Abstract
Background: Acute aortic dissection (AAD) is a life-threatening cardiovascular disease, with a reported incidence rate ranging from 2.5 to 7.2 per 100,000 person-years in several population-based registries in Western countries, but epidemiological data are lacking in Japan.
Methods and Results: The Shiga Stroke and Heart Attack Registry is an ongoing multicenter population-based registry of cerebro-cardiovascular diseases. We enrolled patients who developed AAD, defined by any imaging examination method from 2014 to 2015 in Shiga Prefecture. Death certificates were used to identify cases that were not registered at acute care hospitals. The incidence rates of AAD were calculated by age categories and adjusted using standard populations for comparison. We evaluated differences in patient characteristics between Stanford type A-AAD and type B-AAD subtypes. A total of 402 incident cases with AAD were analyzed. The age-adjusted incidence rates using the 2015 Japanese population and the 2013 European Standard Population were 15.8 and 12.2 per 100,000 person-years, respectively. Compared with cases of type B-AAD, those with type A-AAD were older (75.0 vs. 69.9 years, P=0.001) and more likely to be women (62.3% vs. 28.6%, P<0.001).
Conclusions: Population-based incidence rates of AAD in Japan appear to be higher than in previous reports from Western countries. Incident cases with type A-AAD were older and female predominance.
Acute aortic dissection (AAD) is a life-threatening cardiovascular disease,1 but as described in guidelines from the USA, Europe, and Japan, epidemiological data for AAD are insufficient and accurate incidence rates have not yet been elucidated.2–4 Given that AAD often rapidly progresses to a lethal condition,5 it is important to calculate the incidence rate by including AAD patients who died outside hospitals and in emergency rooms to evaluate the true incidence.6
Previous population-based registries in Western countries have reported variable incidence rates of AAD, ranging from 2.5 to 7.2 per 100,000 person-years, including cases of out-of-hospital deaths.5,7–10 However, the occurrence of cardiovascular diseases, including AAD, might exhibit regional differences in incidence and mortality rates due to differences in genetic factors, and environmental conditions, including lifestyle or dietary factors by race/ethnicity.11 To date, there have been few population-based studies examining the epidemiological evidence for AAD in Asia. Furthermore, data are scarce regarding the characteristic differences between the types of AAD.
The purpose of the present study was to elucidate the incidence of AAD in Japan on the basis of a large-scale, population-based registry, using out-of-hospital death information in addition to medical record data. We also determined how patients’ characteristics differed by the type of AAD.
Methods
Design of Shiga Stroke and Heart Attack Registry
The Shiga Stroke and Heart Attack Registry (SSHR) is an ongoing multicenter population-based registry study designed to provide a comprehensive information system for the management of cerebrovascular disease, including stroke, acute coronary syndrome, and acute aortic disease in Shiga Prefecture, Japan. Shiga Prefecture is located near the middle of Japan with a population of approximately 1.4 million people. In this registry, for the investigation of acute aortic disease, we have constructed a research system among 15 acute care hospitals in the region (Figure 1). These hospitals included all facilities in which cardiovascular surgery can be performed and almost all hospitals that can receive cardiovascular emergency disease in Shiga Prefecture. According to the guidelines,2–4 patients with AAD are recommended to be treated in a hospital in which cardiovascular surgery can be performed. In this context, the current study covered all such hospitals in Shiga Prefecture, enabling us to collect most cases with AAD in the study area.

In the current study, all cases of patients who developed acute aortic disease were listed on the basis of the International Classification of Diseases (ICD)-10 code I71.0 (Aortic dissection) at each hospital. The ICD-10 code was applied to both deceased patients, and patients admitted at outpatient visit. A trained investigator reviewed the medical records of all listed cases, and selected candidate cases that fitted the definitions of AAD. Data of the candidate cases were consolidated at Shiga University of Medical Science, and ≥2 cardiovascular specialist doctors evaluated the data and made a confirmed diagnosis. With the approval of the Ministry of Health, Labour and Welfare, we used death certificates to identify cases in which patients were diagnosed outside the participating hospitals. The SSHR has been approved by the Institutional Review Board of Shiga University of Medical Science (R2011-86).
Definition of AAD and Its Subtypes
Primary cases of AAD were defined as (1) cases registered from acute care hospitals: cases diagnosed with any imaging examination within 2 weeks of onset of any symptoms such as chest pain or syncope; (2) cases detected only by death certificate: “aortic dissection” listed as the underlying cause of death on the death certificate. Cases of recurrent AAD, defined as the second event and occurring ≥6 months from the first event,8 were considered as one event. AAD was classified into 2 subtypes according to the Stanford classification system:4 type A-AAD involves the ascending aorta, regardless of the site of the primary intimal tear, and all other cases are diagnosed as type B-AAD. In death certificate only (DCO) cases, subtype classification of AAD was not performed because the detailed information required to distinguish them was not available.
Study Population
Figure 2 shows the flow of case enrolment in the study. We registered candidate patients who developed AAD between January 2014 and December 2015 in acute care hospitals. Of the candidate cases, we first excluded those that did not fit the definition of AAD. Duplicate cases, residents of other prefectures, iatrogenic cases, and cases of AAD caused by trauma were also excluded.
We used death certificates in 2014 and 2015 to identify cases that were diagnosed with AAD outside the participating hospitals. First, we extracted cases in which “aortic dissection” was listed as the underlying cause of death on the death certificate. We then excluded patients who developed AAD outside of the study period, and duplicate cases already registered from other acute care hospitals. We defined the remaining cases as DCO cases.
Demographics and Clinical Data
We collected the following information from medical records at the time of hospital admission: age, sex, patient’s condition on arrival at the hospital, past medical history, family medical history, smoking status, blood tests, imaging data, surgical information, and condition at discharge. Hypertension, dyslipidemia, and diabetes mellitus were defined on the basis of the use of respective medications before admission or the description in the medical records. Moreover, as the definition of dyslipidemia, we applied high-density lipoprotein cholesterol level <40 mg/dL and/or low-density lipoprotein cholesterol level ≥140 mg/dL. Because all blood samples were not taken only during fasting, triglyceride levels were not included in the criteria. Additionally, glycated hemoglobin (HbA1c) ≥6.5% was applied for diabetes mellitus.
Statistical Analysis
Continuous variables are presented as means with standard deviation, and categorical variables are presented as numbers and proportions. Group differences in continuous variables were examined with Student’s t-test and categorical variables were examined with Fisher’s exact test or χ2
test, as appropriate. To examine age-specific trends, we divided cases into 7 age categories (<35, 35–44, 45–55, 55–64, 65–74, 75–84, ≥85 years). The incidence rates of AAD were described by the person-year approach (per 100,000 person-years) using the populations in Shiga Prefecture in 2014 and 2015, and were standardized for age using a direct method with the 2015 Japanese population. Furthermore, to compare the results with reports from Western countries, incidence rates were standardized for age using a direct method with the 2013 European Standard Population. Differences with a two-tailed P value <0.05 were considered to be statistically significant. Analyses were performed using SAS software version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Incidence Rate of AAD
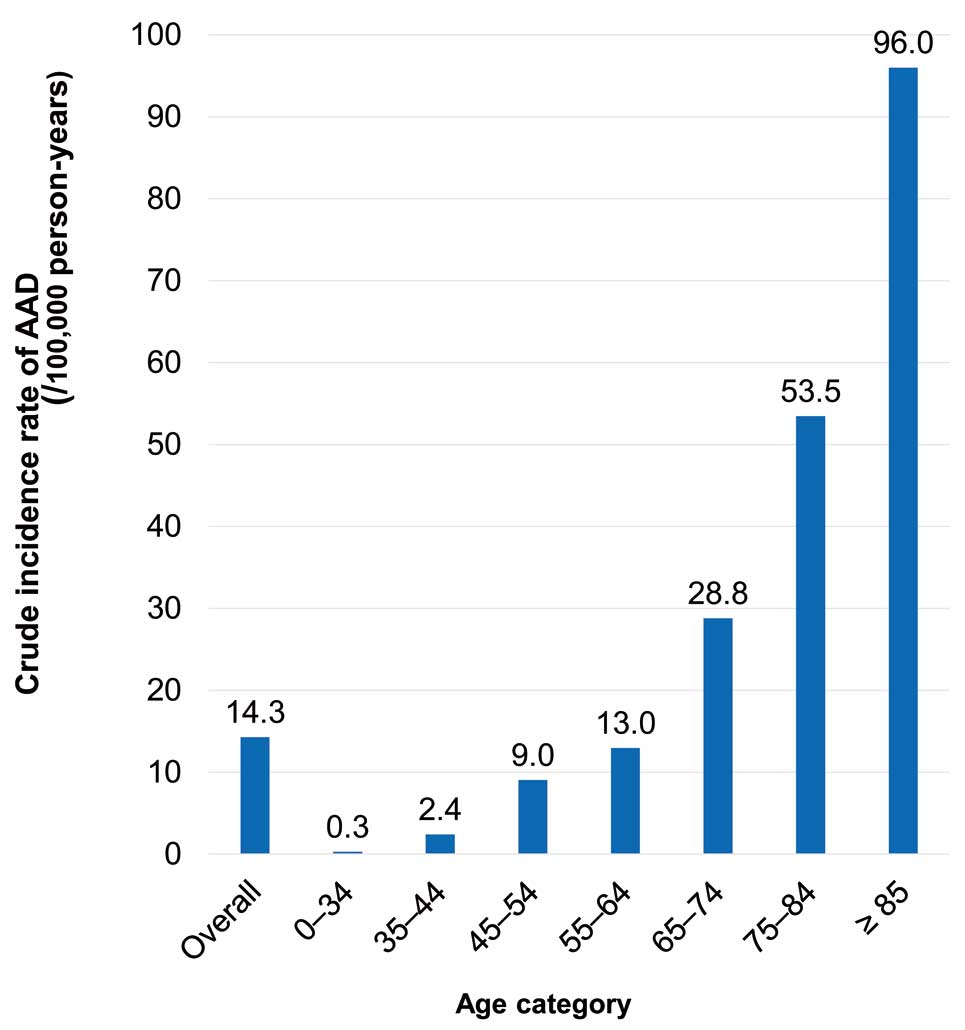
Of 422 candidate cases for AAD from acute care hospitals, 374 were enrolled. In addition, of 165 candidate cases for AAD from death certificates, 28 were enrolled. Finally, 402 cases were analyzed in this study (Figure 2). The mean age was 73.2 years and the proportion of women was 49.5% (Table 1). The crude incidence rate of AAD in Shiga Prefecture was 14.3 per 100,000 person-years. The incidence rate of AAD increased with age, and was highest among those aged ≥85 years, with an incidence of 96.0 per 100,000 person-years (Figure 3). The age-adjusted incidence rates of AAD using the 2015 Japanese population and the 2013 European Standard Population were 15.8 and 12.2 per 100,000 person-years, respectively. In the analysis of cases with an identified subtype, age-adjusted incidence rates in patients with type A-AAD using the 2015 Japanese population and the 2013 European Standard Population were 8.6 and 6.6 per 100,000 person-years, respectively, and those in patients with type B-AAD were 6.0 and 4.8 per 100,000 person-years, respectively.
Table 1. Demographics of AAD
| |
Overall [n=402] |
| Age, years |
73.2±14.8 |
| Women, n (%) |
199 (49.5) |
| Subtype of AAD |
| A-AAD, n (%) |
220 (54.7) |
| B-AAD, n (%) |
154 (38.3) |
| DCO, n (%) |
28 (7.0) |
Data are presented as number (%), mean and standard deviation. AAD, acute aortic dissection; DCO, death certificate only.
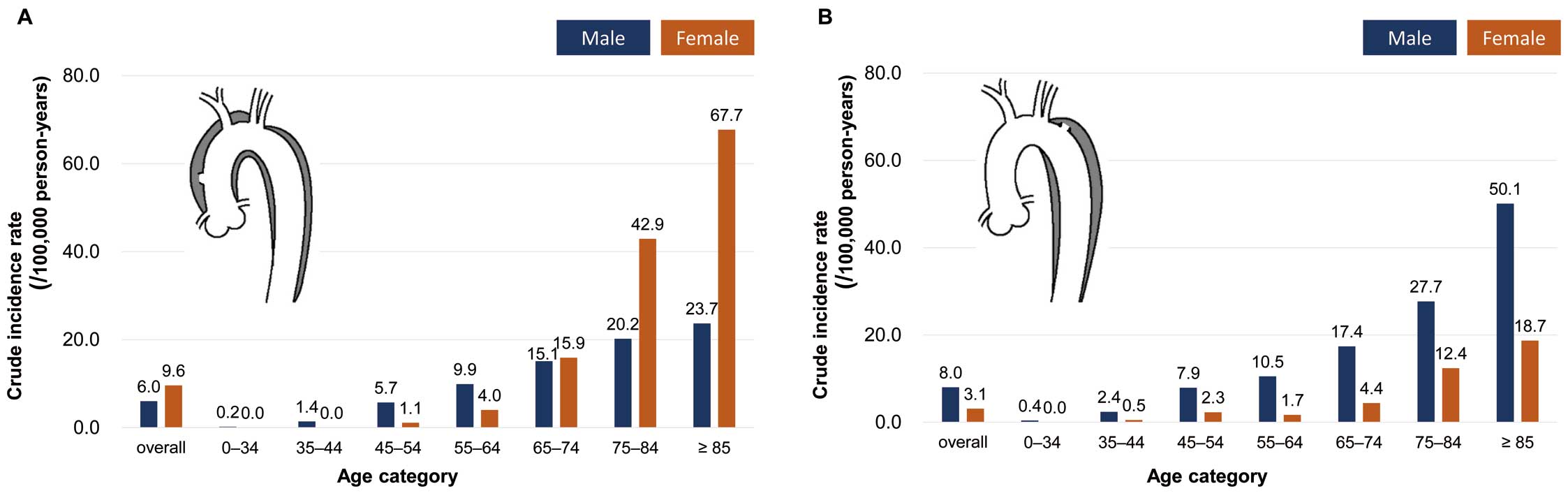
Age- and sex-specific incidence rates for each subtype are shown in Figure 4. The crude incidence rates of type A-AAD in men and women were 6.0 and 9.6, respectively. Although the incidence rates of type A-AAD were higher in men under the age of 65 years, incidence rates of type A-AAD in women increased exponentially over the age of 65 and surpassed those in men. The incidence rates of type B-AAD in men and women were 8.0 and 3.1, respectively. Unlike the trend in type A-AAD patients, men’s predominance of type B-AAD was observed in all age categories.
Differences Between Subtypes of AAD
Table 2 summarizes the differences in baseline characteristics between incident cases of type A-AAD and type B-AAD. Compared with cases of type B-AAD, patients with type A-AAD were significantly older (75.0 vs. 69.9 years, P=0.001), more likely to be female (62.3% vs. 28.6%, P<0.001), less likely to have dyslipidemia (32.2% vs. 46.1, P=0.008), and more likely to be current smokers (17.7% vs. 37.8%, P<0.001). The percentage of patients who died in the emergency room was significantly higher for type A-AAD than for type B-AAD (36.1% vs. 5.2%, P<0.001). In contrast, the proportions of hypertension, Marfan syndrome, and history of AAD were not significantly different between the 2 subtypes.
Table 2. Comparison of Patients’ Baseline Characteristics Between Subtypes A-AAD and B-AAD
| |
Type A-AAD
[n=220] |
Type B-AAD
[n=154] |
P value |
| Age, years |
75.0±12.8 |
69.9±15.0 |
0.001 |
| Women, n (%) |
137 (62.3) |
44 (28.6) |
<0.001 |
| BMI, kg/m2 |
23.1±4.7 [n=143] |
23.4±4.8 [n=131] |
0.505 |
| Height, cm |
156.6±10.9 [n=148] |
162.1±9.8 [n=135] |
<0.001 |
| Weight, kg |
57.5±17.8 [n=148] |
62.2±16.8 [n=137] |
0.022 |
| Hypertension, n (%) |
124/202 (61.4) |
104/152 (68.4) |
0.171 |
| Diabetes mellitus, n (%) |
48/200 (24.0) |
25/152 (16.5) |
0.083 |
| Dyslipidemia, n (%) |
65/202 (32.2) |
70/152 (46.1) |
0.008 |
| Current smoker |
25/141 (17.7) |
54/143 (37.8) |
<0.001 |
| Marfan syndrome, n (%)* |
– |
– |
0.847 |
| Previous disease, n (%) |
| Previous AAD* |
– |
– |
0.957 |
| Any cardiac operation* |
– |
– |
0.944 |
| MI* |
– |
– |
0.738 |
| Heart failure* |
10/199 (5.0) |
– |
0.261 |
| COPD* |
7/200 (3.5) |
– |
0.393 |
| Hemodialysis* |
– |
9/152 (5.9) |
0.630 |
| CI |
19/200 (9.5) |
– |
0.219 |
| ICB* |
8/199 (4.0) |
– |
0.720 |
| Death in ER, n (%) |
81 (36.1) |
8 (5.2) |
<0.001 |
Data are presented as the number (%), mean and standard deviations. The P values were calculated between patients with type A-AAD and those with type B-AAD. *Actual number <5. AAD, acute aortic dissection; CI, cerebral infarction; COPD, chronic obstructive pulmonary disease; ER, emergency room; ICB, intracerebral hemorrhage; TEVAR, thoracic endovascular aortic repair.
Discussion
Principal Findings
Our results revealed 2 main findings. First, the age-adjusted incidence rate of AAD using the 2015 Japanese population was 15.8 per 100,000 person-years. Second, the characteristics of incident cases of type A-AAD and type B-AAD were significantly different. Female predominance among those ≥65 years old was observed, particularly for type A-AAD.
Findings in the Context of Current Literature
Incidence Rate of AAD Several population-based studies have reported incidence rates of AAD. As shown in Figure 5, the Oxford Vascular Study, which is the only prospective study in the UK, reported the incidence of acute thoracic aortic dissection as 6.0 per 100,000 person-years.8 A retrospective nationwide population registry in Sweden reported an incidence of aortic dissection of 7.2 per 100,000 person-years.7 Those studies included information on out-of-hospital deaths, such as autopsy, which may provide a more accurate incidence rate. Japan has one of the oldest national populations in the world, resulting in a tendency for higher age-adjusted incidence rates when using the Japanese population as the standard. Therefore, we also evaluated the age-adjusted incidence rates using the 2013 European Standard Population to compare the results with reports from Western countries. In the current study, when adjusting by the 2013 European Standard Population, the age-adjusted incidence rate of AAD was 12.2 per 100,000 person-years, which was still substantially higher than in previous reports from Western countries. In a previous population-based study in Japan, the age-adjusted incidence rate of AAD was 17.6 per 100,000 person-years,12 indicating a higher rate than that found in the current study. Although the previous report included only patients who were admitted to a single facility in a geographically limited rural area with a small population (120,000 inhabitants), the incidence rate of AAD in Japan may be higher than in Western countries.

The reason for the higher incidence rate of AAD in Japan compared with Western countries is currently unclear. One possible reason is that the prevalence of hypertension in Japan is higher than that in most Western countries.13 In addition, compared with Western countries, improvement in awareness, treatment, and control of hypertension has not reached a satisfactory level in Japan.14 A meta-analysis of 2 large cohorts reported that hypertension is associated with an increased risk of aortic dissection.15 The prevalence of uncontrolled hypertension in Japan might contribute to the high incidence rate of AAD.
Another possible reason is related to the high penetration rate of computed tomography (CT) and the frequent use of CT imaging in Japan. The number of CT machines per million inhabitants was 116 in Japan in 2020, which was approximately 4-fold higher than that reported in Organization for Economic Co-operation and Development countries.16 Frequent use of CT in the emergency department may be related to higher detection rates of AAD.17 Indeed, 97.3% of cases in our study were diagnosed by CT, including autopsy imaging.
However, the occurrence of cardiovascular disease is certainly associated with genetic factors, lifestyle, dietary factors, environmental conditions, and coexisting diseases.11 Therefore, further studies are needed to clarify the underlying reasons for the higher incidence rate of AAD in Japan.
Differences Between Subtypes of AAD The mean age of the incident cases enrolled in the current study was higher than that in other population-based studies conducted in Western countries, in which mean ages ranged from 66 to 72 years.5,7,8,10 In previous studies conducted in Western countries, few differences were reported in the characteristics of cases of type A-AAD and type B-AAD,5,8,18 whereas our findings revealed marked differences between subtypes in age, sex distribution, the proportion of patients with dyslipidemia, and the proportion of current smokers. In the current study, the mean age of patients with type A-AAD was 5 years older than those with type B-AAD. The proportion of women with the type A-AAD subtype was more than twice as high as that among cases of type B-AAD. The International Registry of Acute Aortic Dissection (IRAD), an observational registry involving highly specialized aortic centers around the world, reported that the sex distribution of AAD in both types exhibited a 2 : 1 male:female ratio.18 Recent population-based registries also reported a male predominance in both subtypes.19 However, 2 previous reports from Japan indicated that the proportion of women was higher among patients with type A-AAD compared with those with type B-AAD.17,20 Goda et al surveyed the differences in the characteristics of patients with type A-AAD between Belgian and Japanese centers, and reported that Japanese women were more likely to develop type A-AAD than Belgian women.11 Indeed, our study showed that for type B-AAD, men exhibited higher incidence rates than women in all age groups, whereas for type A-AAD, women over 65 years of age had higher incidence rates than men in the same age group.
Although the clear reason for the higher proportion of women with type A-AAD in our study remains unknown, there are several potential explanations. The first is that the IRAD study reported women with type A-AAD were likely to present atypical initial symptoms such as coma or congestive heart failure,21 which could lead to underestimation of the type A-AAD incidence in women. However, as mentioned above, Japan has the highest penetration rate of CT among OECD countries, and high level of use of CT could contribute to uncovering type A-AAD patients with atypical presentation. The second potential explanation is that Japan has attained the world’s longest life expectancy and healthy life expectancy in women,22 and in the reports on sex differences in patients with type A-AAD, women are older than men at the time of diagnosis.18,23 These facts could have led to the enrolment of a large number of older women with type A-AAD in our study. Indeed, our study showed an exponential increase in the incidence of type A-AAD in women with age. Moreover, the proportion of women was higher than among the deceased patients without concomitant hospital stay.7 Given that our study consisted of relatively older patients than in other studies, including death in the emergency room, it may be reasonable for there to be a higher proportion of women with type A-AAD in our study.
Another possible explanation for the differences in the characteristics between type A-AAD and type B-AAD is the biological mechanisms of AAD, 2 of which have been suggested to contribute to the development of aortic dissection.15 The first mechanism is the loss of elastic fibers in the aortic media and unstable connections between the elastic lamina, which is commonly seen in type A-AAD. Another mechanism that may contribute to the development of AAD is atherosclerosis, which is commonly seen in patients with type B-AAD. One can hypothesize that Japanese women may have more pronounced vessel wall fragility,11 which could explain why Japanese women are more likely to develop type A-AAD. The biological mechanism underlying atherosclerosis is commonly seen in patients with type B-AAD, which may also explain the proportion of men, as shown in this study, as well as the incidence of dyslipidemia, and the proportion of current smokers was higher among the patients with type B-AAD compared with those with type A-AAD. Especially, compared with Western countries, the prevalence of current tobacco use by men is markedly higher than by women in Japan,24 which might have led to the male predominance in cases of type B-AAD.
Study Limitations
This study involved several potential limitations. First, we had no information regarding people with AAD who did not visit a doctor, or those who were diagnosed at non-participating hospitals or clinics. Additionally, we had no information about AAD cases admitted to hospitals outside of Shiga Prefecture (e.g., developed AAD while staying in another prefecture). However, as for the patients who developed AAD in Shiga Prefecture, the rate of patients who were transported outside of the city in Otsu City, which is on the border with Kyoto Prefecture, has been reported to be much lower than in other regions in Japan.25 Second, it is possible that some deceased cases in the community were misdiagnosed. In our study, cases of out-of-hospital or prehospital death were included if they had been diagnosed with AAD by adequate examination such as autopsy or autopsy imaging. However, autopsy rates for individuals who die without an obvious cause of death are lower in Japan compared with many other countries.26 Therefore, there may have been some missed cases of out-of-hospital or prehospital death caused by AAD. However, because both of these limitations would cause an underestimation of the incidence of AAD, they do not explain the high incidence of AAD in Japan observed in the current study. Third, the incidence rate of AAD by its subtype may be underestimated because it did not include DCO cases. Finally, we did not evaluate the accuracy of the diagnosis of DCO cases. However, it is assumed that there is typically some reasonable basis for listing “aortic dissection” as the underlying cause of death on the death certificate. Hence, we consider that it is valid to include DCO cases to calculate the incidence rate of AAD.
Conclusions
The current analysis of a Japanese population-based registry of AAD in a real-world setting clarified the incidence rates of AAD. Compared with previous reports in Western countries, the incidence rate of AAD was higher in Japan, and a female predominance of AAD was identified in older patients with the A-AAD subtype. Further studies are warranted to clarify the underlying reasons for the epidemiological differences in AAD between Japan and other countries.
Acknowledgments
We thank Benjamin Knight, MSc, from Edanz (https://jp.edanz.com/ac) for editing a draft of this manuscript.
SSHR is supported by Shiga Prefecture and the Japan Agency for Medical Research and Development (Grant No. 17ek0210090).
Disclosures
The authors declare no conflicts of interest associated with this manuscript.
IRB Information
Institutional Review Board of Shiga University of Medical Science (R2011-86).
Data Availability
Research data are not publicly available on ethical grounds.
References
- 1.
Mussa FF, Horton JD, Moridzadeh R, Nicholson J, Trimarchi S, Eagle KA. Acute aortic dissection and intramural hematoma. JAMA 2016; 316: 754, doi:10.1001/jama.2016.10026.
- 2.
Erbel R, Aboyans V, Boileau C, Bossone E, Bartolomeo RD, Eggebrecht H, et al. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur Heart J 2014; 35: 2873–2926, doi:10.1093/eurheartj/ehu281.
- 3.
JCS Joint Working Group. Guidelines for diagnosis and treatment of aortic aneurysm and aortic dissection (JCS 2011): Digest version. Circ J 2013; 77: 789–828, doi:10.1253/circj.CJ-66-0057.
- 4.
Hiratzka LF, Bakris GL, Beckman JA, Bersin RM, Carr VF, Casey DE Jr, et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with Thoracic Aortic Disease: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. Circulation 2010; 121: e266–e369, doi:10.1161/CIR.0b013e3181d4739e.
- 5.
Melvinsdottir IH, Lund SH, Agnarsson BA, Sigvaldason K, Gudbjartsson T, Geirsson A. The incidence and mortality of acute thoracic aortic dissection: Results from a whole nation study. Eur J Cardiothorac Surg 2016; 50: 1111–1117, doi:10.1093/ejcts/ezw235.
- 6.
Takeuchi S, Yamaguchi Y, Soejima K, Yoshino H. Incidence and characteristics of acute aortic dissection in patients with out-of-hospital cardiopulmonary arrest evaluated by non-contrast computed tomography. Eur Heart J Acute Cardiovasc Care 2020; 9: S48–S57, doi:10.1177/2048872620923647.
- 7.
Smedberg C, Steuer J, Leander K, Hultgren R. Sex differences and temporal trends in aortic dissection: A population-based study of incidence, treatment strategies, and outcome in Swedish patients during 15 years. Eur Heart J 2020; 41: 2430–2438, doi:10.1093/eurheartj/ehaa446.
- 8.
Howard DP, Banerjee A, Fairhead JF, Perkins J, Silver LE, Rothwell PM, et al. Population-based study of incidence and outcome of acute aortic dissection and premorbid risk factor control: 10-year results from the Oxford Vascular Study. Circulation 2013; 127: 2031–2037, doi:10.1161/CIRCULATIONAHA.112.000483.
- 9.
Obel LM, Lindholt JS, Lasota AN, Jensen HK, Benhassen LL, Mørkved AL, et al. Clinical characteristics, incidences, and mortality rates for type A and B aortic dissections: A nationwide Danish population-based cohort study from 1996 to 2016. Circulation 2022, doi:10.1161/circulationaha.122.061065.
- 10.
McClure RS, Brogly SB, Lajkosz K, Payne D, Hall SF, Johnson AP. Epidemiology and management of thoracic aortic dissections and thoracic aortic aneurysms in Ontario, Canada: A population-based study. J Thorac Cardiovasc Surg 2018; 155: 2254–2264.e4, doi:10.1016/j.jtcvs.2017.11.105.
- 11.
Goda M, Minami T, Imoto K, Uchida K, Masuda M, Meuris B. Differences of patients’ characteristics in acute type A aortic dissection: Surgical data from Belgian and Japanese centers. J Cardiothorac Surg 2018; 13: 92, doi:10.1186/s13019-018-0782-x.
- 12.
Yamaguchi T, Nakai M, Yano T, Matsuyama M, Yoshino H, Miyamoto Y, et al. Population-based incidence and outcomes of acute aortic dissection in Japan. Eur Heart J Acute Cardiovasc Care 2021; 10: 701–709, doi:10.1093/ehjacc/zuab031.
- 13.
Zhou B, Danaei G, Stevens GA, Bixby H, Taddei C, Carrillo-Larco RM, et al. Long-term and recent trends in hypertension awareness, treatment, and control in 12 high-income countries: An analysis of 123 nationally representative surveys. Lancet 2019; 394: 639–651, doi:10.1016/s0140-6736(19)31145-6.
- 14.
Hisamatsu T, Miura K. Epidemiology and control of hypertension in Japan: A comparison with Western countries. J Hum Hypertens 2021, doi:10.1038/s41371-021-00534-3.
- 15.
Hibino M, Otaki Y, Kobeissi E, Pan H, Hibino H, Taddese H, et al. Blood pressure, hypertension, and the risk of aortic dissection incidence and mortality: Results from the J-SCH Study, the UK Biobank Study, and a meta-analysis of cohort studies. Circulation 2022; 145: 633–644, doi:10.1161/circulationaha.121.056546.
- 16.
OECD. Health at a glance 2021: OECD indicators. https://data.oecd.org/healtheqt/computed-tomography-ct-scanners.htm (accessed October 21, 2022).
- 17.
Yamaguchi T, Nakai M, Sumita Y, Miyamoto Y, Matsuda H, Inoue Y, et al. Current status of the management and outcomes of acute aortic dissection in Japan: Analyses of nationwide Japanese Registry of All Cardiac and Vascular Diseases-Diagnostic Procedure Combination data. Eur Heart J Acute Cardiovasc Care 2020; 9: S21–S31, doi:10.1177/2048872619872847.
- 18.
Evangelista A, Isselbacher EM, Bossone E, Gleason TG, Eusanio MD, Sechtem U, et al. Insights from the International Registry of Acute Aortic Dissection. Circulation 2018; 137: 1846–1860, doi:10.1161/circulationaha.117.031264.
- 19.
Bossone E, Carbone A, Eagle KA. Gender differences in acute aortic dissection. J Pers Med 2022; 12: 1148, doi:10.3390/jpm12071148.
- 20.
Sadamatsu K, Sagara S, Oe K, Tashiro H, Yasunaga H. Meteorological and chronobiological factors and the occurrence of acute aortic dissection. Heart Vessels 2020; 35: 1003–1011, doi:10.1007/s00380-020-01569-1.
- 21.
Nienaber CA, Fattori R, Mehta RH, Richartz BM, Evangelista A, Petzsch M, et al. Gender-related differences in acute aortic dissection. Circulation 2004; 109: 3014–3021, doi:10.1161/01.cir.0000130644.78677.2c.
- 22.
Tokudome S, Hashimoto S, Igata A. Life expectancy and healthy life expectancy of Japan: The fastest graying society in the world. BMC Res Notes 2016; 9: 482, doi:10.1186/s13104-016-2281-2.
- 23.
Rylski B, Georgieva N, Beyersdorf F, Büsch C, Boening A, Haunschild J, et al. Gender-related differences in patients with acute aortic dissection type A. J Thorac Cardiovasc Surg 2021; 162: 528–535.e1, doi:10.1016/j.jtcvs.2019.11.039.
- 24.
WHO. The global health observatory. https://www.who.int/data/gho/data/themes/topics/sdg-target-3_a-tobacco-control (accessed February 21, 2023).
- 25.
Takashima N, Arima H, Kita Y, Fujii T, Miyamatsu N, Komori M, et al. Incidence, management and short-term outcome of stroke in a general population of 1.4 million Japanese: Shiga Stroke Registry. Circ J 2017; 81: 1636–1646, doi:10.1253/circj.CJ-17-0177.
- 26.
Urabe S, Ishihara K, Chiba F, Yamaguchi R, Shiko Y, Kawasaki Y, et al. Children’s death survey using death certificates in the Chiba prefecture. Forensic Sci Int Rep 2021; 4: 100246, doi:10.1016/j.fsir.2021.100246.