An 80-year-old man with progressive exertional dyspnea visited hospital on suspicion of heart failure with preserved ejection fraction (HFpEF). Echocardiography showed mild mitral regurgitation and normal systolic but abnormal diastolic function with prolonged deceleration time (289 s) and elevated E/e‘ (23.4). Bicycle-ergometer exercise test up to 5.2 Mets induced severe dyspnea and arterial oxygen desaturation from 97% to 88% without ischemic changes. Pulmonary function tests showed decreased lung diffusing capacity (DLCO/VA, 63.5%) without restrictive or obstructive defects.
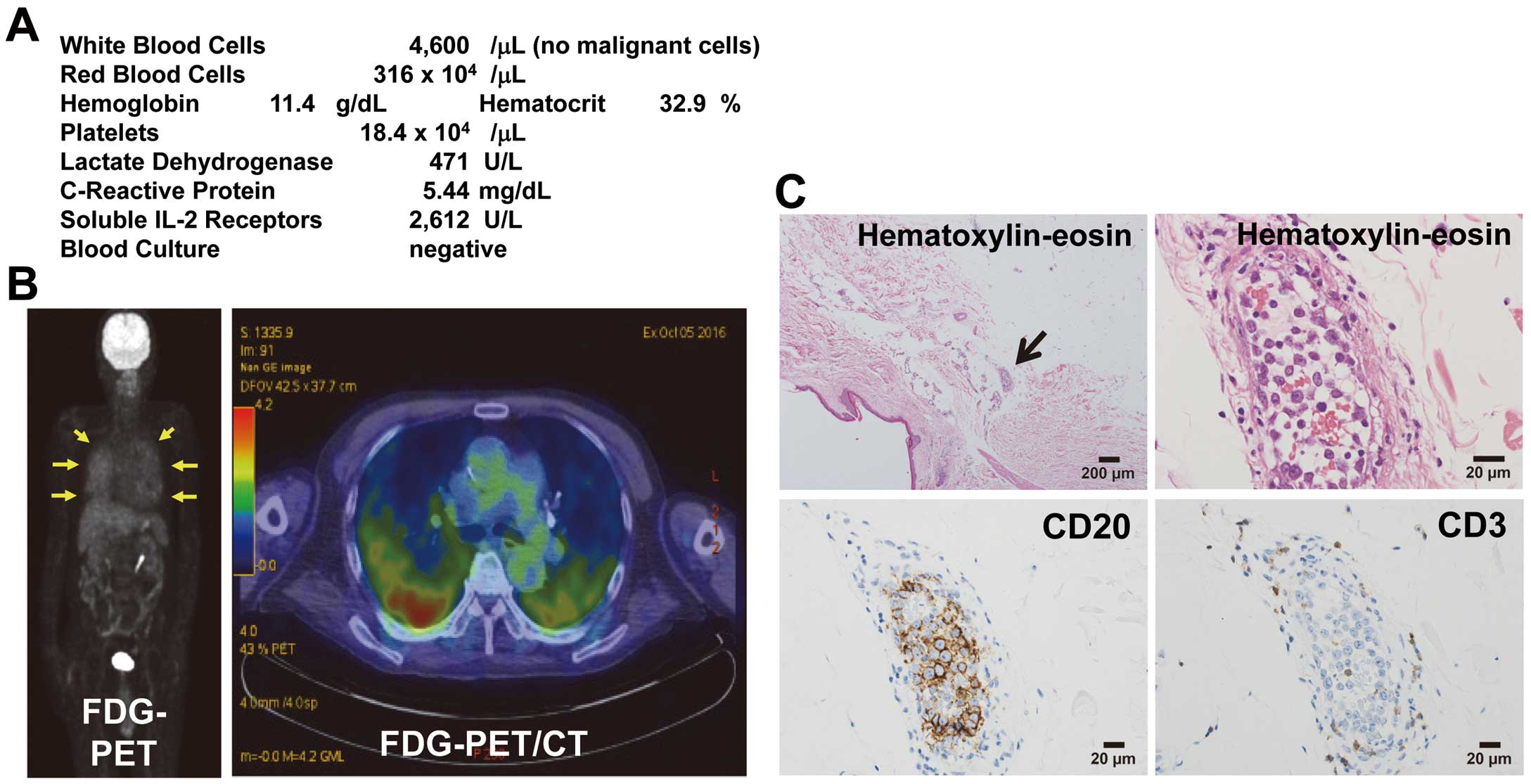
After admission, fever in the 37℃ range and body weight loss (−2 kg in 3 weeks) continued without lymphadenopathy, cutaneous lesions, or neurological abnormality. Soluble interleukin-2 receptors and lactate dehydrogenase increased (Figure). Fluorodeoxyglucose (FDG) positron emission tomography/computed tomography showed FDG uptake in the lungs but not in other organs or lymph nodes. He was diagnosed with intravascular large B-cell lymphoma (IVLBCL) on random skin biopsy showing exclusive growth of large CD20+/CD3−
neoplastic lymphocytes in small vessel lumina in the dermis. R-CHOP therapy produced complete remission for 2 years without recurrent dyspnea. Kurume University Medical Center Ethics Committee waived ethics approval.
IVLBCL typically occurs in the elderly (median age, 70 years) and shows rapid progression of non-specific lymphoma symptoms and various organ disorders (especially neurological and cutaneous abnormalities) with poor prognosis, lacking lymphadenopathy.1
Random skin biopsy is indispensable for diagnosing IVLBCL even if cutaneous lesions are absent. Progressive exertional dyspnea with reduced DLCO/VA and lung FDG uptake suggests lung involvement in IVLBCL, which can cause hypoxia with decreased diffusing capacity.1
Accordingly, IVLBCL can be a differential diagnosis of exertional dyspnea mimicking HFpEF.
Disclosures
The authors declare no conflicts of interest.
