Editorials
Clinical Features of Long QT Syndrome in Children
2016 Volume 80 Issue 3 Pages 598-600


Details
2016 Volume 80 Issue 3 Pages 598-600
Long QT syndrome (LQTS) is a genetic channelopathy with prolonged ventricular repolarization of the myocardial cells, associated with severe cardiac events such as syncope, aborted cardiac arrest, and sudden cardiac death.1 Children with LQTS have more serious risk factors than adults. As noted in a consensus report, patients with syncope or cardiac arrest before the age of 7 years, or patients who have syncope or cardiac arrest in the first year of life, are thought to be at high risk.2 This Editorial Comment focuses on the recent issues of LQTS in children.
Article p 696
Prevalence of LQTS in InfantsThe prevalence of congenital LQTS in infants is reported to be 1:2534 (0.039%) in Caucasians,3 and 4:4285 (0.093%) in Japanese.4 The reasonable cutoff value of the long QT interval in infants is reported to be 470 ms (31 of 43,080; 0.07%3 or 5 of 4,285; 0.12%4), and 460 ms (59 of 43,080; 0.14%3, or 8 of 4,285; 0.19%4), respectively, in those studies.
The genetic variant was identified in 12 of 28 neonates (43%),3 and in 1 of 3 infants (33%)4 with a QTc interval >470 ms. KCNQ1 mutations were found in 8 patients,3 and KCNH2 mutations were found in 43 and 14 patients, respectively. On Okinawa island, 17 of 23 children were identified as gene-positive LQTS by school-based ECG screening; 14 of them had SCN5A E1784K mutations.5 The prevalence of LQT3 is much higher than on any other island in Japan.
ECG Screening for InfantsThe efficacy of ECG screening of infants and children is controversial. Saul et al reported that ECG screening is cost-effective in preventing sudden infant death syndrome, as well as sudden death in childhood, using a cutoff value of the QTc interval of 460 ms,6 but Skinner and Van Hare reported that ECG screening is an unreliable diagnostic tool, and should only be performed to detect probands and to screen family members because most of the deaths from LQTS occur in patients who have had previous symptoms.7
ECG Characteristics of LQTS in Fetuses and NeonatesThe characteristic features of the ECG in fetal and neonatal LQTS are sinus bradycardia or atrioventricular block (AVB).8–10 The baseline fetal heart rate in sinus rhythm is significantly lower in fetal LQTS (range 90–144 beats/min, mean 118.9±13.3 beats/min) than in normal fetuses (range 125–147 beats/min, mean 141.0±9.4 beats/min; P<0.0001).8 LQTS is strongly suggested if the fetal heart rate is less than the 3rd percentile.11 In addition to a low baseline heart rate, nonreactive heart rate patterns are also suggestive in LQTS fetuses and may be explained by lower-than-normal right sympathetic cardiac activity or a blunted response to a sympathetic drive, as seen postnatally.8
LQTS with 2:1 AVB is commonly observed during the fetal and neonatal periods,9,10 but rarely observed in childhood and adulthood. In neonates with LQT2 and LQT3, 2:1 AVB was observed in 55% and 83% of the patients, respectively (Figure 1).10 AVB may be caused by functional block of the ventricle, because of prolongation of the ventricular refractory period, and in the majority of patients the atrioventricular conduction returns with a significant decrease in the QTc interval during the follow-up period.8 That may explain the rare occurrence of AVB in older children and adults with LQTS.
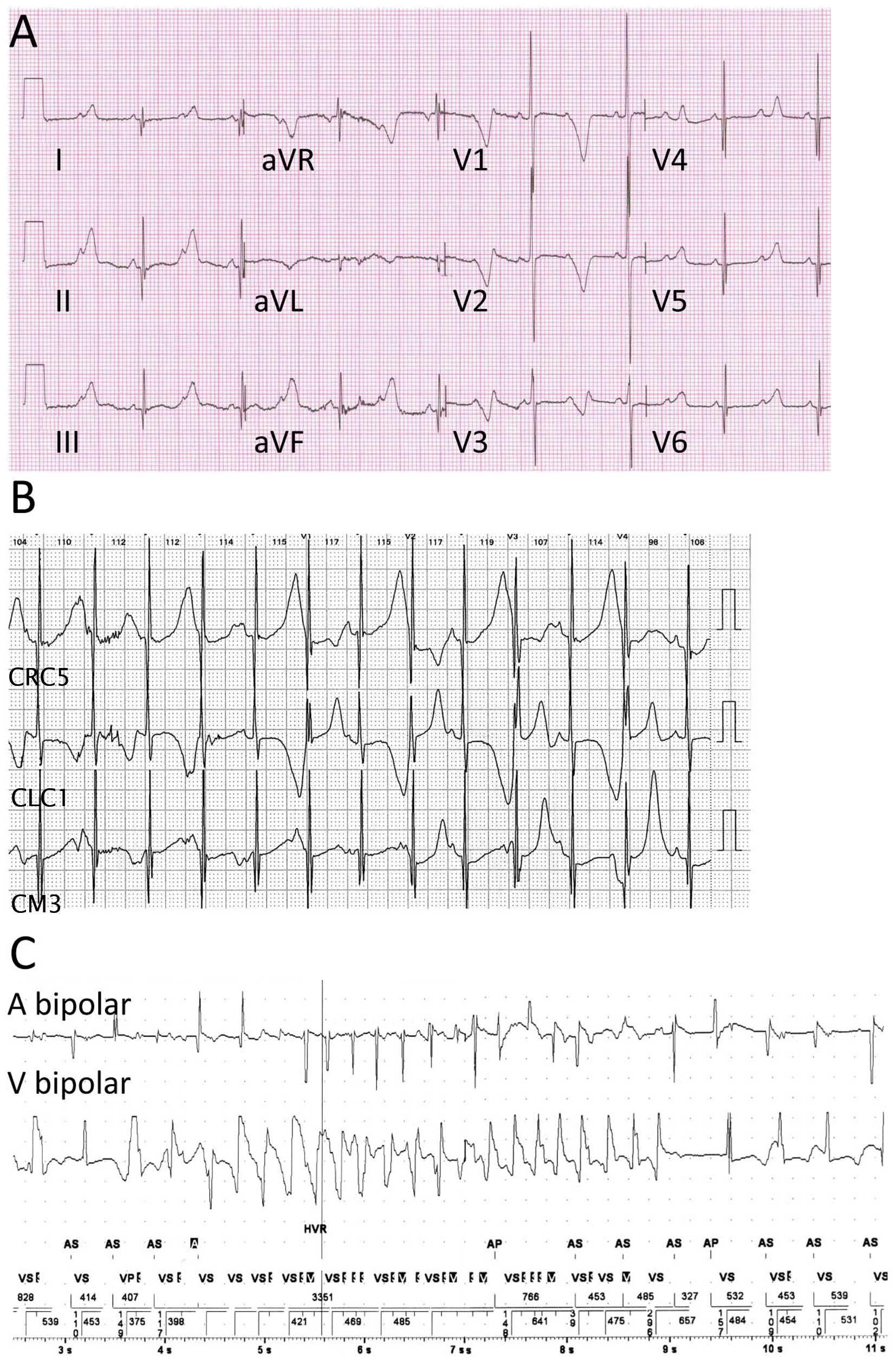
ECG of a 1-year-old male infant with long QT syndrome. (A) 2:1 atrioventricular block (AVB). The QT interval is prolonged to 630 ms, and the QTc interval is also prolonged to 685 ms. Prolongation of the ventricular refractory period resulted in 2:1 AVB with a ventricular rate of 71 beats/min. (B) Holter recording at 4 years old, shows 1:1 atrioventricular conduction with overt T wave alternance. (C) Recording from a pacemaker shows typical torsade de pointes in the same boy at 4 years old.
Previous reports showed that males with LQTS before the age of 15 years have a significant increased risk of syncope, aborted cardiac arrest, and sudden cardiac death.12 However, the risk of these cardiac events is inverted after the age of 14 years.12 Comparing the genotype of LQTS carriers, LQT1 females have a significantly lower risk of cardiac events than LQT1 males ≤15 years old (hazard ratio (HR) 0.58; P=0.005), but a significantly higher risk of cardiac events than males between the ages of 16 and 40 years (HR 3.35; P=0.007) (Figure 2).13 LQT2 and LQT3 children show no significant differences between male and female carriers. Females with LQT2 have a significantly higher risk of a first cardiac event than males between the ages of 16 and 40 years (HR 3.71; P=0.010).13 During 0–12 years old, males with LQT1 have the highest rate of a first syncope episode (P<0.001), but within the age range of 13–20 years, LQT2 females experience the highest rate of both first and subsequent syncope events (P<0.001 and P=0.01).14

Cumulative probability of the first cardiac event in long QT syndrome carriers aged ≤15 years (Left panels) and 16–40 years (Right panels). See further discussion in the text. (Adapted with permission from Zareba W, et al.13)
In this issue of the Journal, Ozawa et al15 report that the LQT2 phenotype presents with more frequent cardiac arrests or repetitive torsade de points (TdP) episodes than the LQT1 phenotype. They also demonstrate that LQT2 females have a repeat TdP episode within a short time period after a prior TdP episode, especially after puberty. As they note in their literature, the effect of estrogen, which prolongs the action potential duration (APD) through the inhibition of IKr, may contribute to the high occurrence of TdP in LQT2 females after adolescence.
A high occurrence of cardiac events in LQT1 males during childhood is also reported.13–15 Male children may be more vigorous than females, which may result in them having more frequent cardiac events than females. Testosterone shortens the APD through enhancement of IKs, which may explain the decrease in the cardiac events after adolescence in LQT1 males.
Recent Issues of LQTS in ChildrenAttention deficit/hyperactivity disorder (ADHD) is a relatively common disease and is prevalent in approximately 11% of children. ADHD-directed stimulant therapy (methylphenidate, dextroamphetamine/amphetamine, lisdexamfetamine, and dexmethylphenidate) is relatively contraindicated in patients with LQTS because of the possibility of LQTS-triggered cardiac events. During a mean follow-up of 7.9±5.4 years after the initiation of ADHD medication, the cumulative probability of cardiac events in the ADHD treatment group was 62% vs. 28% in the matched LQTS control group (P<0.001).16 Time-dependent use of ADHD medication is associated with an increased risk of cardiac events (HR 3.07; P=0.03).16 Syncope is the most common symptom and the risk is higher in males.
Remuneration to the author for attending meetings, and presentations, being payment for the time and effort of attending the activity, by Ono Pharmaceutical Co Ltd and Medtronic Co Ltd.