., 150, 593-600.
-
Martinez,
F.D.,
Wright,
A.L.,
Taussig,
L.M.,
Holberg,
C.J.,
Halonen,
M. &
Morgan,
W.J.
(1995) Asthma and wheezing in the first six years of life. The Group Health Medical Associates. N. Engl. J. Med., 332, 133-138.
-
Matsuishi,
T.,
Nagano,
M.,
Araki,
Y.,
Tanaka,
Y.,
Iwasaki,
M.,
Yamashita,
Y.,
Nagamitsu,
S.,
Iizuka,
C.,
Ohya,
T.,
Shibuya,
K.,
Hara,
M.,
Matsuda,
K.,
Tsuda,
A. &
Kakuma,
T.
(2008) Scale properties of the Japanese version of the Strengths and Difficulties Questionnaire (SDQ): a study of infant and school children in community samples. Brain Dev., 30, 410-415.
-
McGeachie,
M.J.,
Yates,
K.P.,
Zhou,
X.,
Guo,
F.,
Sternberg,
A.L.,
Van Natta,
M.L.,
Wise,
R.A.,
Szefler,
S.J.,
Sharma,
S.,
Kho,
A.T.,
Cho,
M.H.,
Croteau-Chonka,
D.C.,
Castaldi,
P.J.,
Jain,
G.,
Sanyal,
A.,
et al. (2016) Patterns of growth and decline in lung function in persistent childhood asthma. N. Engl. J. Med., 374, 1842-1852.
-
Ministry of Health, Japan
(2011) The reports of the situation of damage to medical institution by the Great East Japan Earthquake 2011. https://www.mhlw.go.jp/stf/shingi/2r9852000001yxlj-att/2r9852000001yy9a.pdf [Accessed: October 19, 2021] (in Japanese).
-
Miyashita,
M.,
Kikuya,
M.,
Yamanaka,
C.,
Ishikuro,
M.,
Obara,
T.,
Sato,
Y.,
Metoki,
H.,
Nakaya,
N.,
Nagami,
F.,
Tomita,
H.,
Kiyomoto,
H.,
Sugawara,
J.,
Hozawa,
A.,
Fuse,
N.,
Suzuki,
Y.,
et al. (2015) Eczema and asthma symptoms among schoolchildren in coastal and inland areas after the 2011 Great East Japan Earthquake: The ToMMo Child Health Study. Tohoku J. Exp. Med., 237, 297-305.
-
Murota,
H.,
Takeuchi,
S.,
Sugaya,
M.,
Tanioka,
M.,
Onozuka,
D.,
Hagihara,
A.,
Saeki,
H.,
Imafuku,
S.,
Abe,
M.,
Shintani,
Y.,
Kaneko,
S.,
Masuda,
K.,
Hiragun,
T.,
Inomata,
N.,
Kitami,
Y.,
et al. (2015) Characterization of socioeconomic status of Japanese patients with atopic dermatitis showing poor medical adherence and reasons for drug discontinuation. J. Dermatol. Sci., 79, 279-287.
-
Nishima,
S. &
Odajima,
H.
(2002) Prevalence of childhood allergic diseases in Japan using International Study of Asthma and Allergies in Childhood (ISAAC) phase I protocol. Japanese Journal of Pediatric Allergy and Clincal Immunology, 16, 207-220 (in Japanese).
-
Odhiambo,
J.A.,
Williams,
H.C.,
Clayton,
T.O.,
Robertson,
C.F. &
Asher,
M.I.;
ISAAC Phase Three Study Group
(2009) Global variations in prevalence of eczema symptoms in children from ISAAC Phase Three. J. Allergy Clin. Immunol., 124, 1251-1258 e23.
-
Ohkouchi,
S.,
Shibuya,
R.,
Yanai,
M.,
Kikuchi,
Y.,
Ichinose,
M. &
Nukiwa,
T.
(2013) Deterioration in regional health status after the acute phase of a great disaster: respiratory physicians’ experiences of the Great East Japan Earthquake. Respir. Investig., 51, 50-55.
-
Ozawa,
M.,
Honda,
M.,
Ochiai,
Y.,
Ozawa,
H.,
Numata,
I.,
Kagimoto,
Y.,
Ohnami,
K.,
Chikama,
R.,
Kuikata,
N.,
Asano,
M. &
Aiba,
S.
(2015) Survey of the disease conditions and the daily living conditions of atopic dermatitis patients after the Great East Japan Earthquake. J.Environ. Dermatol. Cutan. Allergol., 9, 34-40 (in Japanese).
-
Stein,
R.T.,
Sherrill,
D.,
Morgan,
W.J.,
Holberg,
C.J.,
Halonen,
M.,
Taussig,
L.M.,
Wright,
A.L. &
Martinez,
F.D.
(1999) Respiratory syncytial virus in early life and risk of wheeze and allergy by age 13 years. Lancet, 354, 541-545.
-
Suzuki,
K.,
Hasegawa,
T.,
Iguchi,
S.,
Ota,
K.,
Sakagami,
T.,
Gejyo,
F. &
Suzuki,
E.
(2007) The impact of the Chuetsu earthquake on asthma control. Allergol. Int., 56, 179.
-
Suzuki,
T.,
Saito,
I.,
Adachi,
M.,
Shimbo,
T. &
Sato,
H.
(2011) Influence of patients’ adherence to medication, patient background and physicians’ compliance to the guidelines on asthma control. Yakugaku Zasshi, 131, 129-138.
-
Takakura,
R.,
Himeno,
S.,
Kanayama,
Y.,
Sonoda,
T.,
Kiriyama,
K.,
Furubayashi,
T.,
Yabu,
M.,
Yoshida,
S.,
Nagasawa,
Y.,
Inoue,
S. &
Iwao,
N.
(1997) Follow-up after the Hanshin-Awaji earthquake: diverse influences on pneumonia, bronchial asthma, peptic ulcer and diabetes mellitus. Intern. Med., 36, 87-91.
-
Thomas,
P.A.,
Brackbill,
R.,
Thalji,
L.,
DiGrande,
L.,
Campolucci,
S.,
Thorpe,
L. &
Henning,
K.
(2008) Respiratory and other health effects reported in children exposed to the World Trade Center disaster of 11 September 2001. Environ. Health Perspect., 116, 1383-1390.
-
Torrelo,
A.,
Ortiz,
J.,
Alomar,
A.,
Ros,
S.,
Pedrosa,
E. &
Cuervo,
J.
(2013) Health-related quality of life, patient satisfaction, and adherence to treatment in patients with moderate or severe atopic dermatitis on maintenance therapy: the CONDA-SAT study. Actas Dermosifiliogr., 104, 409-417.
-
Trye,
A.,
Berger,
K.I.,
Naidu,
M.,
Attina,
T.M.,
Gilbert,
J.,
Koshy,
T.T.,
Han,
X.,
Marmor,
M.,
Shao,
Y.,
Giusti,
R.,
Goldring,
R.M. &
Trasande,
L.
(2018) Respiratory health and lung function in children exposed to the World Trade Center disaster. J. Pediatr., 201, 134-140 e6.
-
Weidinger,
S. &
Novak,
N.
(2016) Atopic dermatitis. Lancet, 387, 1109-1122.
-
Yamanda,
S.,
Hanagama,
M.,
Kobayashi,
S.,
Satou,
H.,
Tokuda,
S.,
Niu,
K. &
Yanai,
M.
(2013) The impact of the 2011 Great East Japan Earthquake on hospitalisation for respiratory disease in a rapidly aging society: a retrospective descriptive and cross-sectional study at the disaster base hospital in Ishinomaki. BMJ Open, 3, e000865.
-
Yamaoka,
A.,
Abe,
H.,
Watanabe,
Y.,
Kakuta,
H.,
Umebayashi,
H.,
Inagaki,
T.,
Abukawa,
D.,
Yanagida,
N.,
Minoura,
T.,
Morikawa,
M.,
Kondo,
N. &
Miura,
K.
(2011) The questionnaire for caregivers of allergic children in the Great East Japan Earthquake. Japanese Journal of Pediatric Allergy and Clinical Immunology, 25, 801-809 (in Japanese).