Abstract
Background:
The aim of this study was to evaluate the clinical feasibility of simultaneous acquisition of rest 99mTc-tetrofosmin/stress 201Tl dual-isotope single-photon emission computed tomography with a semiconductor gamma camera.
Methods and Results:
Ninety-four patients with known or suspected coronary artery disease (CAD) were enrolled in the study. First, patients were injected with 99mTc-tetrofosmin (296 MBq) for rest imaging, followed by 201Tl (74 MBq) injection during 6 min of vasodilator stress test. Immediately after the stress test, the patients underwent the first electrocardiogram (ECG)-gated simultaneous acquisition including rest and stress perfusion scans. Patients were brought back for the second simultaneous acquisition for the comparison of ECG-gated wall motion between stress and rest scan 30 min later. Coronary angiography was performed in all the patients within 3 months of this protocol. Sensitivity, specificity and accuracy on a per patient basis to detect significant coronary artery stenosis (≥75%) were 88.6%, 79.2% and 86.2%, respectively. Per coronary vessel, sensitivity, specificity and accuracy were as follows: 84.9%, 80.5% and 83% in the left anterior descending coronary artery; 75%, 93.1% and 86.2% in the left circumflex coronary artery; and 74.2%, 85.7% and 81.9% in the right coronary artery.
Conclusions:
Simultaneous acquisition of rest 99mTc-tetrofosmin/stress 201Tl dual-isotope protocol had high diagnostic accuracy for significant CAD. (Circ J 2016; 80: 689–695)
Stress myocardial perfusion single-photon emission computed tomography (MPS) is the standard diagnostic modality in patients with known or suspected coronary artery disease (CAD).1–4
Stress-induced myocardial ischemia and left ventricular (LV) functional parameters are markers of future cardiac events.5–7
Moreover, recent clinical guidelines recommend ≥10% myocardial ischemia in the LV as an indication for coronary revascularization.8
Precise diagnosis and quantification using MPS would facilitate this.
Technical features of the recently developed semiconductor gamma camera include high spatial resolution, high sensitivity and high energy-spectrum resolution. This type of gamma camera has cadmium-zinc-telluride (CZT) detectors and direct conversion of scintillation without NaI crystal. The CZT gamma camera is also expected to improve image contrast, provide multi-isotope imaging, faster scan and short acquisition time.9
A novel dedicated cardiac scanner, the D-SPECT (Spectrum Dynamics, Caesarea, Israel), has 9 CZT detectors (40×160 mm) with square-hole tungsten collimators. In our previous experiment, D-SPECT had 1.6- and 1.4-fold better full width at half maximum (FWHM) in both 99mTc and 201Tl line-sources than the conventional anger gamma camera, respectively. Regarding photon count sensitivity, D-SPECT also had 5.03- and 6.31-fold higher photon count·s–1·MBq–1
for the 99mTc and 201Tl sources than the conventional anger gamma camera, respectively.
According to the 2013 survey of Japanese Circulation Society, 72,500 exercise and 128,000 vasodilator stress MPS were carried out.10
One of the reasons for this difference would be staff shortage in clinical practice. Therefore, physicians who work in the stress laboratory may prefer to use vasodilator stress in order to reduce the stress test time. The high extraction fraction (85%) of 201Tl in vasodilator stress would be ideal to visualize myocardial perfusion in the area of hyperemic condition.11
Therefore, 201Tl may be slightly more effective in identifying mild coronary stenosis. Combination of vasodilator stress and 201Tl is physically compatible and clinically useful for effective time management. 99mTc-labelled myocardial perfusion tracers such as sestamibi and tetrofosmin have a low extraction fraction (54–62%), potentially causing a mild myocardial perfusion defect that could be missed.11–13
Conversely, the difference in extraction fraction between 99mTc-labelled tracer and 201Tl is smaller in the resting condition than in the hyperemic condition. Previously, Berman et al carried out a sequential acquisition of rest 201Tl/stress 99mTc-sestamibi dual-isotope protocol in 1993, which could visualize the combined assessment of stress perfusion and myocardial viability.14
They used 92–133 MBq 201Tl for rest and 740–1,110 MBq 99mTc-sestamibi for stress imaging. The higher radiation exposure and lower cost-effectiveness of this protocol were not conducive to good cost containment. Recently, they proposed sequential acquisition rest 99mTc-sestamibi/stress 201Tl dual-isotope MPS with semiconductor gamma camera.15–17
In that recent study, they proposed the utilization of low-dose tracers (74–92.5 MBq 201Tl for stress and 296–370 MBq 99mTc-sestamibi for rest), followed by the sequential scanning.
In the present study, we developed a novel MPS protocol using low-dose rest 99mTc-tetrofosmin/stress 201Tl with simultaneous acquisition of dual-isotope protocol (SDI protocol) using D-SPECT and validated its clinical application.
Methods
Patients
We enrolled 94 consecutive patients with known or suspected CAD between 1 April and 30 June 2015, who had invasive coronary angiography (CAG) due to the SPECT results or physician recommendation. Patients with high-grade atrioventricular block or bronchial asthma were excluded. Patients were asked to discontinue nitrates and caffeine for 24 h prior to the study.
MPS and Stress Protocol
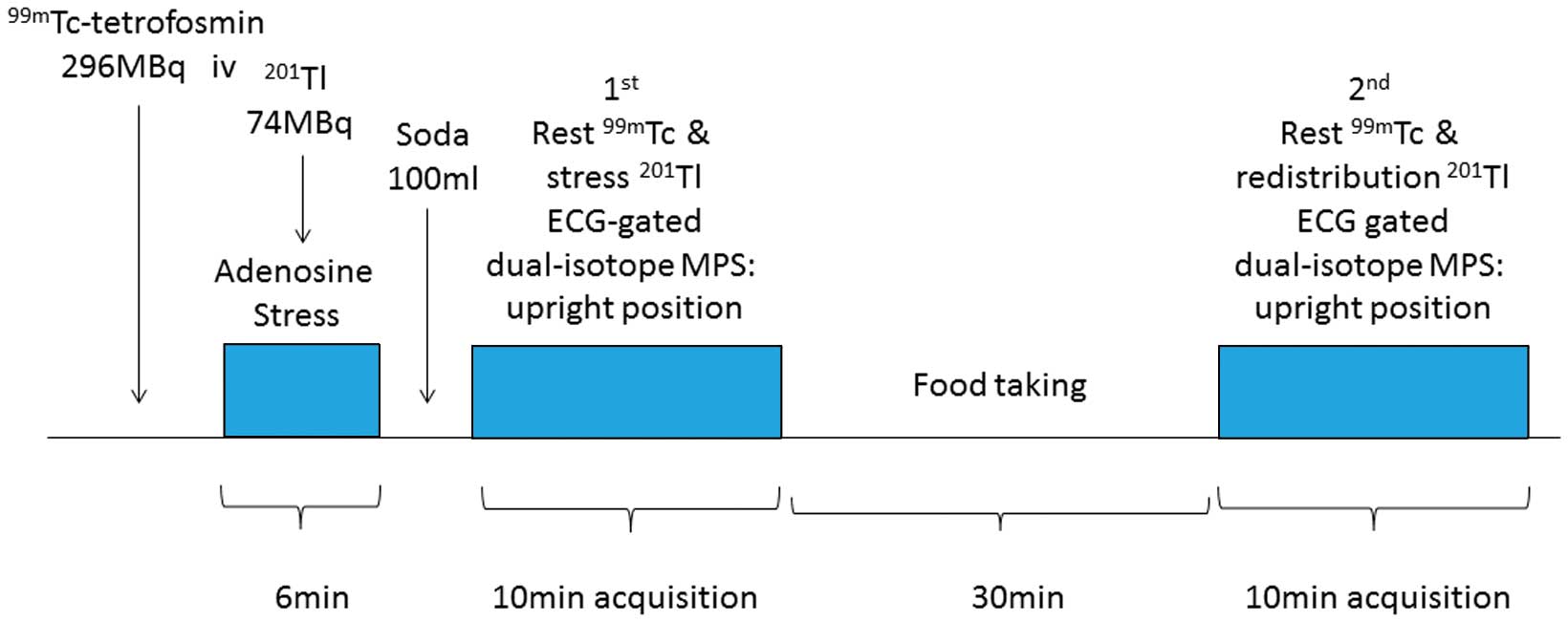
This novel protocol is shown in
Figure 1. First, patients were injected with 296 MBq 99mTc-tetrofosmin (Nihon Medi-Physics, Tokyo, Japan) at the time of calibration for visualizing resting perfusion. After the injection of 99mTc-tetrofosmin, patients then underwent 6 min of adenosine stress (120 μg·kg–1·min–1; Adenoscan injection, Daiichi Sankyo, Tokyo, Japan). Seventy-four MBq 201Tl was injected 3 min after the start of adenosine infusion. Prior to the first acquisition, patients were asked to drink 100 ml of soda in order to produce the space between the heart and subdiaphragmatic activity.18
The first simultaneous rest 99mTc-tetrofosmin/stress 201Tl acquisition (10 min) was started after the end of adenosine stress in an upright position. The second simultaneous rest 99mTc-tetrofosmin/redistribution 201Tl acquisition (10 min) was then done 30 min after the first acquisition (Figure 1). Calculated total protocol time was 1 h. This novel protocol was approved by the hospital’s ethics committee, and informed consent was given by all patients.
To carry out simultaneous acquisition of rest 99mTc-tetrofosmin/stress 201Tl MPS, the subtraction of photo-energy cross-talk between 99mTc-tetrofosmin and 201Tl is a major problem. Although down-scatter of the 140 keV 99mTc photons into the main 201Tl window (70 keV) is a major problem, the much better energy resolution of CZT detectors as compared with the conventional anger camera allows the use of narrower energy windows, thereby reducing down-scatter contribution and effective scatter correction.19
Briefly, the iterative deconvolution method developed by Kacperski et al was used for the calibrations of D-SPECT, which was a hybrid between the triple energy window method and scatter modelling based on spatial and spectral distribution of projection counts in multiple selected energy windows.19
The selected photopeak windows of 99mTc and 201Tl were as follows: 130–150 keV for 99mTc, and 64–77 keV and 157.4–177.4 keV for 201Tl, respectively.19
Scatter correction via the iterative deconvolution method was applied to the 201Tl images.
Acquisition Protocol and Image Reconstruction
Sixteen-frame electrocardiogram (ECG)-gated MPS data were acquired using D-SPECT. A 10-s prescan was performed to set the heart position and define limits of scanning angle for each detector. Each image dataset was acquired with 120 projections per detector. Transaxial images were reconstructed using the proprietary Broadview reconstruction algorithm (Spectrum Dynamics), which is based on the maximum likelihood expectation maximization method.16
SPECT images (short axis, horizontal and vertical long axis) were generated using Autoquant (Cedars-Sinai Medical Center, Los Angeles, CA, USA).20
Image Interpretation
The SPECT images were scored semi-quantitatively by 2 experienced readers using a 17-segment model of the LV on a 5-point scale (0, normal uptake; 1, mildly reduced uptake; 2, moderately reduced uptake; 3, severely reduced uptake; 4, almost no uptake).14,21
Discordance in image interpretation was resolved by consensus. In this model, the left anterior descending coronary artery (LAD) territory consists of 8 segments (segments 1, 2, 5–7, 11, 12, 17), the left circumflex coronary artery (LCX) consists of 5 segments (segments 4, 9, 10, 15, 16) and the right coronary artery (RCA) consists of 4 segments (segments 3, 8, 13, 14). Summed stress score (SSS), summed rest score (SRS) and summed difference score (SDS) were calculated as previously defined by Berman et al.22
Jeopardized myocardium was defined as SDS ≥2 in the relevant coronary vessels.23
Summed regional wall motion score (SWMS) was derived from a 6-point scale scoring system (0, normal; 1, mildly reduced; 2, moderately reduced; 3, severely reduced; 4, akinesis; and 5, dyskinesis) at both rest and stress.24
Transient ischemic dilation (TID) ratio was also calculated using the following equation: end-diastolic LV volume at stress divided by that at rest.25
Image Quality Score
99mTc-tetrofosmin concentration at rest imaging located below the diaphragm may cause an artifactual perfusion defect in the adjacent inferior walls. This phenomenon is known as the liver-heart artifact.26,27
Therefore, we evaluated the image quality of the short-axis rest and stress SPECT images using a 3-point scale: excellent image quality with no liver uptake; good image quality with small liver uptake; and poor image quality with perfusion defect in the inferior wall by adjacent liver uptake.
Statistical Analysis
Continuous variables are expressed as mean±SD. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and accuracy in detecting significant CAD on a per patient or coronary vessel basis were calculated using the usual equations. Receiver operating characteristic (ROC) curve analysis for detection of significant CAD was performed, and ROC area under the curve (AUC) was calculated. Unpaired t-test was used for the evaluation for TID ratio between the normal coronary group and the multi (2 or 3)-vessel group. Paired t-test was used for the evaluation of end-diastolic volume (EDV), ejection fraction (EF) and SWMS between stress and rest.
CAG
All patients underwent invasive CAG within 3 months after MPS. Significant CAD was defined as stenosis (≥75%) in one or more coronary arteries or ≥75% in the left main coronary artery (LMCA).
Results
Patient Characteristics
Patient characteristics are given in
Table 1. All patients completed the protocol. Classical coronary risk factors and clinical symptoms were as follows: hypertension, 81%; dyslipidemia, 64%; diabetes, 55%; current smoking, 21%. Average body mass index was 24.1±3.8 kg/m2. ECG at rest is also listed in
Table 1.
Table 1.
Patient Characteristics
| |
Mean±SD or n (%) |
| n |
94 |
| Age |
69.5±9.8 |
| Male |
77 (82) |
| Height (cm) |
164.5±8.9 |
| Body weight (kg) |
65.6±13.0 |
| BMI (kg/m2) |
24.1±3.8 |
| Hypertension |
77 (81) |
| Dyslipidemia |
61 (64) |
| Diabetes |
52 (55) |
| Current smoking |
20 (21) |
| CKD |
30 (31) |
| Prior AMI |
29 (31) |
| Prior PCI |
46 (49) |
| Abnormal Q wave |
14 (15) |
| ST-T change |
19 (20) |
| AF |
7 (7) |
AF, atrial fibrillation; AMI, acute myocardial infarction; BMI, body mass index; CKD, chronic kidney disease; PCI, percutaneous coronary intervention.
Averaged SSS, SRS and SDS were as follows: 7.0±6.1, 2.3±4.3 and 4.6±4.4, respectively. LVEF was lower at stress (57.8±15.8%) than at rest (60.5±16.5%, P<0.0001), and EDV was larger at stress (99.3±48.6 ml) than at rest (94.4±49.4 ml, P<0.0001). TID ratio in all subjects was 1.06±0.10. TID ratios in the normal coronary group, the single-vessel group and the multi-vessel group were calculated as follows: 1.02±0.10, 1.07±0.07 and 1.08±0.11, respectively. The multi-vessel group had a tendency toward higher TID ratio than the normal coronary group (P=0.0609). The difference in SWMS between stress and rest was not statistically significant (6.37±11.6 vs. 5.98±11.1, P=0.0602;
Table 2).
Table 2.
Myocardial Perfusion and ECG-Gated Parameters
| |
Mean±SD or n (%) |
| n |
94 |
| SSS |
7.0±6.1 |
| SRS |
2.3±4.3 |
| SDS |
4.6±4.4 |
| EF at stress (%) |
57.8±15.8* |
| EF at rest (%) |
60.5±16.5 |
| EDV at stress (ml) |
99.3±48.6** |
| EDV at rest (ml) |
94.4±49.4 |
| TID ratio in all subjects |
1.06±0.10 |
| TID ratio in normal coronary group |
1.02±0.10 |
| TID ratio in single vessel group |
1.07±0.07 |
| TID ratio in multi (2 or 3)-vessel group |
1.08±0.11*** |
| SWMS at stress |
6.37±11.6**** |
| SWMS at rest |
5.98±11.1 |
*P<0.0001, paired t-test between stress and rest EF; **P<0.0001, paired t-test between stress and rest EDV; ***P=0.0609, unpaired t-test of TID ratio between normal coronary group vs. multi-vessel group; ****P=0.0602, paired t-test between stress and rest SWMS. ECG, electrocardiogram; EDV, end-diastolic volume; EF, ejection fraction; SDS, summed difference score; SRS, summed rest score; SSS, summed stress score; SWMS, summed wall motion score; TID, transient ischemic dilation ratio.
Among 94 patients with invasive CAG, 35 had single-vessel disease, 20 had 2-vessel disease, and 16 had 3-vessel disease (Table 3). Regarding the prevalence of CAD, 53 had significant stenosis of the LAD, 39 had significant stenosis of the LCX, 31 had significant stenosis of the RCA and 1 had significant stenosis in the LMCA.
Table 3.
Angiographic Findings
| Significant stenosis |
≥90% |
89–75% |
| LAD (n=53) |
21 (39) |
32 (61) |
| LCX (n=39) |
17 (43) |
22 (57) |
| RCA (n=31) |
18 (58) |
13 (42) |
Data given as n (%). LAD, left anterior descending coronary artery; LCX, left circumflex coronary artery; RCA, right coronary artery.
201Tl (stress) and 99mTc-tetrofosmin (rest) had 0% and 2% poor image quality, respectively (Table 4).
Table 4.
Image Quality Score
| |
Excellent |
Good |
Poor |
| Stress 201Tl |
85 (90) |
9 (10) |
0 (0) |
| Rest 99mTc-tetrofosmin |
26 (28) |
66 (70) |
2 (2) |
Per patient analysis, sensitivity, specificity, PPV, NPV and accuracy were as follows: 88.6%, 79.2%, 92.5%, 70.4% and 86.2%, respectively. With regard to coronary vessels, the data were as follows: 84.9%, 80.5%, 84.9%, 80.5% and 83.0% for LAD; 75.0%, 93.1%, 87.1%, 85.7% and 86.2% for LCX; and 74.2%, 85.7%, 71.9%, 87.1% and 81.9% for the RCA (Figure 2). ROC AUC was 0.908 on a per patient basis; and with regard to the coronary arteries, it was 0.848 for the LAD; 0.835 for the LCX; and 0.813 for the RCA (Figure 3). Sensitivity to detect significant stenosis in 36 patients with multi-vessel disease was 97%.
Representative Cases
A 71-year-old man with dyspnea on exertion was referred for adenosine stress SDI protocol. The patient had a history of dyslipidemia and hypertension. MPS on SDI protocol showed a moderate amount of jeopardized myocardium in the mid-distal anteroseptal wall extending to the apex in the LAD territory (Figure 4). Invasive CAG then showed 75% stenosis in the proximal LAD coronary artery.
Discussion
To our knowledge, this is the first study of simultaneous acquisition rest 99mTc-tetrofosmin/stress 201Tl MPS with D-SPECT. 99mTc-tetrofosmin and 201Tl are the most commonly used isotopes to reflect myocardial perfusion in Japan. These isotopes have different features, as follows. 201Tl has a long half-life (73 h), a property of redistribution and high extraction fraction linearly associated with hyperemic blood flow compared with 99mTc-tetrofosmin. Conversely, 99mTc-tetrofosmin has a short half-life (6 h) and lower extraction fraction than 201Tl. Utilization of 99mTc-tetrofosmin instead of 99mTc-sestamibi in SDI protocol is due to its faster clearance from the liver. More rapid clearance of 99mTc-labeled tracer would be important in the short waiting time between the injection and first acquisition.28
Previously, a sequential acquisition method has been used in the conventional dual-isotope protocol (201Tl for rest and 99mTc-sestamibi for stress) for eliminating down-scatter of 99mTc-sestamibi into the lower energy window of 201Tl.14,29
High-dose 99mTc-sestamibi was necessary for higher quality of stress images in order to assess myocardial perfusion abnormality and ECG-gated parameters with the conventional anger camera. The newly developed SDI protocol with D-SPECT, however, has several improved features.
First, the high sensitivity of semiconductor detectors facilitates low radiation exposure. The SDI protocol uses one-third of 99mTc-tetrofosmin and two-thirds of 201Tl compared with the conventional dual-isotope protocol.14
The use of low-dose 99mTc-tetrofosmin due to higher photon count with the semiconductor camera decreases the down-scatter contribution from 99mTc-tetrofosmin to the 201Tl window, and improved the 201Tl image quality. The conventional dual-isotope MPS (111 MBq 201Tl and 740 MBq 99mTc-sestamibi) resulted in an effective dose of almost 30 mSv. This SDI protocol using 74 MBq 201Tl and 296 MBq 99mTc-tetrofosmin, however, delivers an effective dose <12 mSv, which is similar to the regular 1-day 99mTc-sestamibi protocol.30,31
We propose a reduced dose of 1 MBq/kg for 201Tl and 3 MBq/kg for 99mTc-tetrofosmin isotope when used with the sensitive D-SPECT camera. This may lower radiation exposure and should be confirmed in the future.
Second, the short examination time increases patient throughput and facilitates high satisfaction. All the patients were able to follow the SDI protocol without any complaints. A total examination time of 60 min is acceptable in the regular clinical setting. Six SDI protocols are routinely available from 9 to 12 o’clock in the laboratory. We used a second simultaneous acquisition for the calculation of TID ratio and observation of LV wall motion.21
TID ratio is a well known marker of severe and extensive myocardial ischemia or jeopardized myocardium.32,33
We believe that TID ratio and stress-induced myocardial stunning, reflected by SWMS, would be useful to diagnose the presence of ischemic or jeopardized myocardium. Regarding these variables, there was a tendency toward a difference between the normal coronary group and multi-vessel group. The reasons for this are as follows: (1) the relatively short waiting time between the first and second acquisition; and (2) the lack of myocardial stunning due to the lower severity of SDS, compared with the previous study.34
Conversely, Emmett et al reported that the TID phenomenon with vasodilator stress was not associated with stunning of wall motion or ventricular enlargement, but was more likely a function of subendocardial hypoperfusion and impaired coronary flow reserve.35
This supports the present unexpected results regarding both TID ratio and SWMS in the SDI protocol with vasodilator stress. Moreover, if physicians did not need TID ratio or changes of wall motion between stress and rest scan in clinical reading, the second acquisition might not be necessary.36
A simple first simultaneous acquisition only protocol may contribute to reduce total examination time to 20 min. (The total examination time for sequential acquisition dual-isotope protocol [stress 201Tl and rest 99mTc-sestamibi] with D-SPECT documented by Berman et al was estimated at 24 min.)
In addition, completely identical attenuation due to body position is guaranteed with simultaneous acquisition. If the heart drifts during the acquisition, the same artifactual perfusion defect would be created in the same location of the heart. This phenomenon suggests the need for clinical reading in order to cancel out the motion artifacts.
Third, regular MPS includes supine and prone position imaging, reducing attenuation of inferior walls.37,38
Given the much lower image attenuation with D-SPECT, single position imaging in the upright position would be useful. Upright imaging would also be appropriate to separate the heart and subdiaphragmatic activity (eg, liver or bowel uptake) with assistance of gastric bubble using soda.18
Single position imaging would therefore reduce total examination time and increase patient satisfaction.
Fourth, the image quality score of 201Tl at stress was sufficient in the SDI protocol, but the 99mTc-tetrofosmin images were sometimes disturbed by extracardiac uptake of liver. In these cases, comparison between first and second acquisition of 99mTc-tetrofosmin images would be helpful to eliminate the extracardiac uptake, but further analysis is required.
Comparison of Diagnostic Performance
Although the hardware and protocol were different, diagnostic performance in the detection of significant CAD using another CZT gamma camera (Discovery NM 530c, GE healthcare, Haifa, Israel) was reported by Tanaka et al as follows: 76–85% sensitivity, 69–85% specificity and 74–81% accuracy on a per vessel basis.3
Of course, the subject group was also completely different between the 2 studies. Diagnostic performance is similar, but the advantages of the SDI protocol and D-SPECT are as follows: shorter total examination time (<1 h with the SDI protocol vs. 4 h with 201Tl scan with NM 530c) and single position imaging (upright only scan with D-SPECT vs. supine and prone position scans with NM 530c).
Study Limitations
Although the TID phenomenon is associated with jeopardized myocardium or impaired coronary flow reserve, the relatively short waiting time (30 min) between the first and second acquisitions in the SDI protocol is not sufficient to show a difference in this between the 2 acquisitions. Further validation of the threshold for TID ratio in the SDI protocol is therefore needed.
Conclusions
Simultaneous acquisition rest 99mTc-tetrofosmin/stress 201Tl dual-isotope protocol with D-SPECT facilitates high-speed MPS, lower radiation exposure and precise diagnostic accuracy compared with sequential dual-isotope scans.
Acknowledgments
We thank Ms Hibiko Ode, Ms Dalia Sheety and Mr Yoshitaka Hori for their assistance.
References
- 1.
Hachamovitch R, Berman DS, Kiat H, Cohen I, Cabico JA, Friedman J, et al. Exercise myocardial perfusion SPECT in patients without known coronary artery disease: Incremental prognostic value and use in risk stratification. Circulation 1996; 93: 905–914.
- 2.
Underwood SR, Anagnostopoulos C, Cerqueira M, Ell PJ, Flint EJ, Harbinson M, et al. Myocardial perfusion scintigraphy: The evidence. Eur J Nucl Med Mol Imaging 2004; 31: 261–291.
- 3.
Tanaka H, Chikamori T, Tanaka N, Hida S, Igarashi Y, Yamashita J, et al. Diagnostic performance of a novel cadmium-zinc-telluride gamma camera system assessed using fractional flow reserve. Circ J 2014; 78: 2727–2734.
- 4.
Shiraishi S, Sakamoto F, Tsuda N, Yoshida M, Tomiguchi S, Utsunomiya D, et al. Prediction of left main or 3-vessel disease using myocardial perfusion reserve on dynamic thallium-201 single-photon emission computed tomography with a semiconductor gamma camera. Circ J 2015; 79: 623–631.
- 5.
Matsumoto N, Sato Y, Suzuki Y, Kunimasa T, Yoda S, Iida J, et al. Prognostic value of myocardial perfusion single-photon emission computed tomography for the prediction of future cardiac events in a Japanese population: A middle-term follow-up study. Circ J 2007; 71: 1580–1585.
- 6.
Matsumoto N, Sato Y, Suzuki Y, Kasama S, Nakano Y, Kato M, et al. Incremental prognostic value of cardiac function assessed by ECG-gated myocardial perfusion SPECT for the prediction of future acute coronary syndrome. Circ J 2008; 72: 2035–2039.
- 7.
Sharir T, Kang X, Germano G, Bax JJ, Shaw LJ, Gransar H, et al. Prognostic value of poststress left ventricular volume and ejection fraction by gated myocardial perfusion SPECT in women and men: Gender-related differences in normal limits and outcomes. J Nucl Cardiol 2006; 13: 495–506.
- 8.
Windecker S, Kolh P, Alfonso F, Collet JP, Cremer J, Falk V, et al. 2014 ESC/EACTS Guidelines on myocardial revascularization: The Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS): Developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur Heart J 2014; 35: 2541–2619.
- 9.
Tanaka H, Chikamori T, Hida S, Uchida K, Igarashi Y, Yokoyama T, et al. Comparison of myocardial perfusion imaging between the new high-speed gamma camera and the standard anger camera. Circ J 2013; 77: 1009–1017.
- 10.
Matsumoto N, Hirayama A. Clinical value of high duke treadmill score with myocardial perfusion SPECT. J Nucl Cardiol
2015 June 27, doi:10.1007/s12350-015-0187-3.
- 11.
Husain SS. Myocardial perfusion imaging protocols: Is there an ideal protocol? J Nucl Med Technol 2007; 35: 3–9.
- 12.
Marshall RC, Leidholdt EM Jr, Zhang DY, Barnett CA. Technetium-99 m hexakis 2-methoxy-2-isobutyl isonitrile and thallium-201 extraction, washout, and retention at varying coronary flow rates in rabbit heart. Circulation 1990; 82: 998–1007.
- 13.
Primeau M, Taillefer R, Essiambre R, Lambert R, Honos G. Technetium 99 m SESTAMIBI myocardial perfusion imaging: Comparison between treadmill, dipyridamole and trans-oesophageal atrial pacing “stress” tests in normal subjects. Eur J Nucl Med 1991; 18: 247–251.
- 14.
Berman DS, Kiat H, Friedman JD, Wang FP, van Train K, Matzer L, et al. Separate acquisition rest thallium-201/stress technetium-99 m sestamibi dual-isotope myocardial perfusion single-photon emission computed tomography: A clinical validation study. J Am Coll Cardiol 1993; 22: 1455–1464.
- 15.
Berman DS, Kang X, Tamarappoo B, Wolak A, Hayes SW, Nakazato R, et al. Stress thallium-201/rest technetium-99 m sequential dual isotope high-speed myocardial perfusion imaging. JACC Cardiovasc Imaging 2009; 2: 273–282.
- 16.
Sharir T, Ben-Haim S, Merzon K, Prochorov V, Dickman D, Berman DS. High-speed myocardial perfusion imaging initial clinical comparison with conventional dual detector anger camera imaging. JACC Cardiovasc Imaging 2008; 1: 156–163.
- 17.
Patton JA, Slomka PJ, Germano G, Berman DS. Recent technologic advances in nuclear cardiology. J Nucl Cardiol 2007; 14: 501–513.
- 18.
Matsumoto N, Sato Y, Suzuki Y, Yoda S, Kunimasa T, Kato M, et al. Usefulness of rapid low-dose/high-dose 1-day 99 mTc-sestamibi ECG-gated myocardial perfusion single-photon emission computed tomography. Circ J 2006; 70: 1585–1589.
- 19.
Kacperski K, Erlandsson K, Ben-Haim S, Hutton BF. Iterative deconvolution of simultaneous 99 mTc and 201Tl projection data measured on a CdZnTe-based cardiac SPECT scanner. Phys Med Biol 2011; 56: 1397–1414.
- 20.
Sharir T, Germano G, Waechter PB, Kavanagh PB, Areeda JS, Gerlach J, et al. A new algorithm for the quantitation of myocardial perfusion SPECT. II: Validation and diagnostic yield. J Nucl Med 2000; 41: 720–727.
- 21.
Yoda S, Sato Y, Matsumoto N, Tani S, Takayama T, Nishina H, et al. Incremental value of regional wall motion analysis immediately after exercise for the detection of single-vessel coronary artery disease: Study by separate acquisition, dual-isotope ECG-gated single-photon emission computed tomography. Circ J 2005; 69: 301–305.
- 22.
Berman DS, Kang X, Van Train KF, Lewin HC, Cohen I, Areeda J, et al. Comparative prognostic value of automatic quantitative analysis versus semiquantitative visual analysis of exercise myocardial perfusion single-photon emission computed tomography. J Am Coll Cardiol 1998; 32: 1987–1995.
- 23.
Sharir T, Germano G, Kang X, Lewin HC, Miranda R, Cohen I, et al. Prediction of myocardial infarction versus cardiac death by gated myocardial perfusion SPECT: Risk stratification by the amount of stress-induced ischemia and the poststress ejection fraction. J Nucl Med 2001; 42: 831–837.
- 24.
Wahba FF, Dibbets-Schneider P, Bax JJ, Bavelaar-Croon CD, Zwinderman AH, Pauwels EK, et al. Detection of residual wall motion after myocardial infarction by gated technetium-99 m tetrofosmin SPET: A comparison with contrast ventriculography. Eur J Nucl Med 2001; 28: 514–521.
- 25.
Abidov A, Bax JJ, Hayes SW, Hachamovitch R, Cohen I, Gerlach J, et al. Transient ischemic dilation ratio of the left ventricle is a significant predictor of future cardiac events in patients with otherwise normal myocardial perfusion SPECT. J Am Coll Cardiol 2003; 42: 1818–1825.
- 26.
Germano G, Chua T, Kiat H, Areeda JS, Berman DS. A quantitative phantom analysis of artifacts due to hepatic activity in technetium-99 m myocardial perfusion SPECT studies. J Nucl Med 1994; 35: 356–359.
- 27.
Nuyts J, Dupont P, Van den Maegdenbergh V, Vleugels S, Suetens P, Mortelmans L. A study of the liver-heart artifact in emission tomography. J Nucl Med 1995; 36: 133–139.
- 28.
Jain D, Wackers FJ, Mattera J, McMahon M, Sinusas AJ, Zaret BL. Biokinetics of technetium-99m-tetrofosmin: Myocardial perfusion imaging agent: Implications for a one-day imaging protocol. J Nucl Med 1993; 34: 1254–1259.
- 29.
Groutars RG, Verzijlbergen JF, Zwinderman AH, Tiel-Van Buul MM, Ascoop CA, van Hemel NM, et al. Incremental prognostic value of myocardial SPET with dual-isotope rest (201)Tl/stress (99 m)Tc-tetrofosmin. Eur J Nucl Med Mol Imaging 2002; 29: 46–52.
- 30.
Henzlova MJ, Duvall WL. Return of dual-isotope SPECT myocardial perfusion imaging?: Not so fast. J Nucl Cardiol 2015; 22: 523–525.
- 31.
ICRP. Radiation dose to patients from radiopharmaceuticals: Addendum 3 to ICRP Publication 53: ICRP Publication 106: Approved by the Commission in October 2007. Ann ICRP 2008; 38: 1–197.
- 32.
Mazzanti M, Germano G, Kiat H, Kavanagh PB, Alexanderson E, Friedman JD, et al. Identification of severe and extensive coronary artery disease by automatic measurement of transient ischemic dilation of the left ventricle in dual-isotope myocardial perfusion SPECT. J Am Coll Cardiol 1996; 27: 1612–1620.
- 33.
Abidov A, Berman DS. Transient ischemic dilation associated with poststress myocardial stunning of the left ventricle in vasodilator stress myocardial perfusion SPECT: True marker of severe ischemia? J Nucl Cardiol 2005; 12: 258–260.
- 34.
Hida S, Chikamori T, Tanaka H, Igarashi Y, Hatano T, Usui Y, et al. Diagnostic value of left ventricular function after adenosine triphosphate loading and at rest in the detection of multi-vessel coronary artery disease using myocardial perfusion imaging. J Nucl Cardiol 2009; 16: 20–27.
- 35.
Emmett L, Ng A, Ha L, Russo R, Mansberg R, Zhao W, et al. Comparative assessment of rest and post-stress left ventricular volumes and left ventricular ejection fraction on gated myocardial perfusion imaging (MPI) and echocardiography in patients with transient ischaemic dilation on adenosine MPI: Myocardial stunning or subendocardial hypoperfusion? J Nucl Cardiol 2012; 19: 735–742.
- 36.
Ueyama T, Takehana K, Maeba H, Iwasaka T. Prognostic value of normal stress-only technetium-99 m myocardial perfusion imaging protocol. Comparison with standard stress-rest protocol. Circ J 2012; 76: 2386–2391.
- 37.
Hayes SW, De Lorenzo A, Hachamovitch R, Dhar SC, Hsu P, Cohen I, et al. Prognostic implications of combined prone and supine acquisitions in patients with equivocal or abnormal supine myocardial perfusion SPECT. J Nucl Med 2003; 44: 1633–1640.
- 38.
Nishina H, Slomka PJ, Abidov A, Yoda S, Akincioglu C, Kang X, et al. Combined supine and prone quantitative myocardial perfusion SPECT: Method development and clinical validation in patients with no known coronary artery disease. J Nucl Med 2006; 47: 51–58.



