Abstract
Background:
When an internal iliac artery (IIA) has to be embolized during endovascular aneurysm repair (EVAR), buttock claudication sometimes poses problems. However, there is no established method to evaluate intraoperative blood flow to the gluteal muscles.
Methods and Results:
Gluteal regional oxygen saturation (rSO2) was monitored using near-infrared spectroscopy (NIRS) during surgery, and changes in rSO2
were compared with treatment results. Twenty-seven patients who underwent EVAR and IIA embolization at our institution between April 2019 and May 2020 were included in this study. The association between intraoperative changes in rSO2
and postoperative incidence of buttock claudication was analyzed. Furthermore, the presence or absence of communication between the superior and inferior gluteal arteries and the intraoperative changes in rSO2
were compared to ascertain whether rSO2
reflects blood flow change. Postoperative buttock claudication occurred in 4 of 19 patients (21%) with unilateral occlusion of IIA and in 4 of 8 patients (50%) with bilateral occlusion of IIAs. rSO2
was found to decrease significantly further in patients with buttock claudication than in patients without buttock claudication (−15±12% vs. −4±16%, P<0.05). In addition, rSO2
was predominantly lower in patients without the communication between the superior and inferior gluteal arteries than in those with the communication.
Conclusions:
Gluteal rSO2
is useful as an indicator of intraoperative gluteal blood flow.
In cases of abdominal aortic aneurysms, it is common for the lesion to extend into the iliac artery and form a series of aneurysms. Unilateral and bilateral iliac aneurysms are associated with 40% of abdominal aortic aneurysm cases.1–3
Endovascular aneurysm repair (EVAR) for such cases requires internal iliac artery embolization to prevent type II endoleak from the internal iliac artery. Although it has been reported that pelvic visceral ischemia and buttock claudication may occur even with unilateral embolization of the internal iliac artery, there is no method of intraoperative blood flow assessment of the internal iliac artery system.4–6
Editorial p 351
Previous studies reported that muscle oxygenation and blood flow to regions including the gluteal muscle could be successfully evaluated using near-infrared spectroscopy (NIRS), which enables the comparison of subjects with different adipose tissue thicknesses by physiological calibration.7,8
The purpose of this study was to evaluate the usefulness of NIRS for monitoring the regional oxygen saturation (rSO2) of gluteal artery blood flow during EVAR by comparing changes in rSO2
with treatment results.
Methods
Of the 86 patients who underwent EVAR at our institution between April 2019 and May 2020, 27 patients were included and 2 bedridden patients with a Clinical Frailty Score of ≥7 were excluded from 29 patients with concomitant internal iliac artery embolization. Intraoperative changes in the rSO2
and postoperative incidence of buttock claudication were compared, and an assessment was performed to determine if changes in rSO2
are predictive of buttock claudication. Furthermore, the presence or absence of communication between the superior and inferior gluteal arteries, as well as the intraoperative changes in rSO2, were compared, and analysis was performed to determine whether the change in blood flow to the gluteal muscles at the site of embolization of the internal iliac artery was reflected by rSO2.
An INVOS 5100C oximeter (Medtronic) was used to measure rSO2. The sensor was placed symmetrically at the level of the supracaudal border 5 cm from the center line, and rSO2
was monitored continuously in the gluteal tissue and recorded at the start of anesthesia, at the start of surgery, at the end of embolization, at the end of surgery, and at the end of anesthesia.
Stent grafting was performed using a corporate stent graft. During internal iliac artery embolization, we embolized the central part of the internal iliac artery as much as possible to preserve flow in the superior and inferior gluteal arteries. However, we embolized the peripheral part of the internal iliac artery or the superior and inferior gluteal arteries if there was a complication of an internal iliac artery aneurysm. After embolization was completed, the sheath was replaced with a large-caliber sheath, and the stent graft was implanted. In general, the operation was performed under general anesthesia, but in cases of hypopnea, the operation was performed under local anesthesia. The presence or absence of gluteal claudication was determined by interviewing patients at hospital discharge and at the first outpatient visit after hospital discharge.
The NIRS INVOS 5100C oximeter is equipped with 2 light-emitting diodes that emit near-infrared light at 2 different wavelengths (730 and 810 nm) and 2 photodiodes that detect transmitted light, and signals from 2 photoreceptors located at different distances (3 and 4 cm) from the light emitter are used to determine signal information such as shallow skin. The rSO2
value denotes the oxygen saturation of blood in microvessels, and the local perfusion state can be evaluated by determining the change in the local oxygen demand and supply balance.7,9,10
Statistical Analysis
The data are expressed as the mean±standard deviation, and the chi-squared test was used for statistical analysis. P<0.05 was considered to be statistically significant.
Results
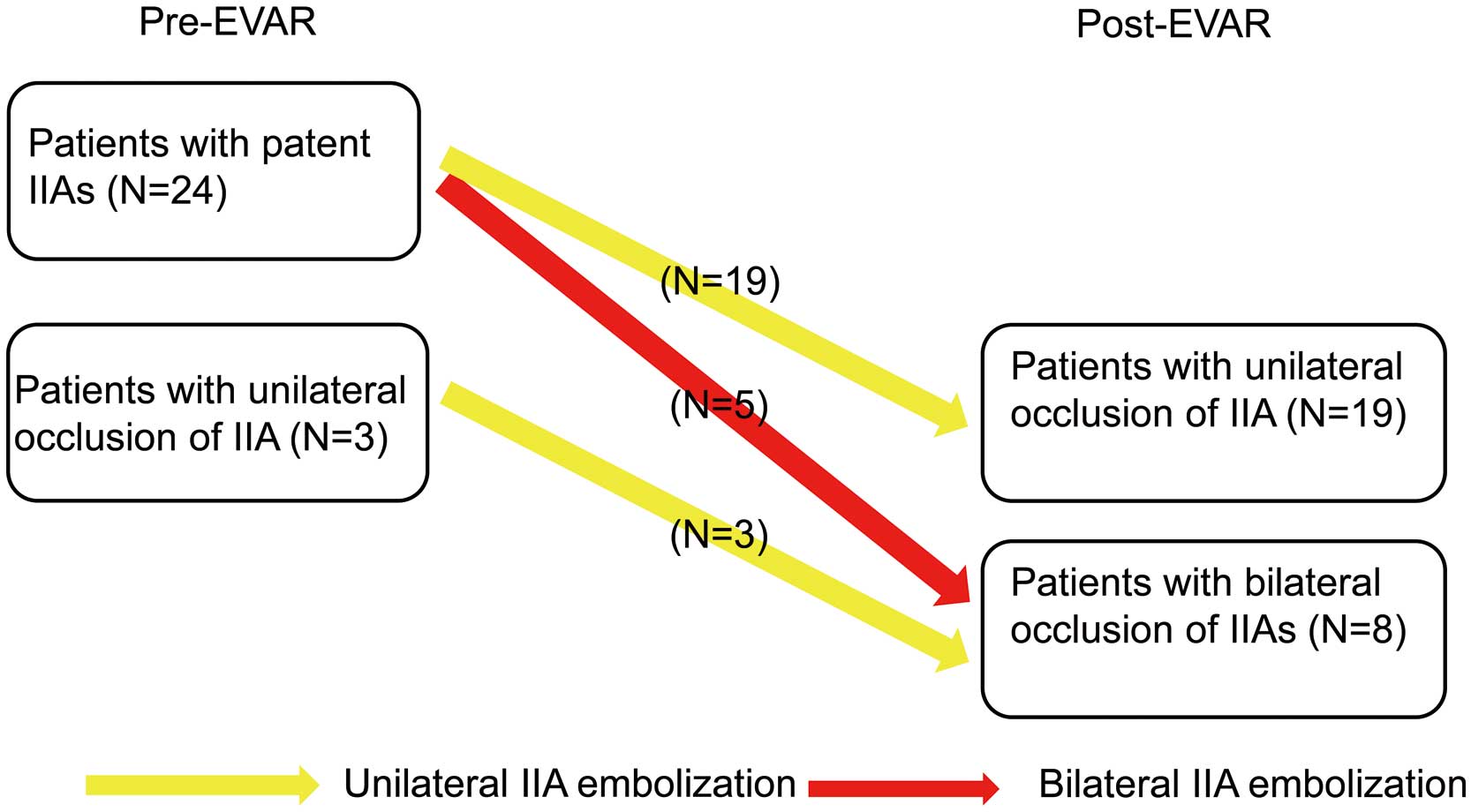
The mean age of the patients was 76±7 years, and 20 patients (74%) were men. The mean body weight was 60±13 kg, and the mean body mass index was 23±4 kg/m2. Eleven patients had an abdominal aortic aneurysm, 15 patients had an internal iliac aneurysm, and 1 patient had an abdominal aortic aneurysm with an internal iliac aneurysm. The mean maximum diameters of the abdominal aortic and internal iliac aneurysms were 52±10 and 39±10 mm, respectively (Table). Unilateral internal iliac artery embolization was performed in 22 patients and bilateral internal iliac artery embolization was performed in 5 patients. One patient underwent embolization with a plug and a coil, and 26 patients underwent embolization with only a coil. Three patients had unilateral internal iliac artery occlusion before surgery (Figure 1). The following devices were used: EXCLUDER C3 (W.L. Gore & Associates, USA) in 18 patients (67%), ENDURANT (Medtronic, USA) in 2 patients (7%), AFX (Endologix, Inc., USA) in 6 patients (22%), and Aorfix (Lombard Medical, Inc., USA) in 1 patient (4%). Iliac branch endoprosthesis (IBE; W.L. Gore & Associates, USA) was used in 2 patients, and we were able to preserve the internal iliac artery in both patients. Including patients with preoperative occlusion of the iliac artery, there were 19 patients with unilateral internal iliac artery occlusion and 8 patients with bilateral internal iliac artery occlusion (5 patients underwent bilateral embolization, and 3 patients underwent unilateral embolization and contralateral occlusion) (Figure 1). Buttock claudication was observed in 4 patients (21%) with unilateral occlusion and in 4 patients (50%) with bilateral occlusion (Figure 2). The communication between the superior and inferior gluteal arteries was preserved in 8 of the 22 patients (36%) who underwent unilateral embolization. Of the patients who underwent bilateral embolization, the communication was preserved bilaterally in 1 patient and unilaterally in 2 of 3 patients, but there was bilateral non-preservation of the communication in 1 patient (Figure 3). It was observed that rSO2
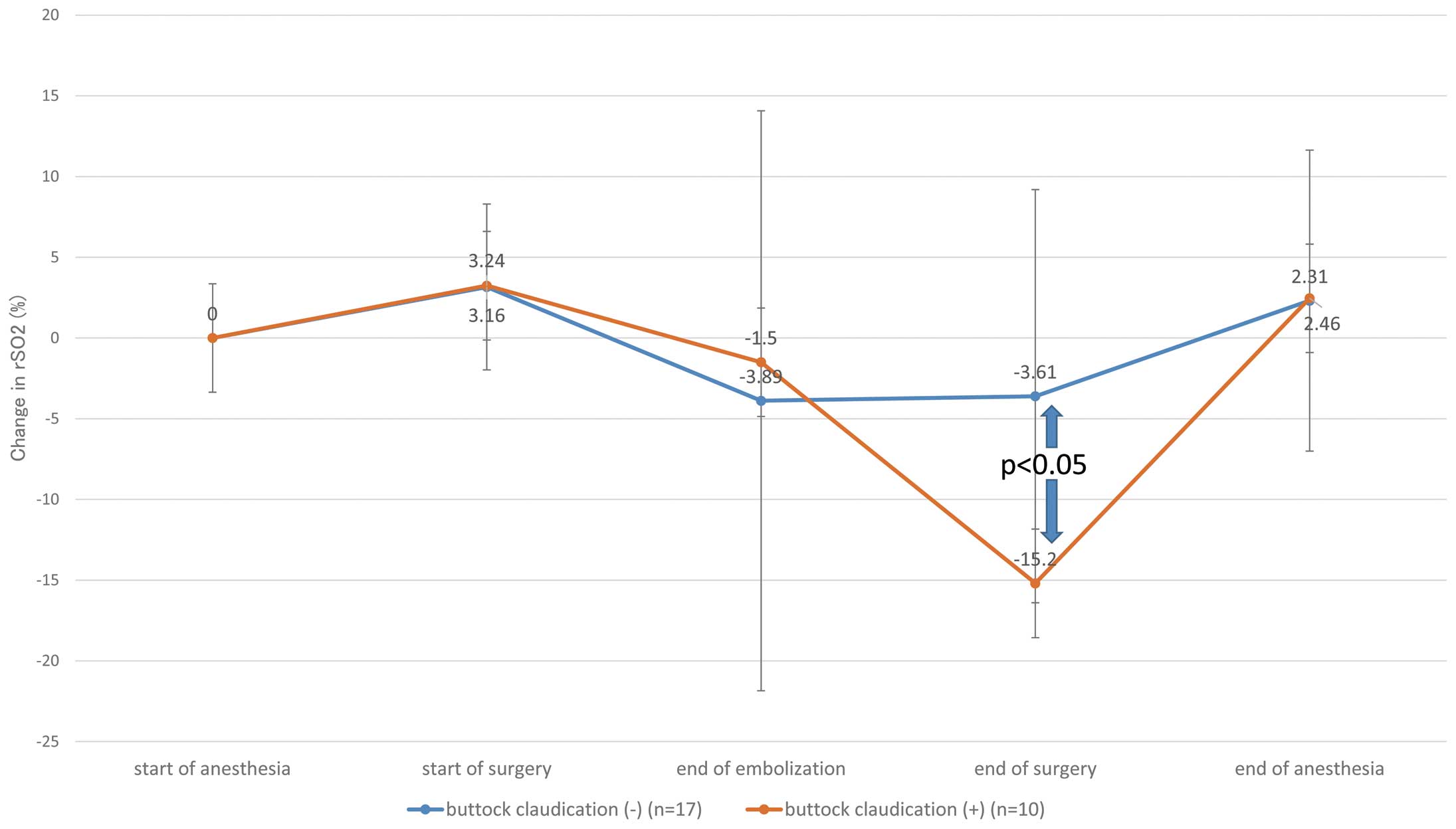
on the side of the proposed embolization began to decrease at the time of coil embolization, decreased most at the end of surgery, and recovered slowly at the end of anesthesia. The mean rSO2
values during EVAR in patients with and without buttock claudication were −15±12% and −4±16%, respectively (P<0.05) (Figure 4). The mean rSO2
values of patients with and without preserved communication between the superior and inferior gluteal arteries were 0±10% and −12±14%, respectively (P<0.05) (Figure 5). There was no case of intestinal ischemia or perioperative death.
Table.
Patient Characteristics
| Characteristics |
Values |
| Number of patients (n) |
27 |
| Age (years) |
76±7 |
| Gender, male |
20 |
| BW (kg) |
60±13 |
| BMI (kg/m2) |
23±4 |
| Clinical Frailty Score |
3±1 |
| Hypertension (%) |
22 (76) |
| Hyperlipidemia (%) |
9 (31) |
| Diabetes mellitus (%) |
2 (7) |
| Smoker (%) |
11 (38) |
| Maximum diameter of aortic aneurysm (mm) |
52±10 |
| Maximum diameter of iliac aneurysm (mm) |
39±10 |
| Devices used (n) |
| Excluder C3 (IBE) |
18 (2) |
| Endurant |
2 |
| AFX |
6 |
| Aorfix |
1 |
| Unilateral IIA embolization (n) |
22 |
| Bilateral IIAs embolization (n) |
5 |
BMI, body mass index; BW, body weight; IBE, iliac branch endoprosthesis; IIA, internal iliac artery.
Discussion
When abdominal aortic aneurysms are accompanied by iliac artery aneurysms, EVAR is performed with internal iliac artery embolization. However, it has been reported that pelvic visceral ischemia and buttock claudication can occur even with unilateral internal iliac artery embolization.5
Internal iliac artery embolization causes buttock claudication in ~30% of patients.3–6
Although there are many reports of improvement in claudication symptoms in the follow-up period, many patients are believed to suffer from persistent ischemic symptoms.6
However, there is no indication criteria for internal iliac artery reconstruction. For patients with unilateral internal iliac artery occlusion who require contralateral or bilateral embolization, it is reasonable to try to preserve blood flow as much as possible in the peripheral part of the internal iliac artery. High technical success rates and good short-term results have been reported with IBE;11–14
however, internal iliac artery occlusion of nearly 7% has also been reported in medium-term results.12
Anatomical unsuitability for IBE has also been reported in nearly 40% of patients.12,14
In this study, we measured rSO2
in the buttocks as an indicator of blood flow in the internal iliac artery. The collateral network concept proposed by Grippe et al states that all collateral vessels around the spinal cord affect spinal cord perfusion, and NIRS is used to measure the rSO2
of the spinal cord and its collateral vessels, which reflects the state of spinal cord perfusion.15–19
Similarly, we propose that continuous monitoring of rSO2
is useful for monitoring gluteal perfusion. It is rare for a single iliac artery to become severely ischemic because of a single occlusion, as the inferior mesenteric artery, the contralateral internal iliac artery, and the deep femoral artery form a network to maintain blood flow, and rSO2
in the gluteal tissues is considered a reflection of the perfusion status of this internal iliac artery system. It has been reported that coil embolization at the proximal part of the internal iliac artery can reduce the incidence of buttock claudication by preserving the communication between the superior and inferior gluteal arteries.5,6,20
In this study, rSO2
was found to be predominantly lower in the patient group without preserved communication; this suggests that blood flow in the internal iliac artery system can be maintained by preserving the communication between the superior and inferior gluteal arteries. In patients with buttock claudication, the demand for oxygen in the gluteal muscles has been reported to increase during exercise, resulting in ischemia and a decrease in rSO2
in the buttocks.10
In this study, intraoperative rSO2
was found to be significantly lower in patients with postoperative buttock claudication than in patients without postoperative buttock claudication. The decrease in rSO2
during EVAR even at rest is thought to be due to the obstruction of blood flow to the external iliac artery caused by the thick sheath of the stent graft and the decrease in blood flow from the deep femoral artery to the internal iliac artery system. Intraoperatively, the decrease in rSO2
meant a decrease in the blood supply capacity of the internal iliac artery network, which was reduced significantly in patients without preserved communication between the superior and inferior gluteal arteries and in patients with buttock claudication. In this study, rSO2, which was decreased at the time of EVAR, was found to recover after sheath removal, and no intestinal or spinal ischemic symptoms were observed. It was reported that buttock claudication occurred in a group with no reserve for acute pelvic ischemia.21
The intraoperative reduction in rSO2
observed in our study may suggest the absence of reserve for ischemia.
Study Limitations
This study has several limitations. First, this is a single-center retrospective study. Second, the number of patients with gluteal claudication was low and not suitable for multivariate analysis. Third, subcutaneous fat thickness may have affected the NIRS signal.
Conclusions
The measurement of rSO2
in the buttocks using NIRS is useful for monitoring blood flow in the internal iliac artery system, and intraoperative reduction of rSO2
may be a predictor of gluteal claudication.
Disclosures
All the authors and co-authors have no conflicts of interest.
IRB Information
This study was approved by Kitasato University Hospital IRB (B18-143).
References
- 1.
Torsello G, Schönefeld E, Osada N, Austermann M, Pennekamp C, Donas KP. Endovascular treatment of common iliac artery aneurysms using the bell-bottom technique: Long-term results. J Endovasc Ther 2010; 17: 504–509.
- 2.
Karthikesalingam A, Hinchliffe RJ, Holt PJE, Boyle JR, Loftus IM, Thompson MM. Endovascular aneurysm repair with preservation of the internal iliac artery using the iliac branch graft device. Eur J Vasc Endovasc Surg 2010; 39: 285–294.
- 3.
Rayt HS, Bown MJ, Lambert KV, Fishwick NG, McCarthy MJ, London NJ, et al. Buttock claudication and erectile dysfunction after internal iliac artery embolization in patients prior to endovascular aortic aneurysm repair. Cardiovasc Interv Radiol 2008; 31: 728–734.
- 4.
Criado FJ, Wilson EP, Velazquez OC, Carpenter JP, Barker C, Wellons E, et al. Safety of coil embolization of the internal iliac artery in endovascular grafting of abdominal aortic aneurysms. J Vasc Surg 2000; 32: 684–688.
- 5.
Kouvelos GN, Katsargyris A, Antoniou GA, Oikonomou K, Verhoeven ELG. Outcome after interruption or preservation of internal iliac artery flow during endovascular repair of abdominal aorto-iliac aneurysms. Eur J Vasc Endovasc Surg 2016; 52: 621–634.
- 6.
Bosanquet DC, Wilcox C, Whitehurst L, Cox A, Williams IM, Twine CP, et al. Systematic review and meta-analysis of the effect of internal iliac artery exclusion for patients undergoing EVAR. Eur J Vasc Endovasc Surg 2017; 53: 534–548.
- 7.
Jones S, Chiesa ST, Chaturvedi N, Hughes AD. Recent developments in near-infrared spectroscopy (NIRS) for the assessment of local skeletal muscle microvascular function and capacity to utilize oxygen. Artery Res 2016; 16: 25–33.
- 8.
Taudorf M, Nielsen MB, Schroeder TV, Lönn L, Nielsen HB. Endovascular aortic repair reduces gluteal oxygenation. Acta Radiol Open 2019; 8: 2058460119850115.
- 9.
Davie SN, Grocott HP. Impact of extracranial contamination on regional cerebral oxygen saturation: A comparison of three cerebral oximetry technologies. Anesthesiology 2012; 116: 834–840.
- 10.
Kishi K, Kawaguchi M, Yoshitani K, Nagahata T, Furuya H. Influence of patient variables and sensor location on regional cerebral oxygen saturation measured by INVOS 4100 near-infrared spectrophotometers. J Neurosurg Anesthesiol 2003; 15: 302–306.
- 11.
Ferrer C, de Crescenzo F, Coscarella C, Cao P. Early experience with the Excluder iliac branch endoprosthesis. J Cardiovasc Surg 2014; 55: 679–683.
- 12.
Van Sterkenburg SMM, Heyligers JMM, Van Bladel M, Verhagen HJ, Eefting D, Van Sambeek MR, et al. Experience with the GORE EXCLUDER iliac branch endoprosthesis for common iliac artery aneurysms. J Vasc Surg 2016; 63: 1451–1457.
- 13.
Itoga NK, Fujimura N, Hayashi K, Obara H, Shimizu H, Lee JT. Outcomes of endovascular repair of aorto-iliac aneurysms and analyses of anatomic suitability for internal iliac artery preserving devices in Japanese patients. Circ J 2017; 81: 682–688.
- 14.
Millon A, Della Schiava N, Arsicot M, De Lambert A, Feugier P, Magne JL, et al. Preliminary experience with the GORE® EXCLUDER® iliac branch endoprosthesis for common iliac aneurysm endovascular treatment. Ann Vasc Surg 2016; 33: 1–7.
- 15.
Etz CD, Kari FA, Mueller CS, Silovitz D, Brenner RM, Lin HM, et al. The collateral network concept: A reassessment of the anatomy of spinal cord perfusion. J Thorac Cardiovasc Surg 2011; 141: 1020–1028.
- 16.
Etz CD, von Aspern K, Gudehus S, Luehr M, Girrbach FF, Ender J, et al. Near-infrared spectroscopy monitoring of the collateral network prior to, during, and after thoracoabdominal aortic repair: A pilot study. Eur J Vasc Endovasc Surg 2013; 46: 651–656.
- 17.
Luehr M, Mohr FW, Etz CD. Indirect neuromonitoring of the spinal cord by near-infrared spectroscopy of the paraspinous thoracic and lumbar muscles in aortic surgery. Thorac Cardiovasc Surg 2016; 64: 333–335.
- 18.
Luehr M, von Aspern K, Etz CD. Limitations of direct regional spinal cord monitoring using near-infrared spectroscopy: Indirect paraspinal collateral network surveillance is the answer! Ann Thorac Surg 2016; 101: 1238–1239.
- 19.
von Aspern K, Haunschild J, Hoyer A, Luehr M, Bakhtiary F, Misfeld M, et al. Non-invasive spinal cord oxygenation monitoring: Validating collateral network near-infrared spectroscopy for thoracoabdominal aortic aneurysm repair. Eur J Cardio Thorac Surg 2016; 50: 675–683.
- 20.
Fujioka S, Hosaka S, Morimura H, Chen K, Wang ZC, Toguchi K, et al. Outcomes of extended endovascular aortic repair for aorto-iliac aneurysm with internal iliac artery occlusion. Ann Vasc Dis 2017; 10: 359–363.
- 21.
Nitta J, Hoshina K, Isaji T. Changes in blood flow distribution after hypogastric artery embolization and the ischaemic tolerance of the pelvic circulation. Medicine (Baltimore) 2019; 98: e14214.