Abstract
After the Great East Japan Earthquake, Tohoku University began to provide mental health services during the acute phase of the disaster in cooperation with Shichigahama Town, one of the municipalities located in the coastal area of the Miyagi Prefecture that was severely damaged by the earthquake and tsunami; it continued to be providing long-term mental health activities, incorporating annual surveys for affected residents in the town for 10 years. Ten years of combination of surveys and outreach activities first depicted detailed longitudinal alterations in the mental health conditions of communities affected by a catastrophe. While posttraumatic stress reaction had recovered year by year after the year following the Great East Japan Earthquake, recovery from psychological distress retreated between 2014 and 2017, probably due to the relocation from temporal to eternal housing conditions. The annual cycles of assessment and provision of mental health support and promotion activities continued for 10 years can be an initial model for evidence-based, long-term post-disaster mental health and psychosocial support for the affected communities. Data regarding subsequent disasters should be collected in comparable ways, in order to improve the accuracy and usefulness of the accumulated data for planning and providing evidence-based post-disaster mental health and psychosocial support.
Introduction
After the 1995 Great Hanshin-Awaji Earthquake, the mental health conditions of people affected by a disaster began drawing attention in Japan. Teams consisting of mental health care professionals visited the affected area to provide support for the local mental health care systems and residents during the acute phase of the disaster. Mental care centers, namely “Kokoro-no Care Centers,” to provide support for the affected communities in the long-term phase of the disaster were funded by the reconstruction budgets from the Japanese Government in Hyogo Prefecture after the 1995 Great Hanshin-Awaji Earthquake; Niigata Prefecture after the 2007 Niigataken Chuetsu-oki Earthquake; Iwate, Miyagi and Fukushima Prefectures after the 2011 Great East Japan Earthquake (GEJE); and Kumamoto Prefecture after the 2016 Kumamoto Earthquakes (Kunii et al. 2022). In addition to these centers, numerous organizations offered various kinds of activities to the affected communities with the intention of providing mental health support. These activities included (1) one-on-one support for individuals in need of assistance, (2) support for collective activities to facilitate social interaction, (3) support for living conditions, (4) increasing public awareness about mental health, (5) human resource development to improve response capabilities for mental health care, (6) support for mental health care providers, and (7) facilitating collaboration among mental health care activities (Seto et al. 2019).
In general, it is difficult to grasp the effectiveness of the current mental health and living conditions of people in the affected communities, where there is a need for support, including the types of resources available for mental health support. Information gathering is the first step in planning a psychiatric disaster response. The needs assessment and planning for each target community are integral to all the phases of the response. Whether involved in information gathering and logistical planning, a needs assessment mission, or clinical deployment, mental health responders should work according to a needs assessment. Three essential categories of information to launch a post-disaster mental health response have been suggested: basic facts of the general disaster type, information about its impact on the community, and background information about the pre-disaster community. Among them, determination of the magnitude of the mental health impact of a disaster lies at the core of the information needed by post-disaster mental health care providers. This may involve a community-level assessment of symptoms or behavioral changes during the disaster’s acute phase and disorders during the post-acute phase, enabling the design of appropriate mental health support measures (Katz 2011).
The guidelines and textbooks integrating the above principles do not clarify the timeframe of the period in which assessment and support would preferably be provided. As the impact of a catastrophe is known to remain after many years, mental health support should ideally be provided in a continuous manner. As the years pass, the effects of the disaster on mental health conditions among the affected communities become more obscure. It becomes more difficult to indicate how the current mental health condition of affected people is directly or indirectly relevant to the disaster, to what extent they have recovered, and the degree of effectiveness of the support.
However, there have been very few records of mental health support integrating a community-level assessment of symptoms or behavioral changes, as well as support planned based on the assessment. Therefore, we aimed to report an overview of a decade of mental health support conducted as a cooperative project between Shichigahama Town and Tohoku University, both located in the Miyagi Prefecture, under the name of the Shichigahama Health Promotion Project.
Mental Health Support in the Acute Phase and Context behind Starting the Shichigahama Health Promotion Project
Within a few days after the GEJE, mental health support teams from various regions of Japan were deployed in most local governmental districts severely damaged by the disaster. Tohoku University assigned mental health support teams to several affected regions in the cities of Sendai, Ishinomaki, Kesennuma, Iwanuma, and Watari.
In Shichigahama Town, located in the coastal area of the Miyagi Prefecture, there were around 6,500 households composed of 20,897 residents at the time of the onset of the GEJE. Around 96 residents were killed or missing in the event, 674 households were washed away or totally damaged, 237 households were majorly damaged, 413 households were half-collapsed, and 2,605 households were partially damaged. A total of 1,323 households suffered damage to buildings that were half-collapsed or more, which had a significant impact on the town’s residents (Shichigahama Town 2014). While Shichigahama Town accepted medical support teams immediately after onset, mental health support teams were not included in these teams for a while. On March 22, Shichigahama Town Hall requested the Miyagi Prefectural Government to dispatch a mental health support team, and the latter from Tohoku University was deployed to the town. The team visited the town on March 23, shared information, and planned to provide mental health support for the affected residents and workers to deal with their recovery. The team had mental health-related meetings with the town hall representatives every morning and evening, and visited seven evacuation centers and affected people remained in their own houses during the daytime between March 23 and 28. As many of the affected people became busy working on daily activities and reconstructions, the teams decreased their frequency of visiting the town. The team visited evacuation center, and affected people remained in the damaged housing every Tuesday and Friday between March 29 and April 29. At the end of April, the need for activities as a team diminished and that for consultations based on personal cases increased. Since May 2, a psychiatrist started to visit the town once a week to deal with cases of psychosocial problems, arranging seminars for various kinds of populations and meetings with health care givers. By the middle of June, prefabricated temporary housing was built in seven areas of the town, and individuals moved into the housing. Meeting places were set at each of the seven areas for residents to gather freely during the daytime. Many volunteer groups visited the meeting places to provide various kinds of support, including exercises, cultural activities, recreation, and massage. Personnel were hired by the local government (Shichigahama Town) to facilitate interactions among residents of the housing and take care of those who were isolated or in need of help. Since September 1, a series of workshops focusing on the psychosocial effects of the GEJE on the community as “psychoeducation” were held by public health nurses in the town and members of Tohoku University in each of the meeting places of the temporary housing areas. In the sessions, many of the residents and public health nurses raised concerns that people in the temporary housing who did not attend the workshops and those who lived outside the temporary housing seemed to have more severe psychosocial problems; more intense assessment was needed to grasp their current conditions. Through discussions among the affected residents, the local government of Shichigahama and Tohoku University established the Shichigahama Health Promotion Project, which was designed as a post-disaster mental health support program integrating the annual health surveys of affected residents (Fig. 1); it was funded by the Ministry of Health, Labour and Welfare as part of a research on health surveys of the population affected by the GEJE.

The Initiation of Mental Health Surveys Conducted in the Shichigahama Health Promotion Project
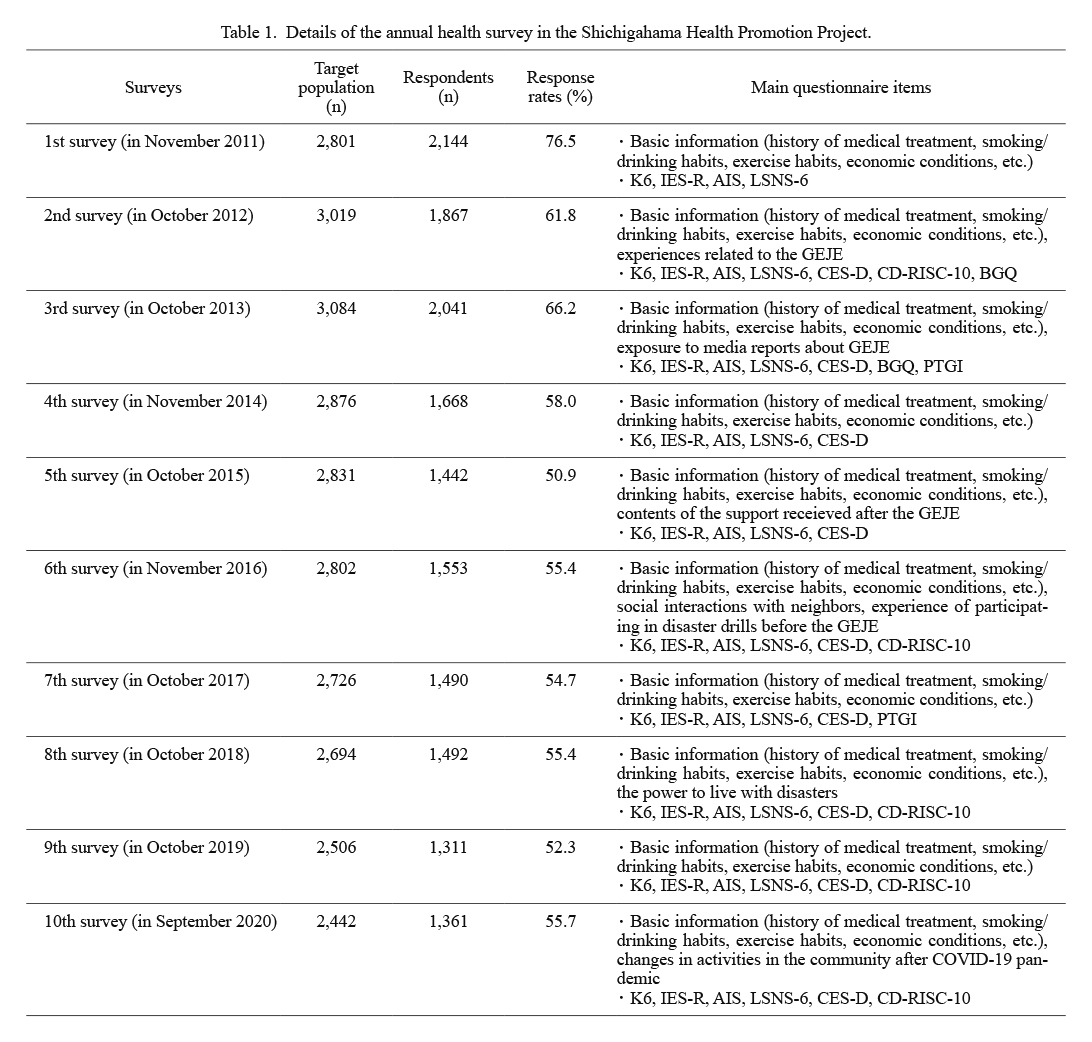
The first health survey was conducted in November 2011 (Fig. 1). The aims of the annual surveys were: 1) to monitor the effects of the damage caused by the GEJE on health status in affected communities in the town; 2) to contribute to the intervention regarding psychological or psychiatric problems according to the results of the monitoring; and 3) to accumulate knowledge regarding the environmental and psychosocial factors that affected the mental health conditions of the communities post the disaster. Subjects of the survey (n = 2,801) were people (all ages) who resided in Shichigahama Town at the onset of the GEJE, and whose housings were certified as “completely destroyed” and “significantly destroyed,” as the selection criteria based on the building damage assessment conducted by the Shichigahama Government, following the criteria issued by the Cabinet Office. In the first survey, investigators visited every home, distributed self-administered questionnaires after obtaining informed consent, and retrieved the questionnaires several days later. Questionnaires included the following: 1) employment status; 2) perceived economic conditions; 3) social interactions evaluated by the Lubben Social Network Scale-6 items version (LSNS-6) (Lubben et al. 2006); 4) social capital; 5) general health conditions; 6) daily physical activity; 7) habits of eating; 8) alcohol drinking and smoking habits; 9) sleep conditions evaluated using the Athens Insomnia Scale (AIS) (Soldatos et al. 2000); 10) psychological distress evaluated by the Kessler six-item psychological distress (K-6) scale (Kessler et al. 2002); and 11) posttraumatic stress reactions (PTSR) evaluated by the revised impact-of-event scale (IES-R) (Weiss 2004). These questionnaires were administered as standard questionnaires every year throughout the 10 years of observation period, and the data were collected annually (Table 1). As from the second survey conducted in October 2012, the Center for Epidemiologic Studies Depression Scale (CES-D) and residential conditions were added to the standard questionnaire. As other survey items, Brief Grief Questionnaire (BGQ) in the 2nd and 3rd surveys, 10-item Connor-Davidson Resilience Scale (CD-RISC-10) in the 2nd, 6th, 8th, 9th, and 10th surveys, and Posttraumatic Growth Inventory (PTGI) in the 3rd and 7th surveys, were added to the standard questionnaire respectively.
Of the 2,801 affected residents, 2,144 (76.5%) answered the questionnaire in the first survey. At the time (November, 2011), 48% of the participants lived in prefabricated temporary housing and around 18% lived outside the town, mainly due to the limited living space in the town. Among the adult populations (n = 1,871), 32% showed PTSR with IES-R scores greater than the cutoff point of 25, 50% showed a mild or severer level of psychological distress with K-6 scores greater than 5, and 57% showed a suggested condition of sleep disturbance with an AIS of ≥ 4.
An overview of the mental health conditions was posted to all participants as feedback. Workshops were held by the public health nurses of the town and members of the Tohoku University team in each of the meeting places of the prefabricated temporary housing in February 2012, to discuss how the attendees felt about the outcome of the studies and their current conditions, including the impact of the disaster on the communities. The outcome of the studies was also provided to all residents in the town, along with advice to promote mental health as columns in the monthly journal issued. The public health nurses and members of Tohoku University visited the participants whose answers to the questions seemed to involve a high risk of mental health problems, and offered support for these residents.
The updated protocols of the 10 surveys were reviewed and approved by the Ethics Committee of Tohoku University Graduate School of Medicine every year before conducting the surveys (2021-1-618).
After the Second Survey of the Shichigahama Health Promotion Project
The inclusion criteria, that is, individuals (all ages) who resided in Shichigahama Town at the onset of the GEJE, and whose houses were certified as “completely destroyed” and “significantly destroyed,” were consistently applied to the study sample every time the 10 surveys conducted between 2011 and 2020. The total number of target population increased slightly by 2012, as the judgement of the extent of destruction was made after the first survey. In 2014, the list of target subjects was fixed, and after 2015, the total number of potential participants gradually decreased as some participants moved out of the residence without informing the survey team or refused to participate in the survey (Table 1).
In order to assess mental health needs among the community members with less house damage, only in the second survey, we added the people who met the following criteria in addition to the target population mentioned above; 1) their houses were not completely or significantly damaged by the GEJE, and 2) they also lived in five specific seashore areas of Shichigahama Town in September 2012, where more than 10% of households were completely or partially damaged by the GEJE.
Between 2011 and 2013, the investigators visited the participants and passed them the questionnaires directly upon obtaining informed consent. Between 2014 and 2020, explanations of the follow-up surveys and questionnaires were posted to the participants, with a message that those who returned the questionnaires deemed to be considered to participate the survey with informed consent.
Workshops to discuss the current psychosocial conditions of the communities and attendees in the meeting places of prefabricated temporary housing and post-disaster public condominiums were held twice a year until 2018. In these workshops, the kinds of questions we should ask in the next survey were also discussed among the participants, and these questions were prepared specifically for the next survey, being added to the standard questionnaires that were filled consistently every year for 10 years. For example, in the second survey, the respondents were asked about their experience of the earthquake and tsunami, evacuations, loss of close persons, properties, and customs due to the GEJE. In the fifth survey, anxiety regarding the transfer of housing from temporary housing to a new place, such as post-disaster public condominiums, was assessed. In the 6th and 10th surveys, a detailed manner of interaction with neighbors was assessed.
In addition to the ten questionnaire-based surveys, several other types of surveys were conducted on specific topics separately from this project. For example, to grasp concerns that must be considered for perinatal women’s mental healthcare in post-disaster settings, participants of mothers who had given birth were recruited for our preliminary questionnaire survey during the public, medical/developmental check-ups for 18-month-old children held between October 2012 and March 2013 (Kobayashi et al. 2020).
Ten Years of Alterations in Mental Health Conditions among the Communities in Shichigahama Town Affected by the GEJE
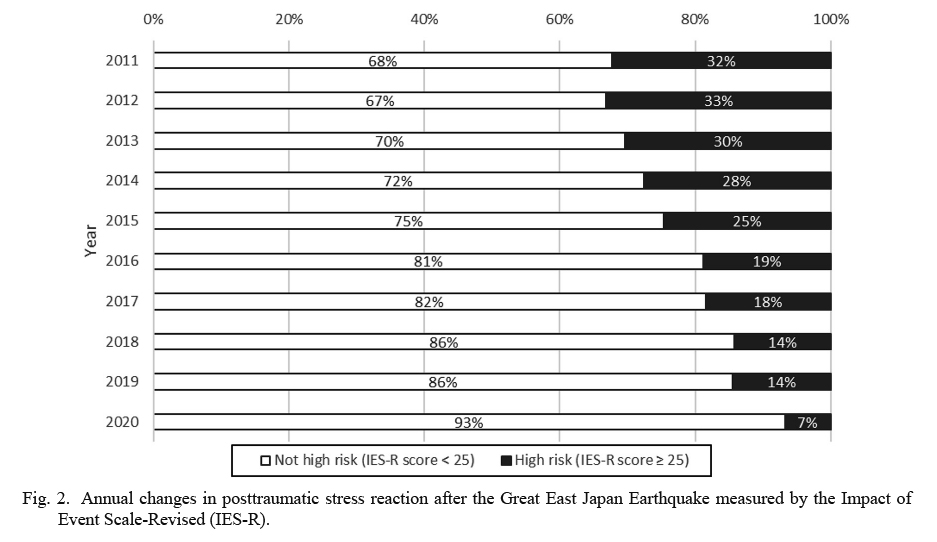
The PTSR due to the GEJE may reflect a direct impact on the mental health conditions of affected people. The proportion of subjects who showed IES-R scores equal to or greater than the cut-off point of 25 (defined as subjects with PTSR in the following part) among the total survey subjects was monitored for 10 years. The percentage of individuals with PTSR was 32% eight months after the GEJE in 2011, and 33% in the following year. After that, it gradually decreased as the years went by; 30% in 2013, 28% in 2014, 25% in 2015, 19% in 2016, 18% in 2017, 14% in 2018 and 2019, and 7% in 2020 (Fig. 2).
Unlike PTSR, psychological distress measured by K-6 among the communities did not recover in one direction over time. A just 50% of the participants had a K-6 score of five or more, that is, they suffered from mild or severer psychological distress eight months after the GEJE. Until 2014, the percentage decreased year by year to 31%, which was almost the same level as the average of the National Basic Survey (https://www.mhlw.go.jp/english/database/db-hss/cslc-report2013.html). Subsequently, the percentage of participants who felt psychological distress increased slightly in 2015, 2016, and 2017 (Fig. 3). While the duration following the onset of the disaster influences recovery from the event-related PTSR, psychological distress may be affected by other factors besides the post-event duration. The surrounding situations of affected people have continuously changed throughout the decade in various aspects. Among them, drastic changes for many individuals occurred around 2014, when post-disaster public condominiums were built and highland was newly created for the affected people, with them moving from the prefabricated temporary housing to new places. While moving to a new location was beneficial with regard to having more privacy, amenities, and comfort related to living in a place for a long time, the relocation forced the affected people to be away from those in the temporary housing with whom they shared their post-disaster experiences. The robustness of buildings with thick walls and doors distracted people from feeling signs of neighbors’ presence and casual communications, which they appreciated in the prefabricated temporary housing. In the new places, the meeting places were no longer freely open during the daytime, and reservation and payment became necessary to use these spaces. There were no longer personnel hired specifically to look after the affected population, and most volunteers quit the activities by that time. The temporal worsening of psychological distress among communities between 2014 and 2017 may have reflected these drastic changes in living conditions. In the workshops held during this period, claims of loneliness from many of the participants due to the environmental gaps between the temporary housing and their current living conditions endorsed this data. The time course of the data, along with what was told in the workshops, suggested that people may have successfully adjusted to the new environment and created new communities after 2018.
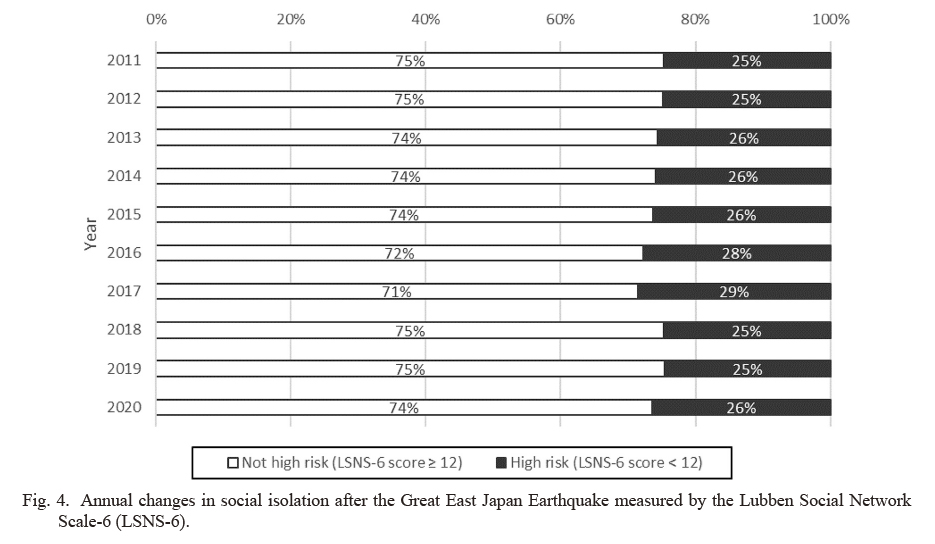
The assessment of social isolation based on the number of family members, relatives, and friends to interact with using the LSNS-6 validated the above discussion. LSNS-6 scores of 0-11 points were described as being “socially isolated,” and 12-30 points were thought as being “strongly connected with others.” The percentage of individuals being “socially isolated” remained at 25-26% from 2011 to 2015, but showed a slight increase to 28-29% in 2016 and 2017. Subsequently, it decreased to 25% in 2018 and 2019, being 26% in 2020 (Fig. 4).
Based on the relationship between the K-6 and LSNS-6, the annual changes in the percentage of strongly connected and socially isolated subpopulations, who showed more than mild psychological distress, were as follows: in 2011, the first year of the disaster, the percentage of strongly connected subjects who felt psychological distress was 46%, and that of socially isolated subjects who felt psychological distress was 63%. However, over time, the percentage of those who felt psychological distress among strongly connected subjects decreased to 20%, and the percentage of those who felt psychological distress among socially isolated subjects decreased to 40%. The strongly connected group remained largely unchanged, whereas the socially isolated group rose to 50% in 2017, fell to 34% in 2018, and rose again to 41% in 2019 (Fig. 5). The peaks in 2017 and 2019 might reflect the severe flood damage caused by the typhoons that occurred during the surveys, which might induce memories of those days and exaggerate the psychological distress of the socially isolated population.
Regarding the recovery of mental health indicators after the disaster, PTSR maintained a recovery trend with the passage of time after the traumatic event, while psychological distress was exacerbated by major environmental changes, such as moving into post-disaster public condominiums and relocating to higher ground during the recovery process, which is a pivotal finding when considering long-term health promotion in the aftermath of disasters. In anticipation of these environmental changes, it was suggested that the following efforts could help improve the community’s recovery process regarding the mental health consequences of disasters: 1) promoting interpersonal interaction from the time of moving into temporary housing to the new environment; 2) considering infrastructure to promote interpersonal interaction in the new environment; 3) rather than disbanding the temporary housing support center and charging for community space all at once, it is recommended that after the transition, assistance be provided for a while until the residents adjust to new environments and create networks with their new neighbors; and 4) monitoring social interaction habits and mental health conditions of the residents, gradually shifting from “public support” to “self-help” for maintaining mental health conditions.
Overview of Mental Health Studies Using the Cohort of the Shichigahama Health Promotion Project
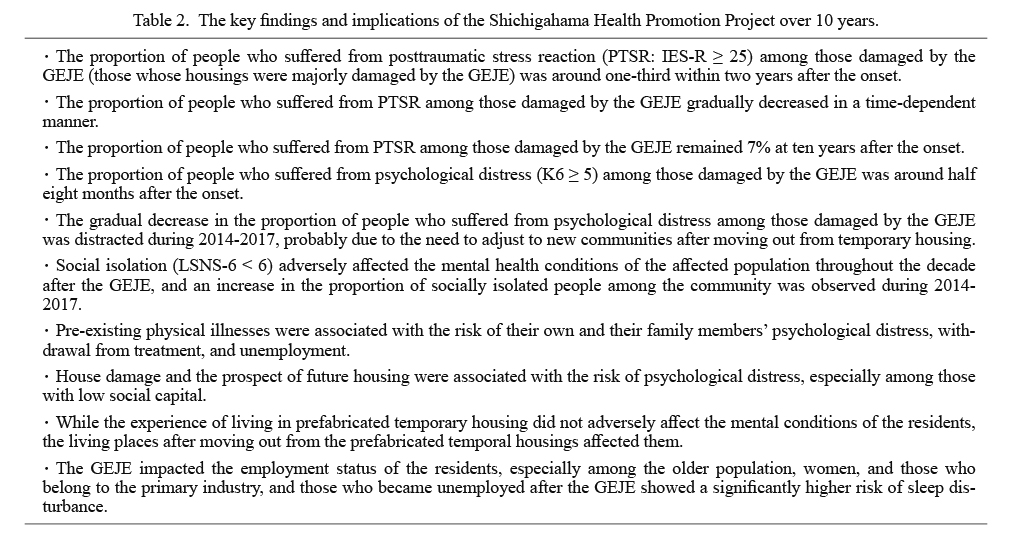
The survey data were not only utilized for promoting the mental health of the affected communities in Shichigahama Town, but also for extracting findings to be accumulated to improve preparedness and response to future disasters (Table 2). The survey data depicted how the GEJE impacted living and mental health conditions. The data also endorsed and added new insight to the knowledge that physical health and living conditions, including living places and employment, significantly impact the mental health of the people affected by the disaster, alongside their family members through interaction with other factors.
Being affected with physical diseases had a positive correlation with psychological distress, regardless of the degree of damage to the house (Nakaya et al. 2015). The data indicated that it was also associated with the psychological distress of the partners (Nakaya et al. 2016c). As other psychosocial aspects of being affected by chronic diseases needed to be considered, psychological distress was associated with the risk of withdrawal from hypertension treatment (Nakaya et al. 2017). The data further revealed that being affected by chronic diseases was associated with unemployment risk (Nakaya et al. 2016b), which was a major issue in the community affected by a catastrophe, as described later. Periodontal disease was also associated with insomnia, which is closely related to mental health problems in affected communities (Tsuchiya et al. 2015). Psychological distress was associated with the incident risk of functional disability in elderly people affected by a disaster (Tanji et al. 2017; Sone et al. 2021).
The living conditions of the affected communities were devastated by the GEJE, and drastically changed over the decade after the event, as described in the sections above. The survey showed that the degree of housing damage may affect the association between social capital and psychological distress. Low social capital increased the risk of psychological distress, particularly for subjects who experienced large-scale house destruction, and higher social capital played a critical role in protecting the worsening of mental health in post-disaster situations (Tsuchiya et al. 2017). The survey also indicated that the prospect of future housing was associated with the risk of psychological distress one year after the disaster (Nakaya et al. 2016a). While there were concerns regarding the potential risk of living in prefabricated temporal housing on mental health problems, the survey data clarified that living in prefabricated temporary housing did not adversely affect the subsequent social interaction activities or mental conditions of the subjects five years after the disaster (Akaishi et al. 2021). Regarding living places after moving out from the prefabricated temporal housing, living in post-disaster public condominiums showed significantly fewer social interactions, higher depressive symptoms, psychological distress, and PTSR (Suzuki et al. 2021).
Seven years after the disaster, walking habits were evaluated according to whether individuals walked to maintain healthy living habits (health-conscious walkers) or merely for transportation without considering health consequences. Walking duration was negatively associated with avoidance symptoms among non-health-conscious walkers, indicating that the disaster might have had a long-lasting impact on walking habits, probably in relation to environmental changes. The study revealed that walking duration may positively affect mood, but not PTSR, only when walking is performed to maintain healthy living habits (Utsumi et al. 2020).
Employment conditions could be another major factor affecting the mental health of communities affected by disasters. The surveys revealed the severe impact of the GEJE on populations belonging to the primary industry, particularly elderly women. Among participants who had a job before the GEJE, 19% became unemployed after the earthquake. In particular, 34% of the elderly men and 49% of the elderly women became unemployed. In addition, 38% of the subjects who belonged to the primary industry before the disaster became unemployed. Those who became unemployed showed a significantly higher risk of sleep disturbance than those who maintained their jobs (Katayanagi et al. 2020).
In addition to issues regarding mental health conditions, questionnaires were designed with an interdisciplinary effort in the research field of disaster risk reduction, and incorporated in the survey to reveal how the tsunami drill experience before the GEJE was associated with the actual evacuation at the onset of the earthquake. The rate of quick evacuation was significantly higher among those who participated in tsunami disaster drills before the event than among those who did not. The study provided initial evidence to advocate the administration of tsunami drills in seaside communities to enhance evacuation behavior immediately after disaster onset (Nakaya et al. 2018).
Considering the multifactorial nature of mental health conditions, an efficient prediction of these conditions could be made if one identified the interaction among multiple risk factors. The Massive Parallel Limitless-Arity Multiple-Testing Procedure (MP-LAMP) was developed to comprehensively detect significant combinational risk factors and reveal the hidden factors, to explain the long-term trajectory of Posttraumatic Stress Disorder (PTSD) symptoms among the survey participants. Sixty-one potential risk factors encompassing socio-demographics, lifestyle, and traumatic experiences were analyzed using MP-LAMP regarding combinational associations with the trajectory of PTSD symptoms, and 56 significant combinational risk factors were detected. The strongest association was observed with the combination of short resting time, short walking time, unemployment, and experience of evacuation without preparation at the onset of the GEJE (Takahashi et al. 2020).
The Future Direction of the Shichigahama Health Promotion Project
Thus, outcomes from a series of surveys have indicated that although the mental health of the affected population has been improving, PTSR remains evident in the community, suggesting that a careful monitoring and support system is needed even a decade after a catastrophe. Further detailed analyses of the survey data are necessary to examine the cross-sectional correlation between each factor in this survey and the relationship between changes in each factor over time, in order to extract findings that will be beneficial for understanding and improving individuals’ mental health in disaster-affected areas.
Shichigahama Town is a relatively closed, small-scale community in today’s information society, characterized by a relatively larger population belonging to primary industries and a close social distance between the residents, which represents the good old days of Japan where people naturally cared for each other’s surroundings. Conversely, it is a region where young people are leaving for the cities, and the proportion of the aging population has been increasing (the percentage of people aged 65 and over in the 1st survey: 33.7%; in the 10th survey: 44.3%), making it a microcosm in modern Japan. The participation rate of residents in the survey was high, and there was no precedent in the world where the effects of a large-scale disaster could be investigated continuously over a period of 10 years. The findings of the mental health surveys accumulated over the past 10 years can provide useful resources for evaluating how the impact of new natural disasters and other emergencies on the mental health conditions of the affected communities would be different. The Shichigahama data can also be useful in planning mental health care measures for communities affected by another disaster, predicting the prognosis of the impact on these communities.
Conclusion
Ten years of a combination of surveys and outreach activities conducted as a government-academia collaborative project, the Shichigahama Health Promotion Project, first depicted detailed longitudinal alterations in the mental health conditions of communities affected by a catastrophe. While PTSR recovered year by year after the year following the GEJE, recovery from psychological distress retreated between 2014 and 2017, probably due to the subjects’ relocation from temporal to eternal housing conditions. The assessment and provision of mental health support and promotion activities continued every 10 years can be an initial model of evidence-based, long-term, post-disaster mental health and psychosocial support for the affected communities. As data regarding subsequent disasters will be collected in comparable ways, the accuracy and usefulness of the accumulated data are indispensable for planning and providing evidence-based post-disaster mental health and psychosocial support.
Acknowledgments
This study was supported by the Reconstruction Agency; Ministry of Education, Culture, Sports, Science and Technology (MEXT); Japan Agency for Medical Research and Development (AMED) through the Tohoku Medical Megabank Project; Ministry of Health, Labour and Welfare, Japan; Health Sciences Research Grant for Health Services [H24-Kenki-Shitei-002, H25-Kenki-Shitei-002 (Fukko)]; Intramural Research Grant for Special Project Research from the International Research Institute of Disaster Science, Tohoku University, Japan; and Core Research Cluster of Disaster Science, Tohoku University, Japan. We thank the Government of Shichigahama and the residents of the town who supported and participated in this survey. We appreciate Ms. Harumi Nemoto for her assistance in arranging the survey.
Author Contributions
Y.K. and H.T. designed the study. Y.K., H.U., and H.T. conducted the primary literature search and analyzed the data. Y.K. and H.U. created tables and figures. Y.K. wrote the first draft of the manuscript. H.T. played a major role in revising and editing the manuscript. All authors contributed to and approved of the final manuscript.
Conflict of Interest
The authors declare no conflict of interest.
References
-
Akaishi,
T.,
Suzuki,
T.,
Nemoto,
H.,
Utsumi,
Y.,
Seto,
M.,
Usukura,
H.,
Kunii,
Y.,
Sugawara,
Y.,
Nakaya,
N.,
Nakamura,
T.,
Tsuchiya,
N.,
Narita,
A.,
Kogure,
M.,
Hozawa,
A.,
Tsuji,
I.,
et al. (2021) Five-year psychosocial impact of living in post-disaster prefabricated temporary housing. Disaster Med. Public Health Prep., 1-31.
-
Katayanagi,
M.,
Seto,
M.,
Nakaya,
N.,
Nakamura,
T.,
Tsuchiya,
N.,
Narita,
A.,
Kogure,
M.,
Sugawara,
Y.,
Kodaka,
A.,
Utsumi,
Y.,
Usukura,
H.,
Kunii,
Y.,
Hozawa,
A.,
Tsuji,
I. &
Tomita,
H.
(2020) Impact of the Great East Japan Earthquake on the employment status and mental health conditions of affected coastal communities. Int. J. Environ. Res. Public Health, 17, 8130.
-
Katz,
C.L. (2011) Needs Assessment. In Disaster Psychiatry Readiness, Evaluation, and Treatment, edited by Stoddard, F.J.,
Pandya,
A. &
Katz,
C.L.
American Psychiatric Association Publishing, Washington, DC, pp. 49-68.
-
Kessler,
R.C.,
Andrews,
G.,
Colpe,
L.J.,
Hiripi,
E.,
Mroczek,
D.K.,
Normand,
S.L.,
Walters,
E.E. &
Zaslavsky,
A.M.
(2002) Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol. Med., 32, 959-976.
-
Kobayashi,
N.,
Nemoto,
H.,
Seto,
M.,
Sato,
S.,
Kikuchi,
S.,
Honda,
N.,
Suzuki,
T.,
Sato,
K.,
Sugawara,
J.,
Ito,
K.,
Kayano,
R.,
Ozaki,
N.,
Beadling,
C.W.,
Kelman,
I.,
Imamura,
F.,
et al. (2020) Experiences of perinatal women and public healthcare providers in a community affected by the great east Japan earthquake and tsunami: concerns that must be considered for the mental healthcare of perinatal women in postdisaster settings. Intl. J. Disaster Risk Reduct., 51, 101767.
-
Kunii,
Y.,
Usukura,
H.,
Otsuka,
K.,
Maeda,
M.,
Yabe,
H.,
Takahashi,
S.,
Tachikawa,
H. &
Tomita,
H.
(2022) Lessons learned from psychosocial support and mental health surveys during the 10 years since the Great East Japan Earthquake: establishing evidence-based disaster psychiatry. Psychiatry Clin. Neurosci. doi: org/10.1111/pcn.13339. [Epub ahead of print].
-
Lubben,
J.,
Blozik,
E.,
Gillmann,
G.,
Iliffe,
S.,
von Renteln Kruse,
W.,
Beck,
J.C. &
Stuck,
A.E.
(2006) Performance of an abbreviated version of the Lubben Social Network Scale among three European community-dwelling older adult populations. Gerontologist, 46, 503-513.
-
Nakaya,
N.,
Nakamura,
T.,
Tsuchiya,
N.,
Narita,
A.,
Tsuji,
I.,
Hozawa,
A. &
Tomita,
H.
(2016a) Prospect of future housing and risk of psychological distress at 1 year after an earthquake disaster. Psychiatry Clin. Neurosci., 70, 182-189.
-
Nakaya,
N.,
Nakamura,
T.,
Tsuchiya,
N.,
Narita,
A.,
Tsuji,
I.,
Hozawa,
A. &
Tomita,
H.
(2017) Psychological distress and the risk of withdrawing from hypertension treatment after an earthquake disaster. Disaster Med. Public Health Prep., 11, 179-182.
-
Nakaya,
N.,
Nakamura,
T.,
Tsuchiya,
N.,
Tsuji,
I.,
Hozawa,
A. &
Tomita,
H.
(2015) The association between medical treatment of physical diseases and psychological distress after the Great East Japan Earthquake: The Shichigahama Health Promotion Project. Disaster Med. Public Health Prep., 9, 374-381.
-
Nakaya,
N.,
Nakamura,
T.,
Tsuchiya,
N.,
Tsuji,
I.,
Hozawa,
A. &
Tomita,
H.
(2016b) Unemployment risk among individuals undergoing medical treatment for chronic diseases. Occup. Med. (Lond.), 66, 143-149.
-
Nakaya,
N.,
Narita,
A.,
Tsuchiya,
N.,
Nakamura,
T.,
Tsuji,
I.,
Hozawa,
A. &
Tomita,
H.
(2016c) Partners’ ongoing treatment for chronic disease and the risk of psychological distress after the Great East Japan Earthquake. Tohoku J. Exp. Med., 239, 307-314.
-
Nakaya,
N.,
Nemoto,
H.,
Yi,
C.,
Sato,
A.,
Shingu,
K.,
Shoji,
T.,
Sato,
S.,
Tsuchiya,
N.,
Nakamura,
T.,
Narita,
A.,
Kogure,
M.,
Sugawara,
Y.,
Yu,
Z.,
Gunawansa,
N.,
Kuriyama,
S.,
et al.(2018) Effect of tsunami drill experience on evacuation behavior after the onset of the Great East Japan Earthquake. Intl. J. Disaster Risk Reduct., 28, 206-213.
-
Seto,
M.,
Nemoto,
H.,
Kobayashi,
N.,
Kikuchi,
S.,
Honda,
N.,
Kim,
Y.,
Kelman,
I. &
Tomita,
H.
(2019) Post-disaster mental health and psychosocial support in the areas affected by the Great East Japan Earthquake: a qualitative study. BMC Psychiatry, 19, 261.
-
Shichigahama Town
(2014) The Great East Japan Earthquake Shichigahama Town Disaster Record Collection: Passing on to the Next Generation.
https://www.shichigahama.com/benricho/joho/documents/d89-010.pdf [Accessed: June 14, 2021] (in Japanese).
-
Soldatos,
C.R.,
Dikeos,
D.G. &
Paparrigopoulos,
T.J.
(2000) Athens Insomnia Scale: validation of an instrument based on ICD-10 criteria. J. Psychosom. Res., 48, 555-560.
-
Sone,
T.,
Sugawara,
Y.,
Tanji,
F.,
Nakaya,
N.,
Tomita,
H. &
Tsuji,
I.
(2021) The association between psychological distress and risk of incident functional disability in elderly survivors after the Great East Japan Earthquake: the mediating effect of lifestyle and bodily pain. J. Affect. Disord., 295, 552-558.
-
Suzuki,
T.,
Akaishi,
T.,
Nemoto,
H.,
Utsumi,
Y.,
Seto,
M.,
Usukura,
H.,
Kunii,
Y.,
Sugawara,
Y.,
Nakaya,
N.,
Nakamura,
T.,
Tsuchiya,
N.,
Narita,
A.,
Kogure,
M.,
Hozawa,
A.,
Tsuji,
I.,
et al. (2021) Impact of type of reconstructed residence on social participation and mental health of population displaced by disasters. Sci. Rep., 11, 21465.
-
Takahashi,
Y.,
Yoshizoe,
K.,
Ueki,
M.,
Tamiya,
G.,
Zhiqian,
Y.,
Utsumi,
Y.,
Sakuma,
A.,
Tsuda,
K.,
Hozawa,
A.,
Tsuji,
I. &
Tomita,
H.
(2020) Machine learning to reveal hidden risk combinations for the trajectory of posttraumatic stress disorder symptoms. Sci. Rep., 10, 21726.
-
Tanji,
F.,
Sugawara,
Y.,
Tomata,
Y.,
Watanabe,
T.,
Sugiyama,
K.,
Kaiho,
Y.,
Tomita,
H. &
Tsuji,
I.
(2017) Psychological distress and the incident risk of functional disability in elderly survivors after the Great East Japan Earthquake. J. Affect. Disord., 221, 145-150.
-
Tsuchiya,
M.,
Aida,
J.,
Hagiwara,
Y.,
Sugawara,
Y.,
Tomata,
Y.,
Sato,
M.,
Watanabe,
T.,
Tomita,
H.,
Nemoto,
E.,
Watanabe,
M.,
Osaka,
K. &
Tsuji,
I.
(2015) Periodontal disease is associated with insomnia among victims of the Great East Japan Earthquake: a panel study initiated three months after the disaster. Tohoku J. Exp. Med., 237, 83-90.
-
Tsuchiya,
N.,
Nakaya,
N.,
Nakamura,
T.,
Narita,
A.,
Kogure,
M.,
Aida,
J.,
Tsuji,
I.,
Hozawa,
A. &
Tomita,
H.
(2017) Impact of social capital on psychological distress and interaction with house destruction and displacement after the Great East Japan Earthquake of 2011. Psychiatry Clin. Neurosci., 71, 52-60.
-
Utsumi,
Y.,
Nemoto,
H.,
Nakaya,
N.,
Nakamura,
T.,
Tsuchiya,
N.,
Narita,
A.,
Kogure,
M.,
Suzuki,
T.,
Seto,
M.,
Katayanagi,
M.,
Okuyama,
J.,
Sakuma,
A.,
Honda,
N.,
Sugawara,
Y.,
Kaye-Kauderer,
H.,
et al. (2020) The impact of health consciousness on the association between walking durations and mental health conditions after a disaster: a cross-sectional study. Sports Med. Open, 6, 30.
-
Weiss,
D. (2004) The Impact of Event Scale-Revised. In Assessing psychological trauma and PTSD, 2nd. ed.,
edited by Wilson,
J.P. &
Keane,
T.M.
The Guilford Press, New York, NY, pp 168-189.