Abstract
This study aimed to investigate the effects of listening to Wolfgang Amadeus Mozart’s “Sonata for two pianos in D major, K448” and Johann Sebastian Bach’s “Brandenburg concerto No. 4 in G major, BWV1049” on the heart rate, blood pressure, and autonomic nervous activity. Seventeen healthy young adults were recruited as participants. All participants underwent a 10-minute rest, a 10-minute load test, and a triplicate 8-minute music listening process. Electrocardiograms were continuously measured from the measurement onset to completion. Moreover, the high-frequency (HF) component was extracted from the heart rate variability analysis as a measure of the parasympathetic nervous activity and the ratio of low frequency (LF) to HF as a measure of the sympathetic nervous activity. Blood pressure was also measured. There was a significant decrease in the heart rate after listening to both K448 and BWV1049, as well as in the silence state. Blood pressure did not significantly change in either case. Further, the LF/HF ratio significantly decreased after listening to BWV1049. Nevertheless, HF did not change after listening to either music. In conclusion, this study suggests that listening to K448 does not affect the heart rate, blood pressure, or autonomic nervous activity, whereas listening to BWV1049 may suppress the sympathetic nervous activity in healthy adults.
Introduction
Music therapy is defined by the American Music Therapy Association as the means to try to recover, maintain, and increase the psychological and physical health of people by listening to music or playing an instrument for therapeutic purposes (Abrams 2010). In the 1990s and thereafter, reports studying the possible effects of music therapy have been accumulated that cover a broad area such as physiological effects of music on heart rate (HR), blood pressure (BP), respiration, and temperature (Trappe 2010) or relief from cancer-related pain (Roy et al. 2008). Regarding the effects of music on autonomic nervous activity, Iwanaga et al. (2005) suggested that music-induced mood-relieving effects are accompanied by a predominance of the parasympathetic nervous activity.
Although various music genres are used in music therapy, Mozart’s works are especially considered to have a relaxing effect (Paugam-Burtz and Mantz 2007) and good for prenatal care (Osuch et al. 2009). Thus, the purported sound source of Mozart is being distributed as a commercial product worldwide. An attention to Mozart’s music was initially triggered by a report of Rauscher et al. (1993), in which healthy college students performed intelligence tests before and after listening to Wolfgang Amadeus Mozart’s Sonata for two pianos in D- major (K448). The group member who listened to K448 accomplished significantly higher test scores as compared to the member who listened to the text-reading or the member who took the rest in silence. Although this report by Rauscher et al. (1993) was thereafter called a “Mozart effect,” there are reports that either support or reject Rauscher’s notion. Newman et al. (1995) set out essentially similar experimental conditions as those of Rauscher et al. (1993), but found no significant difference in intelligent test scores between K448-listening, sentence reading-listening, and silence. On the other hand, Rideout et al. (1998) reported that listening to either K448 or contemporary music led to a significant increase in intelligence test scores in both groups of students, arguing the Mozart’s effect as a common factor present in music that contains fast-paced, high-register melodies. Furthermore, a third notion claims that Mozart’s music does not directly increase non-musical skills, but causes psychological arousal, and as a secondary effect may increase some performance ability (Thompson et al. 2001). Finally, Lin et al. (2013) reported that listening to K448 induces the predominance of the parasympathetic nervous activity. Therefore, Mozart’s music is generally considered to have a relaxation effect and bring a predominance of the parasympathetic nervous activity. As a matter of fact, not only Mozart’s music, but also other baroque music including Pachelbel’s Canon and Johan Sebastian Bach’s Brandenburg Concerto No. 4, G- major (BWV1049) are known to cause a predominance of the parasympathetic nervous activity (da Silva et al. 2014b; Matney 2017).
Here, when interpreting music effects, we may better keep in mind protocols of examination that were used in the previous studies. For example, in one study, participants were divided into three groups and each group member was exposed to either music, text-reading, or silence (Rauscher et al. 1993), whereas in the other study, participants were divided into two groups and each group member was exposed to either one genre of music or another very different genre of music (da Silva et al. 2014a). If taking these variations into consideration, some ambiguity still remains as to whether the so-called music effect is caused by music in general or by music in a particular genre, or by individual music. In the present study on a music effect, we tried to compare two music that had been used in the previous studies, which made it possible to compare our result with the preceding results. The music we chose are K448 and BWV1049 both of which belong to the same genre of classic. Furthermore, in our study, each participant was exposed to both K448 and BWV1049 serially, an approach different from the previous studies. Under this experimental condition, music effects were evaluated by simple physiological parameters, not by psychological parameters.
Methods
Participants
This study enrolled 17 healthy Japanese university students (11 females and 6 males) aged 20-40 years. The age of participants enrolled in this study was not substantially different from that in the preceding studies using Mozart’s music (Rauscher et al. 1993; Roque et al. 2013; Nakajima et al. 2016). Participants with the following conditions were excluded in the present study: past or current smoking; any history of respiratory, cardiovascular, or auditory diseases, as well as hypertension, diabetes, neurological disorder; and treatment with drugs that might influence the autonomic nervous system. All female participants had regular menstrual cycles; moreover, they were assessed when they were during the early follicular phases, which is within 10 days of the start of the menstrual cycle. This was to avoid the influence of estrogen and progesterone levels on the heart rate variability (HRV) (Tenan et al. 2014; Bao et al. 2016).
The participants were asked to refrain from drinking alcohol and caffeinated beverages for at least 12 hours before data collection (Vaschillo et al. 2008). Additionally, they were required to have 6 to 7 hours of sleep the night before, and to be fasting for more than 2 hours before the experiment.
All participants were informed of the objective and protocol of the study, and agreed to provide consent for participating in the study. This study was approved by the Ethics Committee of the Tohoku University Graduate School of Medicine (Approval No. 2018-1-288).
Mental workload
The outline of the experimental protocol is shown in Fig. 1. Before listening to music, the participants were exposed to mental stress during the loading state. They performed the reading-span-test (RST) as a mental workload test, which was comprised of double tasks such as reading sentences aloud and memorizing several words for 10 minutes (Kondo and Osaka 2000; Endo and Osaka 2012). RST aimed to induce the sympathetic tone to reevaluate the Mozart effect on physiological parameters, especially the autonomic nervous activity after a state of mental stress. In addition, the test was similar to an intelligence test. In the RST, several stimulus sentences were presented in a serial order during the reading phase. The participants read the stimulus sentences and were required to remember a designated target word. When a card containing none of the stimulus sentences was presented, the participants were required to answer the target word within 5 seconds.
Musical stimulation
After the mental workload was over, each participant listened to either W.A. Mozart’s Sonata for two Pianos, D- major, the 1st movement (K448) or J.S. Bach’s Brandenburg Concerto No. 4, G- major, the 1st movement (BWV1049) for 8 minutes or did not listen to any music and remained in silence. The participants wore earphones (SONY MDR-EX250; Tokyo, Japan) connected to a personal computer and were exposed to music at a sound level of 25% from the loudspeaker. Similarly, the participants wore earphones during the silence condition.
Experimental protocol
Data was collected in an air-conditioned quiet laboratory [ambient temperature and humidity were 23.8 ± 1.6℃ and 46.0 ± 4.9%, respectively, mean ± standard error of the mean (SE)] between 9:00 and 17:00. The daytime schedule was selected to minimize the effect of the circadian rhythm on the autonomic nervous system (Bilan et al. 2005; Becker et al. 2019). The participants were seated on a chair and equipped with 4 electrocardiogram (ECG) electrodes (RadarcircTM; Dainippon Pharmaceutical Co., Ltd., Osaka, Japan) on both sides of the anterior and lateral thoracic regions, as well as a digital sphygmomanometer (OMRON HEM-7420; Kyoto, Japan) on the right upper arm. The participants were instructed to relax with their eyes open and to avoid talking except when trying RST.
The participants were exposed to 3 different states serially as follows: a resting state for adapting to the experimental environment, then a loading state, and finally a listening-to-music state (Fig. 1). In detail, the participants first took a 10-minute rest for relaxation, and they were loaded by the RST for another 10 minutes. After the RST, the participants wore a canal earphone, listened to either K448 or BWV1049, or were kept in silence for 8 minutes. A cycle of resting, loading and listening was repeated three times in all participants. ECG was recorded for 94 minutes continuously, but the records from the first and last 5 minutes were excluded from the analysis. BP was measured immediately before after the RST and after listening to music. The respiratory rate was visually measured during the resting state. A case of respiratory rate of < 9 breaths per minute was excluded from the analysis, since such a lower respiratory rate may induce alterations in the HRV (Sasaki and Maruyama 2014).
HRV analysis
The sampling frequency for ECG signals was 1,000 Hz, and the data were analog-to-digital conversed and stored on a personal computer. The peak of the R wave in the recorded ECG signal was identified, and the consecutive R-R interval was measured. Sinus pause and atrial or ventricular arrhythmia were deleted.
Power spectral analysis was performed off-line with continuous wavelet transformation using FlucletTM WT Ver 4.0 (Dainippon Sumitomo Pharmaceutical Co., Ltd., Osaka, Japan). We obtained the low-frequency (LF) and high-frequency (HF) components as the area of the power spectral curve between 0.04 and 0.15 Hz and between 0.15 and 0.40 Hz, respectively. In this study, the ratio of LF over HF components (LF/HF) was used as an index of sympathetic nervous activity, whereas HF was used as an index of parasympathetic nervous activity (Karemaker 2017). The reliability of using the HRV in spectral analysis has been reported (Lehrer and Gevirtz 2014).
Statistical analysis
Data were analyzed using SPSS Statistics 24.0 (IBM Japan, Ltd., Tokyo, Japan). The normal Gaussian distribution of the data was verified using the Shapiro-Wilk goodness-of-fit test (z value of > 1.0). For parametric distributions, one-way repeated measures analysis of variance and multiple comparison tests were performed to compare each data. Values were expressed as mean ± SE. All p values were two-tailed with p < 0.05 being considered statistically significant.
Results
Characteristics of the participants
The age, height, weight, body mass index, and respiratory rate at the resting state of the 17 participants were 21.9 ± 0.4 years, 164.3 ± 2.5 cm, 58.6 ± 2.4 kg, 21.5 ± 2.5 kg/m2, and 12.9 ± 1.0 breaths/min, respectively. No one had a respiratory rate of < 9 breaths per minute. All these values were within the standard range for healthy adults (Table 1).
Effects of listening to music on HR and BP
Among the three conditions of silence, K448, and BWV1049, HRs at resting were within a similar range as shown in Fig. 2 (69.5 ± 2.1, 69.9 ± 2.2, and 70.6 ± 1.8 bpm, respectively). As expected, the RST-loading significantly increased HR to a similar extent in each condition (72.8 ± 1.8 in the silence, 73.8 ± 1.9 in the K448, and 73.1 ± 1.7 bpm in the BWV1049, respectively). Listening to K448 or BWV1049 decreased HR to 70.0 ± 1.9 or 69.2 ± 1.8 bpm, respectively. Reduction in HR from loading to listening was significant regardless of the type of music employed. Similarly, HR significantly returned to 69.2 ± 1.9 bpm under the silence condition. Therefore, the reduction in HR was likely due to a mere release from loading stress and not necessarily due to the music’s effects. On the other hand, not only the RST-loading state but also the listening to music state did not induce significant changes in systolic BP (SBP) as well as diastolic BP (DBP) (see Supplementary Fig. S1A, B).

The LF/HF ratio is an index of the sympathetic nervous activity, and the relevant data are presented in Fig. 3. In all 3 conditions of silence, K448, and BWV1049, the LF/HF values at the RST-loading state increased as compared to those at the resting state. However, statistically significant increases were only in the silence and BWV1049 conditions. As for the effect of listening, only BWV1049 decreased the LF/HF ratio significantly, whereas the silence and K448 conditions did not affect the LF/HF ratio. The values of LF/HF in the BWV1049 condition were 2.9 ± 0.7 at the resting state, 4.2 ± 0.9 at the RST-loading state, and 2.2 ± 0.6 at the listening state.
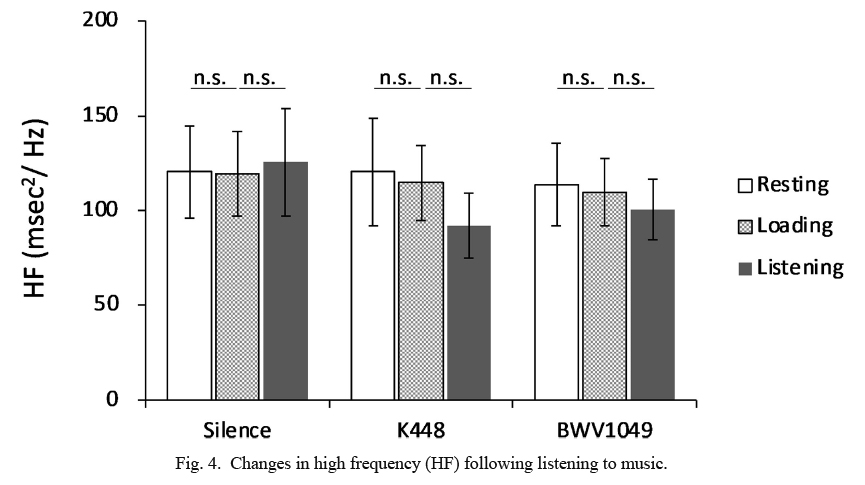
HF is an index of the parasympathetic nervous activity, and the relevant data are presented in Fig. 4. Not only the RST-loading state but also the listening-to-music state did not induce any significant change in HF.
Discussion
The circulatory function is regulated by the balance between the sympathetic and parasympathetic nervous activities and is also influenced by respiration. The HRV, a measurable indicator of the autonomic nervous activity, varies depending on age, respiration, sex hormones, and circadian rhythms (Sasaki and Maruyama 2014). Therefore, in this study, the participants’ age, respiratory rate, menstrual cycle, and the time of experiments were set as uniform as possible among the participants.
HR is generated by the spontaneous excitation of sinus nodes, which is regulated by the autonomic nervous activity. Specifically, the sympathetic nervous system, if placed under psychological stress, increases HR (Azam et al. 2016). In this study, participants’ HR significantly increased during the RST, which confirmed that RST acted as loading stress on the sympathetic nervous activity. When listening to music, one may unconsciously catch the rhythm of music and move their body in synchrony with the music (Henry et al. 2017). Both K448 and BWV1049 were allegro-specified (120-152 bpm) by their composers. This speed is faster than the HR of healthy adults (70-80 bpm). If the HR is tuned to adjust to the speed and rhythm of music, HR, when listening to K448 or BWV1049, is expected to increase as compared to the HR observed under RST-loading (72.8-73.8 bpm). Indeed, we found that HR rather decreased to 70.2 ± 1.9 bpm and 69.2 ± 1.8 bpm, when listening to K448 and BWV1049, respectively. The silence condition also decreased the HR to a similar extent as music. Therefore, the observed decrease in HR is not likely due to music and/or silence but due to relief from the RST-loading.
The psychosomatic stress also causes a predominance of the sympathetic nervous activity (von Rosenberg et al. 2017). Indeed, we observed that LF/HF, an index of the sympathetic nervous activity, showed an increasing tendency at the RST-loading state (statistically significant at least in the silence and BWV1049 conditions). Conversely, listening to music after a psychological loading leads to a predominance of the parasympathetic activity (Lee et al. 2016). However, in this study, there was no significant change in HF data, an index of the parasympathetic nervous activity, during resting, loading, and listening-to-music states. Thus, there was no predominance of the parasympathetic nervous activity when listening to either K448 or BWV1049.
Ferreira et al. (2015) reported that baroque and heavy metal music suppressed the sympathetic and parasympathetic activities, respectively. Suppression of the sympathetic nervous activity by baroque music is reported by do Amaral et al. (2016) as well. In this study, the LF/HF ratio was significantly decreased during listening to BWV1049, but not K448. Therefore, listening to some particular kind of baroque music, BWV1049 in this case, may reduce the sympathetic nervous activity. Since listening to classical music, in general, is reported to have a small impact on the autonomic nervous activity (Yagi et al. 2003; Hodges 2009), our observation that BWV1049 significantly decreased the LF/HF ratio might perhaps be an exceptional situation or the specialty of BWV1049.
There are some limitations in this study. We compared similar-sounding music clips and found that autonomic activity responded differently upon listening. However, we were unable to elucidate the mechanisms responsible for this difference. Moreover, this study could not evaluate musical preference because only two participants preferred classical music. Future research should examine how differences in musical structure or music preference affect changes in the autonomic nervous activity. In addition, the autonomic nervous activity has sex differences: the sympathetic nervous activity tends to be higher in males and the parasympathetic nervous activity in females. In this study, we analyzed males and females together, because each sample size in both sexes was small. There were no significant changes in the LF/HF ratio from the listening of BWV1049 to resting, when statistically analyzed in either the female group (n = 11) or the male group (n = 6). In addition, there was no significant difference in the response of the LF/HF ratio to the listening of K448 or BWV1049 between the female group and the male group.
In conclusion, this study suggests that listening to K448 and BWV1049 does not affect the heart rate, blood pressure, or parasympathetic nervous activity; however, only listening to BWV1049 may suppress the sympathetic nervous activity in healthy adults.
Conflict of Interest
The authors declare no conflict of interest.
References
-
Abrams,
B.
(2010) Evidence-based music therapy practice: an integral understanding. J. Music Ther., 47, 351-379.
-
Azam,
M.A.,
Katz,
J.,
Mohabir,
V. &
Ritvo,
P.
(2016) Individuals with tension and migraine headaches exhibit increased heart rate variability during post-stress mindfulness meditation practice but a decrease during a post-stress control condition - a randomized, controlled experiment. Int. J. Psychophysiol., 110, 66-74.
-
Bao,
S.,
Kanno,
E. &
Maruyama,
R.
(2016) Blunted autonomic responses and low-grade inflammation in Mongolian adults born at low birth weight. Tohoku J. Exp. Med., 240, 171-179.
-
Becker,
B.K.,
Zhang,
D.,
Soliman,
R. &
Pollock,
D.M.
(2019) Autonomic nerves and circadian control of renal function. Auton. Neurosci., 217, 58-65.
-
Bilan,
A.,
Witczak,
A.,
Palusinski,
R.,
Myslinski,
W. &
Hanzlik,
J.
(2005) Circadian rhythm of spectral indices of heart rate variability in healthy subjects. J. Electrocardiol., 38, 239-243.
-
da Silva,
A.G.,
Guida,
H.L.,
Antonio,
A.M.,
Marcomini,
R.S.,
Fontes,
A.M.,
Carlos de Abreu,
L.,
Roque,
A.L.,
Silva,
S.B.,
Raimundo,
R.D.,
Ferreira,
C. &
Valenti,
V.E.
(2014a) An exploration of heart rate response to differing music rhythm and tempos. Complement. Ther. Clin. Pract., 20, 130-134.
-
da Silva,
S.A.,
Guida,
H.L.,
Dos Santos Antonio,
A.M.,
de Abreu,
L.C.,
Monteiro,
C.B.M.,
Ferreira,
C.,
Ribeiro,
V.F.,
Barnabe,
V.,
Silva,
S.B.,
Fonseca,
F.L.A.,
Adami,
F.,
Petenusso,
M.,
Raimundo,
R.D. &
Valenti,
V.E.
(2014b) Acute auditory stimulation with different styles of music influences cardiac autonomic regulation in men. Int. Cardiovasc. Res. J., 8, 105-110.
-
do Amaral,
J.A.T.,
Guida,
H.L.,
de Abreu,
L.C.,
Barnabe,
V.,
Vanderlei,
F.M. &
Valenti,
V.E.
(2016) Effects of auditory stimulation with music of different intensities on heart period. J. Tradit. Complement. Med., 6, 23-28.
-
Endo,
K. &
Osaka,
M.
(2012) Individual difference in strategy use in the Japanese Reading Span Test. The Japanese Journal of Psychology, 82, 554-559.
-
Ferreira,
L.L.,
Vanderlei,
L.C.M.,
Guida,
H.L.,
de Abreu,
L.C.,
Garner,
D.M.,
Vanderlei,
F.M.,
Ferreira,
C. &
Valenti,
V.E.
(2015) Response of cardiac autonomic modulation after a single exposure to musical auditory stimulation. Noise Health, 17, 108-115.
-
Henry,
M.J.,
Herrmann,
B. &
Grahn,
J.A.
(2017) What can we learn about beat perception by comparing brain signals and stimulus envelopes? PLoS One, 12, e0172454.
-
Hodges,
D.A. (2009) Bodily responses to music. In Oxford Handbook of music Psychology, 1st ed.,
edited by Hallam,
S.,
Cross,
I. &
Thaut,
M.H, Oxford University Press, Oxford, England, pp.
121-130.
-
Iwanaga,
M.,
Kobayashi,
A. &
Kawasaki,
C.
(2005) Heart rate variability with repetitive exposure to music. Biol. Psychol., 70, 61-66.
-
Karemaker,
J.M.
(2017) An introduction into autonomic nervous function. Physiol. Meas., 38, R89-R118.
-
Kondo,
H. &
Osaka,
N.
(2000) Effect of concreteness of target words on verbal working memory: an evaluation using Japanese version of reading span test. The Japanese Journal of Psychology, 71, 51-56.
-
Lee,
K.S.,
Jeong,
H.C.,
Yim,
J.E. &
Jeon,
M.Y.
(2016) Effects of music therapy on the cardiovascular and autonomic nervous system in stress-induced university students: a randomized controlled trial. J. Altern. Complement. Med., 22, 59-65.
-
Lehrer,
P.M. &
Gevirtz,
R.
(2014) Heart rate variability biofeedback: how and why does it work? Front. Psychol., 5, 756.
-
Lin,
L.C.,
Chiang,
C.T.,
Lee,
M.W.,
Mok,
H.K.,
Yang,
Y.H.,
Wu,
H.C.,
Tsai,
C.L. &
Yang,
R.C.
(2013) Parasympathetic activation is involved in reducing epileptiform discharges when listening to Mozart music. Clin. Neurophysiol., 124, 1528-1535.
-
Matney, B. (2017) The effect of specific instrumentation on anxiety music students: a feasibility study. Arts Psychother., 54, 47-55.
-
Nakajima,
Y.,
Tanaka,
N.,
Mima,
T. &
Izumi,
S.I.
(2016) Stress recovery effects of high- and low-frequency amplified music on heart rate variability. Behav. Neurol., 2016, 5965894.
-
Newman,
J.,
Rosenbach,
J.H.,
Burns,
K.L.,
Latimer,
B.C.,
Matocha,
H.R. &
Vogt,
E.R.
(1995) An experimental test of “the Mozart effect”: does listening to his music improve spatial ability? Percept. Mot. Skills, 81, 1379-1387.
-
Osuch,
E.A.,
Bluhm,
R.L.,
Williamson,
P.C.,
Theberge,
J.,
Densmore,
M. &
Neufeld,
R.W.J.
(2009) Brain activation to favorite music in healthy controls and depressed patients. Neuroreport, 20, 1204-1208.
-
Paugam-Burtz,
C. &
Mantz,
J.
(2007) Sedative effects of Mozart’s music in the critically ill: enjoy the hormonal symphony. Crit. Care Med., 35, 2858-2859.
-
Rauscher,
F.H.,
Shaw,
G.L. &
Ky,
K.N.
(1993) Music and spatial task performance. Nature, 365, 611.
-
Rideout,
B.E.,
Dougherty,
S. &
Wernert,
L.
(1998) Effect of music on spatial performance: a test of generality. Percept. Mot. Skills, 86, 512-514.
-
Roque,
A.L.,
Valenti,
V.E.,
Guida,
H.L.,
Campos,
M.F.,
Knap,
A.,
Vanderlei,
L.C.M.,
Ferreira,
L.L.,
Ferreira,
C. &
Abreu,
L.C.
(2013) The effects of auditory stimulation with music on heart rate variability in healthy women. Clinics (Sao Paulo), 68, 960-967.
-
Roy,
M.,
Peretz,
I. &
Rainville,
P.
(2008) Emotional valence contributes to music-induced analgesia. Pain, 134, 140-147.
-
Sasaki,
K. &
Maruyama,
R.
(2014) Consciously controlled breathing decreases the high-frequency component of heart rate variability by inhibiting cardiac parasympathetic nerve activity. Tohoku J. Exp. Med., 233, 155-163.
-
Tenan,
M.S.,
Brothers,
R.M.,
Tweedell,
A.J.,
Hackney,
A.C. &
Griffin,
L.
(2014) Changes in resting heart rate variability across the menstrual cycle. Psychophysiology, 51, 996-1004.
-
Thompson,
W.F.,
Schellenberg,
E.G. &
Husain,
G.
(2001) Arousal, mood, and the Mozart effect. Psychol. Sci., 12, 248-251.
-
Trappe,
H.J.
(2010) The effects of music on the cardiovascular system and cardiovascular health. Heart, 96, 1868-1871.
-
Vaschillo,
E.G.,
Bates,
M.E.,
Vaschillo,
B.,
Lehrer,
P.,
Udo,
T.,
Mun,
E.Y. &
Ray,
S.
(2008) Heart rate variability response to alcohol, placebo, and emotional picture cue challenges: effects of 0.1-Hz stimulation. Psychophysiology, 45, 847-858.
-
von Rosenberg,
W.,
Chanwimalueang,
T.,
Adjei,
T.,
Jaffer,
U.,
Goverdovsky,
V. &
Mandic,
D.P.
(2017) Resolving ambiguities in the LF/HF ratio: LF-HF scatter plots for the categorization of mental and physical stress from HRV. Front. Physiol., 8, 360.
-
Yagi,
R.,
Nishina,
E.,
Honda,
M. &
Oohashi,
T.
(2003) Modulatory effect of inaudible high-frequency sounds on human acoustic perception. Neurosci. Lett., 351, 191-195.