Abstract
Shoulder pain is more common among survivors of natural disasters than the general population. This study aimed to examine the occurrence of shoulder pain, especially the association between prior and later shoulder pain episodes, in survivors living in coastal areas severely damaged by the Great East Japan Earthquake (GEJE) (n = 1,821) over a period of 5 years. The presence of shoulder pain was assessed at 2 (first period), 4 (second period), and 7 (third period) years after the disaster. Multiple logistic regression analyses were performed to assess the association between shoulder pain during the first and second periods and shoulder pain during the third period. Shoulder pain in the first period was significantly associated with shoulder pain in the third period [adjusted odds ratio (OR) 5.93; 95% confidence interval (CI) 4.06-8.66]. Furthermore, shoulder pain in the first and second periods was significantly associated with shoulder pain in the third period. With the absence of shoulder pain in both the first and second periods used as the reference, adjusted ORs for the presence of shoulder pain during each period and both periods were 4.58 (95% CI 3.17-6.62) and 15.54 (95% CI 8.38-28.84), respectively (P for trend < 0.001). Thus, prior shoulder pain was significantly associated with shoulder pain after 5 years among GEJE survivors, and the association was stronger as the number of prior shoulder pain episodes increased. This expertise should be shared with other expert teams to address the affected people and prepare for future disasters.
Introduction
Disasters have an enormous impact on people’s lives, specifically survivors, and the long-lasting impacts gradually affect people’s health, not only physically but also mentally. The Great East Japan Earthquake (GEJE) was a catastrophe accompanied by a giant tsunami and the indirect effects of a nuclear power plant accident on March 11, 2011, resulting in severe damage, particularly to the northeastern coastal areas of Japan (Ishigaki et al. 2013).
Musculoskeletal pain often increases the socio-economic cost due to factors such as increased absenteeism and presenteeism, early retirement, and use of medical services (Phillips 2009). Shoulder pain, along with back and knee problems, is the third most common musculoskeletal complaint in the general population (Walker-Bone et al. 2004; Gill et al. 2020). Shoulder problems are often chronic, usually lead to disability in the community, and have a considerable impact on daily activities (Macfarlane et al. 1998; Gill et al. 2020). Among people with shoulder pain, 17.7% had difficulty with basic daily activities, while 21.4% had difficulty with complex daily activities (Institute of Medicine 2011). Addressing shoulder pain is key to allowing people to lead a normal life.
Most pain syndromes after earthquakes or natural disasters are due to traumatic events in the musculoskeletal system during the acute phase (a few weeks after the occurrence) (Angeletti et al. 2012). The prevalence of musculoskeletal pain had been reported to be higher even during the recovery phase (a month after the occurrence) after the GEJE (Angeletti et al. 2012), and almost half of the survivors experienced musculoskeletal pain at multiple sites (Yabe et al. 2019a). Pain has been afflicting survivors before and after the GEJE, including during the recovery phase, making it difficult for them to return to the lifestyle they had before the GEJE. Furthermore, multiple conditions such as psychological disorders, physical inactivity, and functional disabilities attributable to the impact of life-threatening stress and changes in living conditions resulting from the devastation of home environments and public health systems impact chronic pain among survivors in the recovery phase (Angeletti et al. 2012; Yabuki et al. 2015). As several factors influence musculoskeletal pain in GEJE survivors, a consideration of such situations is quite important while taking care of these survivors.
A cross-sectional study showed that similarly to the general population, the knee and surrounding regions, low back, and shoulder were the three most frequent chronic pain sites after 1.5 years among GEJE survivors (Yabuki et al. 2015). Subjective shoulder pain after the GEJE had been reported by a prospective cohort study to be significantly associated with sleep disturbances (Hagiwara et al. 2017a), pain in other body parts (Hagiwara et al. 2021), and by a cross-sectional study to be related to the living status, economic hardship, and sleep disturbance (Hagiwara et al. 2017b). However, no study has investigated changes in shoulder pain over a long period after natural disasters. Although some changes between pre- and post-disaster lifestyle status have been reported among survivors, these changes could affect the later occurrence of shoulder pain. The present study aimed to examine the time course of shoulder pain, particularly the association between prior and later occurrence of shoulder pain episodes, over a period of 5 years in the recovery phase after the GEJE.
Materials and Methods
Participants
A panel study was conducted on residents living in the northeastern coastal areas of Japan that suffered severe damage from the GEJE, including Ogatsu, Oshika, and Ajishima in Ishinomaki City and Wakabayashi Ward in Sendai City, Miyagi Prefecture. The first survey was initiated at 3 months after the GEJE (from June to October in 2011) and was performed every 6 months in Ogatsu, Oshika, and Wakabayashi Ward and every year in Ajishima (Hagiwara et al. 2017a; Yabe et al. 2019a). For the first study, inhabitants registered in the Residential Registry of Ogatsu, Oshika, and Ajishisma as well as those who resided in temporary prefabricated houses in Wakabayashi Ward, were recruited. As the number of participants increased up to the survey conducted from May to August in 2013 (i.e., approximately 2 years after the GEJE) and remained constant after that period, the data at 2 years after the GEJE (first period), 4 years after the GEJE (second period), and 7 years after the GEJE (third period) were used to examine the time course of shoulder pain over a period of 5 years. For each survey, inhabitants aged ≥ 18 years who were registered in the Residential Registry of Ogatsu, Oshika, and Ajishima and those who participated in the previous survey in Wakabayashi Ward were recruited. Self-reported questionnaires and informed consent forms were mailed to these inhabitants. Residents who participated in all three periods were included in this study. A total of 7,007 individuals were recruited in the first period; of these, 41.1% (2,881/7,007) were responders. Subsequently, 78.2% (2,254/2,881) participated in the second period, and 80.8% (1,821/2,254) of the participants in the second period participated in the third period. Finally, a total of 1,821 participants were included in this study (Fig. 1). This study was approved by the institutional review board of our university (approval number: 201192).

Subjective shoulder pain was assessed using the Comprehensive Survey of Living Conditions since it only requires a simple circle response (Ministry of Health, Labour and Welfare of Japan 2019). The question was: “Have you had symptoms within the last few days? If yes, please circle your symptoms” (multiple choices were allowed at the time of the questionnaire). Examples of the possible responses were: “dizziness”, “irritation”, “diarrhea”, “palpitations”, “headache”, “lower back pain”, “shoulder pain”, “knee pain” and “katakori (in Japanese)”. Shoulder pain at the first and/or second surveys was defined as “prior shoulder pain”. The outcome of interest was shoulder pain during the third period. First, shoulder pain during the first period was used as the main predictor to evaluate the effect of prior shoulder pain on the later occurrence of shoulder pain. Second, shoulder pain during the first and second periods was used as the main predictor to evaluate the association between the number of prior shoulder pain episodes and the later occurrence of shoulder pain. Furthermore, shoulder pain was classified into the following three categories according to the presence of pain: (1) absent in both periods, (2) present in each period, and (3) present in both periods.
Covariates
The following variables were assessed using self-reported questionnaires and included in the analysis as covariates because they were thought to be potential confounding factors: sex, age, body mass index, living areas (Ogatsu, Oshika, Wakabayashi Ward, and Ajishima), smoking habits, drinking habits, comorbid conditions (hypertension, diabetes mellitus, myocardial infarction, and cerebral stroke), working status, walking time/day, living status (same house as before the GEJE, prefabricated house, new house, or other), economic hardship (very hard, hard, a little bit hard, and normal), psychological condition, sleep condition, and social condition during the first period. Psychological condition was assessed using the Kessler Psychological Distress Scale, with a score of ≥ 10/24 indicating psychological distress (Suzuki et al. 2014). Sleep condition was evaluated using the Athens Insomnia Scale, with a score of ≥ 6/24 indicating sleep disturbance (Soldatos et al. 2000). Social condition was assessed using the Lubben Social Network Scale, with social isolation defined as a score of < 12/30 (Sone et al. 2016).
Statistical analysis
Variables are presented as numbers and percentages (%). Variables were compared according to shoulder pain in the first period using the chi-square test. Crude and multiple logistic regression analyses were performed to calculate the odds ratios (ORs) and 95% confidence intervals (CIs) for shoulder pain in the third period according to shoulder pain in the first period. Categories of covariates were the same as in a previous report (Sogi et al. 2019) and are summarized in Table 1. Additionally, the participants were divided into subgroups according to age (< 65 or ≥ 65 years) and sex (male or female), and the ORs and 95% CI for shoulder pain in the third period were calculated in the same manner. With respect to stratified analysis, multiplicative interaction between shoulder pain in the first period and age or sex was tested using the Wald test. Furthermore, the ORs and 95% CIs for shoulder pain during the third period were evaluated according to shoulder pain during the first and second periods. All statistical analyses were performed using SPSS version 24.0 (SPSS Japan Inc., Tokyo, Japan), and P-values of < 0.05 were considered to indicate statistical significance.
Results
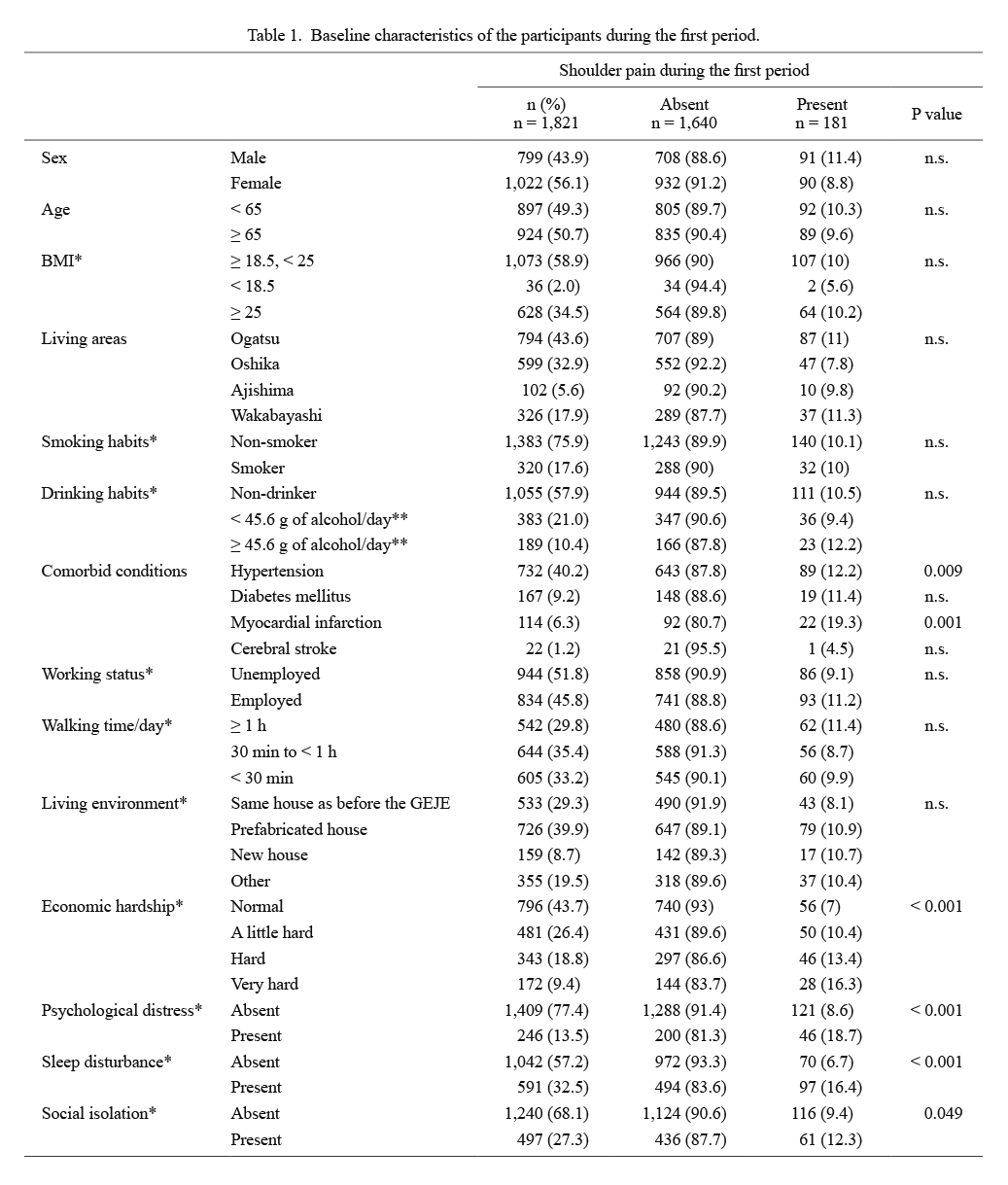
The baseline characteristics of participants are presented in Table 1. The point prevalence of shoulder pain during the first period was 9.9% (181/1,821). Participants with shoulder pain during the first period were more likely to have myocardial infarction as a comorbid condition, subjective economic hardship, psychological distress, sleep disturbance, and social isolation (Table 1).
The pattern of shoulder pain changes from the first to third periods is shown in Table 2. The point prevalence of shoulder pain during the second and third periods was 9.2% (167/1,821) and 11.3% (205/1,821), respectively. Overall, 78% (1,421/1,821) reported no shoulder pain, 15.3% (279/1,821) experienced shoulder pain during one period, 4.9% (89/1,821) had shoulder pain during two periods, and 1.8% (32/1,821) had shoulder pain in all three periods.
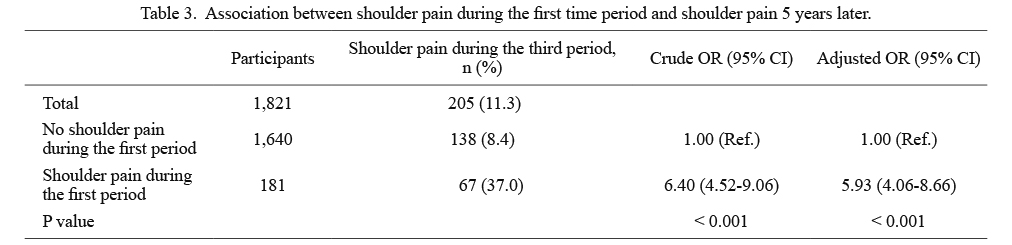
Crude and adjusted analyses revealed that shoulder pain in the first period was significantly associated with shoulder pain in the third period. Using residents without shoulder pain in the first period as the reference, the adjusted OR for shoulder pain in the third period was determined to be 5.93 (95% CI 4.06-8.66) among survivors with shoulder pain in the first period (Table 3).
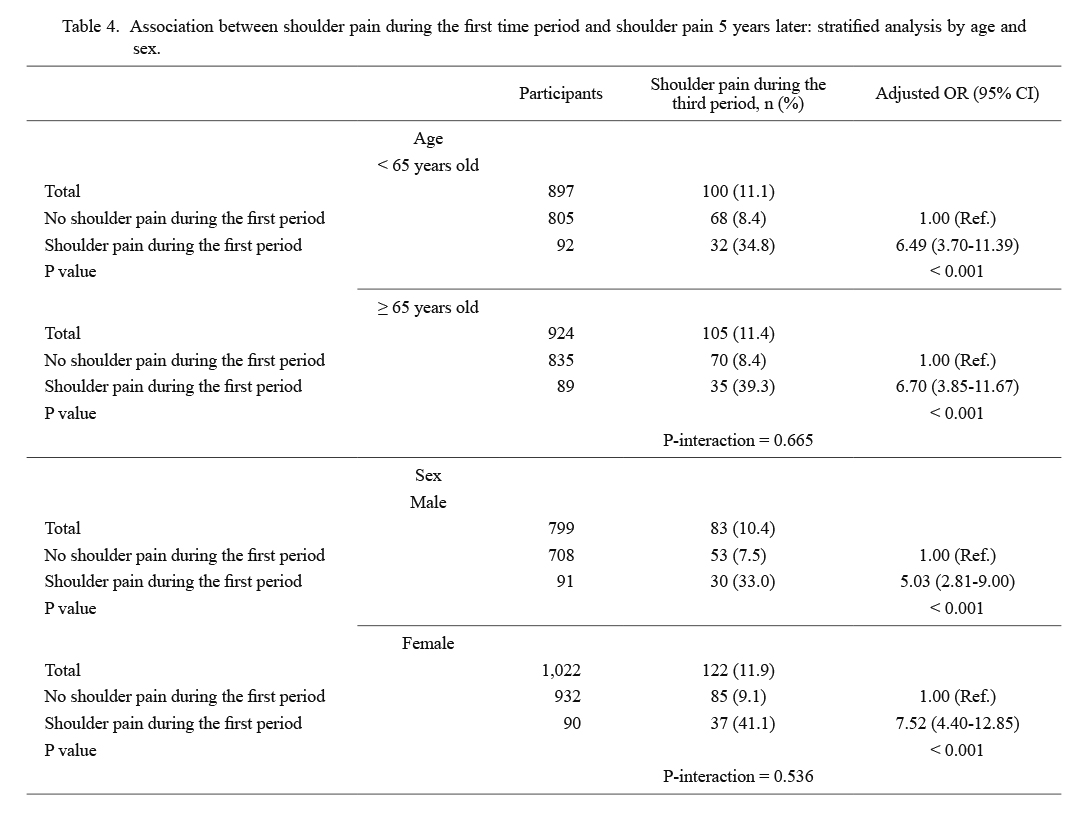
The results of the stratified analysis are presented in Table 4. In each group, shoulder pain during the first period was significantly associated with shoulder pain during the third period. The adjusted OR was 6.49 (95% CI 3.70-11.39) for the < 65 year age group, which was similar to the adjusted OR of 6.70 for the ≥ 65-year age group (95% CI 3.85-11.67). Furthermore, the adjusted OR was 5.03 (95% CI 2.81-9.00) for men, similar to the adjusted OR of 7.52 for women (95% CI 4.40-12.85). No significant multiplicative interaction between shoulder pain during the first period and age or sex was identified (Table 4).
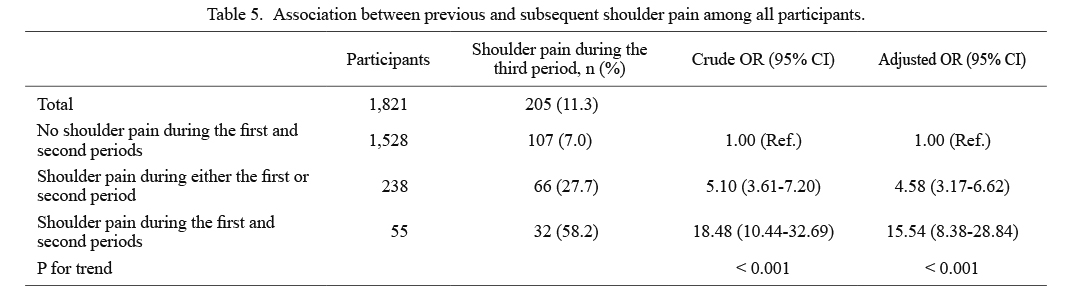
Shoulder pain in the first and second periods was significantly associated with shoulder pain in the third period (Table 5). With the absence of shoulder pain in both the first and second periods used as the reference, adjusted ORs for the presence of shoulder pain in the third period were 4.58 (95% CI 3.17-6.62) during each period and 15.54 (95% CI 8.38-28.84) during both periods (P for trend < 0.001).
Discussion
The present study revealed that prior shoulder pain was significantly associated with the later occurrence of shoulder pain among survivors in the recovery phase after the GEJE. Furthermore, the effect of prior shoulder pain on the later occurrence of shoulder pain was stronger with an increased number of prior shoulder pain episodes.
Globally, musculoskeletal pain conditions are the main cause of disability and, therefore, a major burden to society (GBD 2016 Disease and Injury Incidende and Prevalence Collaborators 2017). Some cross-sectional studies have shown that musculoskeletal pain often occurs at multiple sites, such as the shoulder, elbow, knee, and lower back (Kamaleri et al. 2009; Bayattork et al. 2019). In the general Japanese population, chronic musculoskeletal pain occurs at a frequency of 15.4% and is the highest among individuals between the ages of 30 and 59 years (Nakamura et al. 2011). Nonetheless, this frequency increased to 62%, with a mean Numeric Rating Scale score of 2.74, in GEJE survivors, indicating that GEJE survivors likely suffer from musculoskeletal pain (Yabuki et al. 2015; Yabe et al. 2019a). Among GEJE survivors, musculoskeletal pain was also associated with new-onset poor physical function, psychological distress, and continued residence in temporary prefabricated housing in the recovery phase after the GEJE (Yabe et al. 2018, 2019a, b; Sogi et al. 2019). Furthermore, pre-existing musculoskeletal pain in other body parts was significantly associated with new-onset low back and shoulder pain (Yabe et al. 2020; Hagiwara et al. 2021), and previous low back pain was associated with low back pain among survivors 5 years after the GEJE (Yabe et al. 2021). Musculoskeletal pain among the survivors was multifactorial.
Individuals with a history of shoulder pain and trauma were more likely to report having shoulder pain, suggesting that shoulder pain can be recurrent and frequently progresses to a chronic condition (Rekola et al. 1997; Macfarlane et al. 1998; Meislin et al. 2005; Khosravi et al. 2019). Shoulder pain of long duration, high intensity, and high level of disability predicts persistent complaints (Macfarlane et al. 1998; Noten et al. 2017). Furthermore, musculoskeletal pain in other body sites is highly associated with new-onset shoulder pain among GEJE survivors (Hagiwara et al. 2021). In the present study, prior shoulder pain also affected the later occurrence of shoulder pain. To our knowledge, this is the first study to report the effect of prior shoulder pain on the later occurrence of shoulder pain in both the general population and survivors of the natural disaster for a long period of time. A better understanding of factors influencing shoulder pain among survivors is necessary to aid them in returning to their normal life in a manner similar to that before the GEJE.
Shoulder pain is a pervasive health presentation with complex underlying factors. The exact pathology is not always clear since muscles and joints do not always seem to be the main cause of the problem, and biomedical approaches are sometimes unsuccessful (Noten et al. 2017). A prospective cohort study with a 6-month follow-up in the Netherlands revealed that different forms of acute shoulder pain and chronic shoulder pain were more likely affected by psychosocial factors with poor pain intensity and disability at the general practitioner (Reilingh et al. 2008). Central sensitization is the increased functioning of neurons and circuits in nociceptive pathways that leads to an excessive perception of pain from low-level painful stimuli or pain from innocuous stimuli, which might be a mechanism behind the persistent complaints in some patients with shoulder pain (Noten et al. 2017). With respect to the effect of prior shoulder pain on later shoulder pain episodes, it is speculated that a higher number of prior shoulder pain episodes may have a stronger effect on shoulder pain later. Nevertheless, there exist no reports following a long duration of time and assessing the association between the number of prior shoulder pain episodes and the later occurrence of shoulder pain using logistic regression models. Identifying individuals with shoulder pain according to the number of prior shoulder pain episodes may be useful in developing strategies for the treatment and prevention of shoulder pain.
Shoulder pain is believed to have multifactorial etiologies, with age being a considerable risk factor (Miranda et al. 2001; Luime et al. 2004; Vincent et al. 2017; Khosravi et al. 2019). Furthermore, females had been reported to be significantly associated with an increased prevalence of shoulder pain (Mitchell et al. 2005; Straker et al. 2009). In the present stratified analysis, both < 65-year and ≥ 65-year age groups exhibited similar significance. Additionally, women were more likely to have shoulder pain than were men in the third period; nonetheless, the significance was also observed in men. Musculoskeletal pain has been reported to be more common among older individuals (Kamaleri et al. 2009), and so they are considered more vulnerable to this pain. However, our results show that the association between pre-existing and later onset shoulder pain was greater in female participants. Notably, despite the loss of estrogen having been shown to decrease life-long painful conditions such as headache, menopause can also be accompanied by subsequent painful conditions such as osteoporosis and joint inflammation (Meriggiola et al. 2012). Menopause could play an important role in changing pain sensitivity. Careful attention is required for survivors with multiple pain sites, which provides useful information for clinical and public health policies.
This study has some limitations. First, the response rate during the first period (41.1%) was not high. Since we have no information on the non-responders, their effect on the results of this study remains unclear. Second, this study did not assess shoulder pain intensity and duration or results of prior shoulder pain. The recurrence rate could be high in participants with severe shoulder pain, which should be assessed in future studies. Finally, the study participants lived in coastal areas severely damaged by the GEJE and were not compared to those residing in non-damaged areas. We could not assess the effect of a natural disaster on the results of this study.
In conclusion, the present study showed that prior shoulder pain was associated with shoulder pain after 5 years among GEJE survivors. Furthermore, the effect of prior shoulder pain on the later occurrence of shoulder pain was stronger with an increased number of prior shoulder pain episodes. Therefore, this expertise should be shared with other expert teams, like the Japan Rehabilitation Assistance Team, to address those affected by natural disasters and prepare for future disasters.
Acknowledgments
This study was supported by Health Sciences Research Grant for Health Services [H23-Tokubetsu-Shitei-002, H24-Kenki-Shitei-002, H25-Kenki-Shitei-002 (Fukko)], Ministry of Health, Labour and Welfare, Japan, and Grant-in-Aid for Scientific Research (A; 21H04845) from Japan Society for the Promotion of Science.
Conflict of Interest
The authors declare no conflict of interest.
References
-
Angeletti,
C.,
Guetti,
C.,
Papola,
R.,
Petrucci,
E.,
Ursini,
M.L.,
Ciccozzi,
A.,
Masi,
F.,
Russo,
M.R.,
Squarcione,
S.,
Paladini,
A.,
Pergolizzi,
J.,
Taylor,
R. Jr.,
Varrassi,
G. &
Marinangeli,
F.
(2012) Pain after earthquake. Scand. J. Trauma Resusc. Emerg. Med., 20, 43.
-
Bayattork,
M.,
Jakobsen,
M.D.,
Sundstrup,
E.,
Seidi,
F.,
Bay,
H. &
Andersen,
L.L.
(2019) Musculoskeletal pain in multiple body sites and work ability in the general working population: cross-sectional study among 10,000 wage earners. Scand. J. Pain, 19, 131-137.
-
GBD 2016 Disease and Injury Incidende and Prevalence Collaborators
(2017) Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet, 390, 1211-1259.
-
Gill,
T.K.,
Shanahan,
E.M.,
Tucker,
G.R.,
Buchbinder,
R. &
Hill,
C.L.
(2020) Shoulder range of movement in the general population: age and gender stratified normative data using a community-based cohort. BMC Musculoskelet. Disord., 21, 676.
-
Hagiwara,
Y.,
Sekiguchi,
T.,
Sugawara,
Y.,
Yabe,
Y.,
Koide,
M.,
Itaya,
N.,
Yoshida,
S.,
Sogi,
Y.,
Tsuchiya,
M.,
Tsuji,
I. &
Itoi,
E.
(2017a) Association between sleep disturbance and new-onset subjective shoulder pain in survivors of the Great East Japan Earthquake: a prospective cohort study in Miyagi Prefecture. Tohoku J. Exp. Med., 242, 193-201.
-
Hagiwara,
Y.,
Sekiguchi,
T.,
Yabe,
Y.,
Sugawara,
Y.,
Watanabe,
T.,
Kanazawa,
K.,
Koide,
M.,
Itaya,
N.,
Tsuchiya,
M.,
Tsuji,
I. &
Itoi,
E.
(2017b) Living status, economic hardship and sleep disturbance were associated with subjective shoulder pain in survivors of the Great East Japan Earthquake: a cross sectional study. J. Orthop. Sci., 22, 442-446.
-
Hagiwara,
Y.,
Yabe,
Y.,
Sekiguchi,
T.,
Sugawara,
Y.,
Tsuchiya,
M.,
Yoshida,
S.,
Onoki,
T.,
Takahashi,
T.,
Iwatsu,
J.,
Tsuji,
I. &
Itoi,
E.
(2021) Association of musculoskeletal pain in other body parts with new-onset shoulder pain: a longitudinal study among survivors of the Great East Japan Earthquake. BMJ Open, 11, e041804.
-
Institute of Medicine
(2011) Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research, The National Academies Press, Washington, DC.
-
Ishigaki,
A.,
Higashi,
H.,
Sakamoto,
T. &
Shibahara,
S.
(2013) The Great East-Japan Earthquake and devastating tsunami: an update and lessons from the past Great Earthquakes in Japan since 1923. Tohoku J. Exp. Med., 229, 287-299.
-
Kamaleri,
Y.,
Natvig,
B.,
Ihlebaek,
C.M.,
Benth,
J.S. &
Bruusgaard,
D.
(2009) Change in the number of musculoskeletal pain sites: a 14-year prospective study. Pain, 141, 25-30.
-
Khosravi,
F.,
Amiri,
Z.,
Masouleh,
N.A.,
Kashfi,
P.,
Panjizadeh,
F.,
Hajilo,
Z.,
Shanayii,
S.,
Khodakarim,
S. &
Rahnama,
L.
(2019) Shoulder pain prevalence and risk factors in middle-aged women: a cross-sectional study. J. Bodyw. Mov. Ther., 23, 752-757.
-
Luime,
J.J.,
Koes,
B.W.,
Hendriksen,
I.J.,
Burdorf,
A.,
Verhagen,
A.P.,
Miedema,
H.S. &
Verhaar,
J.A.
(2004) Prevalence and incidence of shoulder pain in the general population; a systematic review. Scand. J. Rheumatol., 33, 73-81.
-
Macfarlane,
G.J.,
Hunt,
I.M. &
Silman,
A.J.
(1998) Predictors of chronic shoulder pain: a population based prospective study. J. Rheumatol., 25, 1612-1615.
-
Meislin,
R.J.,
Sperling,
J.W. &
Stitik,
T.P.
(2005) Persistent shoulder pain: epidemiology, pathophysiology, and diagnosis. Am. J. Orthop. (Belle Mead N.J.), 34, 5-9.
-
Meriggiola,
M.C.,
Nanni,
M.,
Bachiocco,
V.,
Vodo,
S. &
Aloisi,
A.M.
(2012) Menopause affects pain depending on pain type and characteristics. Menopause, 19, 517-523.
-
Ministry of Health, Labour and Welfare of Japan
(2019) Summary Report of Comprehensive Survey of Living Conditions 2019 in Japan.
https://www.mhlw.go.jp/english/database/db-hss/cslc-report2019.html [Accessed: August 4, 2021].
-
Miranda,
H.,
Viikari-Juntura,
E.,
Martikainen,
R.,
Takala,
E.P. &
Riihimaki,
H.
(2001) A prospective study of work related factors and physical exercise as predictors of shoulder pain. Occup. Environ. Med., 58, 528-534.
-
Mitchell,
C.,
Adebajo,
A.,
Hay,
E. &
Carr,
A.
(2005) Shoulder pain: diagnosis and management in primary care. BMJ, 331, 1124-1128.
-
Nakamura,
M.,
Nishiwaki,
Y.,
Ushida,
T. &
Toyama,
Y.
(2011) Prevalence and characteristics of chronic musculoskeletal pain in Japan. J. Orthop. Sci., 16, 424-432.
-
Noten,
S.,
Struyf,
F.,
Lluch,
E.,
D’Hoore,
M.,
Van Looveren,
E. &
Meeus,
M.
(2017) Central pain processing in patients with shoulder pain: a review of the literature. Pain Pract., 17, 267-280.
-
Phillips,
C.J.
(2009) The cost and burden of chronic pain. Rev. Pain, 3, 2-5.
-
Reilingh,
M.L.,
Kuijpers,
T.,
Tanja-Harfterkamp,
A.M. &
van der Windt,
D.A.
(2008) Course and prognosis of shoulder symptoms in general practice. Rheumatology (Oxford), 47, 724-730.
-
Rekola,
K.E.,
Levoska,
S.,
Takala,
J. &
Keinanen-Kiukaanniemi,
S.
(1997) Patients with neck and shoulder complaints and multisite musculoskeletal symptoms--a prospective study. J. Rheumatol., 24, 2424-2428.
-
Sogi,
Y.,
Yabe,
Y.,
Hagiwara,
Y.,
Sekiguchi,
T.,
Sugawara,
Y.,
Tsuchiya,
M.,
Koide,
M.,
Itaya,
N.,
Yoshida,
S.,
Yano,
T.,
Tsuji,
I. &
Itoi,
E.
(2019) Association between continued residence in temporary prefabricated housing and musculoskeletal pain in survivors of the Great East Japan Earthquake: a longitudinal study. BMJ Open, 9, e030761.
-
Soldatos,
C.R.,
Dikeos,
D.G. &
Paparrigopoulos,
T.J.
(2000) Athens Insomnia Scale: validation of an instrument based on ICD-10 criteria. J. Psychosom. Res., 48, 555-560.
-
Sone,
T.,
Nakaya,
N.,
Sugawara,
Y.,
Tomata,
Y.,
Watanabe,
T. &
Tsuji,
I.
(2016) Longitudinal association between time-varying social isolation and psychological distress after the Great East Japan Earthquake. Soc. Sci. Med., 152, 96-101.
-
Straker,
L.M.,
O’Sullivan,
P.B.,
Smith,
A.J. &
Perry,
M.C.
(2009) Relationships between prolonged neck/shoulder pain and sitting spinal posture in male and female adolescents. Man. Ther., 14, 321-329.
-
Suzuki,
Y.,
Fukasawa,
M.,
Obara,
A. &
Kim,
Y.
(2014) Mental health distress and related factors among prefectural public servants seven months after the great East Japan Earthquake. J. Epidemiol., 24, 287-294.
-
Vincent,
K.,
Leboeuf-Yde,
C. &
Gagey,
O.
(2017) Are degenerative rotator cuff disorders a cause of shoulder pain? Comparison of prevalence of degenerative rotator cuff disease to prevalence of nontraumatic shoulder pain through three systematic and critical reviews. J. Shoulder Elbow Surg., 26, 766-773.
-
Walker-Bone,
K.,
Palmer,
K.T.,
Reading,
I.,
Coggon,
D. &
Cooper,
C.
(2004) Prevalence and impact of musculoskeletal disorders of the upper limb in the general population. Arthritis Rheum., 51, 642-651.
-
Yabe,
Y.,
Hagiwara,
Y.,
Sekiguchi,
T.,
Sugawara,
Y.,
Tsuchiya,
M.,
Itaya,
N.,
Yoshida,
S.,
Sogi,
Y.,
Yano,
T.,
Onoki,
T.,
Tsuji,
I. &
Itoi,
E.
(2019a) Musculoskeletal pain and new-onset poor physical function in elderly survivors of a natural disaster: a longitudinal study after the great East Japan earthquake. BMC Geriatr., 19, 274.
-
Yabe,
Y.,
Hagiwara,
Y.,
Sekiguchi,
T.,
Sugawara,
Y.,
Tsuchiya,
M.,
Koide,
M.,
Itaya,
N.,
Yoshida,
S.,
Sogi,
Y.,
Yano,
T.,
Tsuji,
I. &
Itoi,
E.
(2018) Higher incidence of sleep disturbance among survivors with musculoskeletal pain after the Great East Japan Earthquake: a prospective study. Tohoku J. Exp. Med., 244, 25-32.
-
Yabe,
Y.,
Hagiwara,
Y.,
Sekiguchi,
T.,
Sugawara,
Y.,
Tsuchiya,
M.,
Koide,
M.,
Itaya,
N.,
Yoshida,
S.,
Sogi,
Y.,
Yano,
T.,
Tsuji,
I. &
Itoi,
E.
(2019b) Musculoskeletal pain is associated with new-onset psychological distress in survivors of the Great East Japan Earthquake. Disaster Med. Public Health Prep., 13, 295-300.
-
Yabe,
Y.,
Hagiwara,
Y.,
Sekiguchi,
T.,
Sugawara,
Y.,
Tsuchiya,
M.,
Yoshida,
S.,
Sogi,
Y.,
Onoki,
T.,
Suzuki,
K.,
Takahashi,
T.,
Iwatsu,
J.,
Tsuji,
I. &
Itoi,
E.
(2021) A 5-year longitudinal study of low back pain in survivors of the Great East Japan Earthquake. Spine (Phila Pa 1976), 46, 695-701.
-
Yabe,
Y.,
Hagiwara,
Y.,
Sekiguchi,
T.,
Sugawara,
Y.,
Tsuchiya,
M.,
Yoshida,
S.,
Sogi,
Y.,
Yano,
T.,
Onoki,
T.,
Takahashi,
T.,
Iwatsu,
J.,
Tsuji,
I. &
Itoi,
E.
(2020) Musculoskeletal pain in other body sites is associated with new-onset low back pain: a longitudinal study among survivors of the great East Japan earthquake. BMC Musculoskelet. Disord., 21, 227.
-
Yabuki,
S.,
Ouchi,
K.,
Kikuchi,
S. &
Konno,
S.
(2015) Pain, quality of life and activity in aged evacuees living in temporary housing after the Great East Japan earthquake of 11 March 2011: a cross-sectional study in Minamisoma City, Fukushima prefecture. BMC Musculoskelet. Disord., 16, 246.