Abstract:
Industrial talc has been widely circulated in the world for a long time. The pure talc
has little effects on humans, but inhalation of talc contaminated with asbestos can causes
severe asbestos-related diseases such as lung cancer and malignant mesothelioma. Herein,
we represent a case of lung cancer after occupational exposure to industrial talc in the
rubber manufacturing industry.
Introduction
Talc is a hydrated magnesium silicate that has been widely used in the chemical, ceramic,
cosmetic, leather, paper, and building industries. Industrial talc can contain asbestos or
quartz particles1), which have
the potential to induce asbestos-related diseases, including malignancies, or silicosis.
Herein we report a case of lung cancer after occupational exposure to talc in the rubber
manufacturing industry.
Case Report
An 85 yr-old man presented to the Department of Internal Medicine of Kosin Medical Center
with a three-month history of shortness of breath, cough, and bloody sputum. He had a
history of tuberculosis 20 yr prior to presentation. He had worked in handicraft
manufacturing for 20 yr until his retirement at his age of 60. Before starting this work he
was a farmer since he was 20 yr old. He was self-employed for 20 yr at approximately
10m2 sized workplace in which there was no ventilation system (closed system).
The workplace was dusty in the air and floor and no protection equipment was used at that
time. The patient’s main task was to blow up the talc stained balloons through his mouth
without the support of the air pumping equipment for 10 h per day. At that time he received
no information about asbestos contamination, and he inhaled talc from the balloons. His
smoking history was 30 pack-years. Physical and clinical examination at the local medical
center revealed a cavitary lung lesion that was highly suspicious for cancer; therefore, he
wanted to get a second opinion regarding whether the diagnosis was lung cancer or
tuberculosis. On examination, his temperature was 37.8°, heart rate was 80 beats per minute,
blood pressure was 98/60 mmHg, and oxygen saturation was 95%. The left lung sounds were
decreased on auscultation and radiography revealed a cavitary lung mass in the left lower
lobe (Fig. 1A). Several calcified opacities were
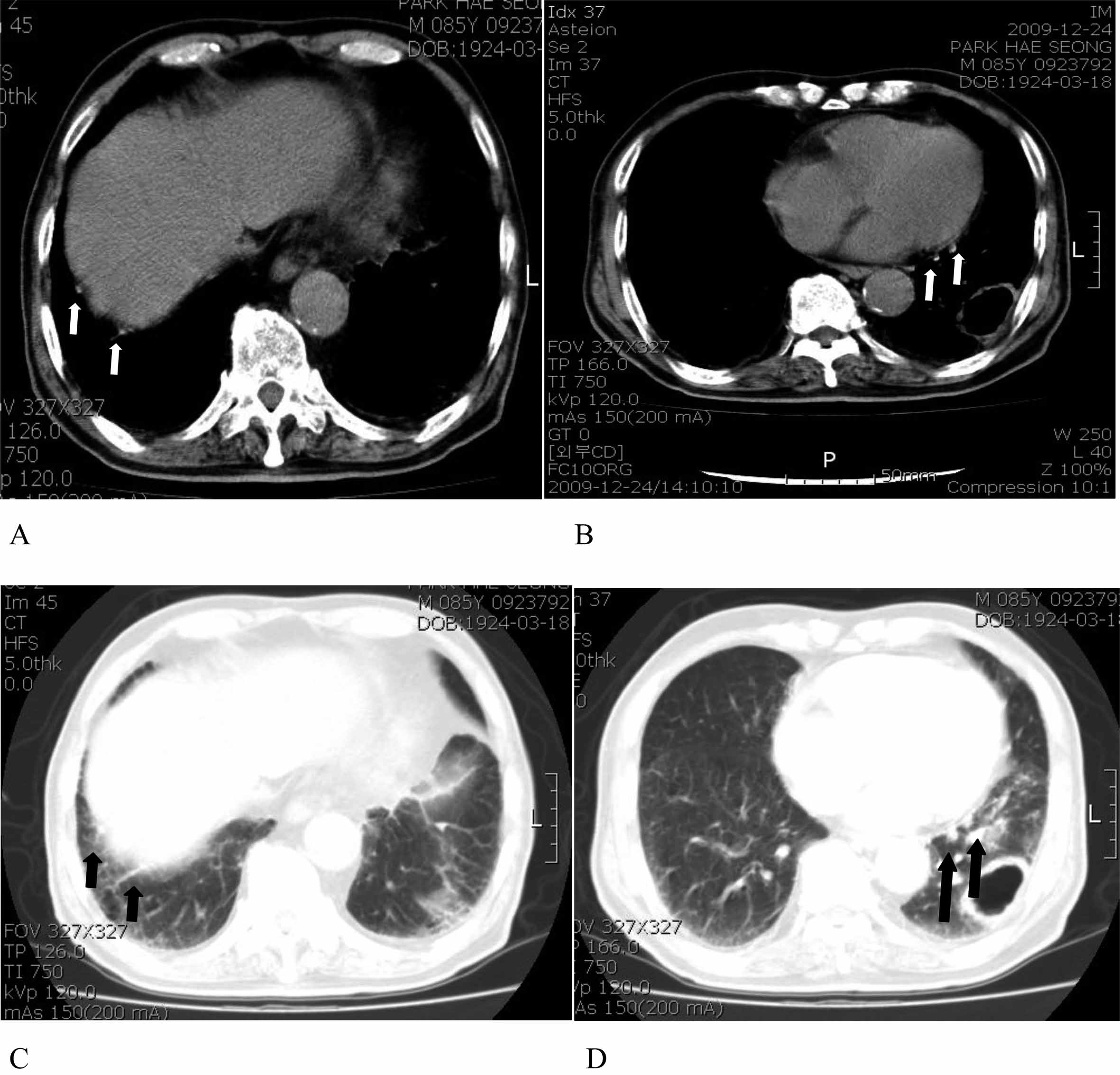
also visualized around tumor on computed tomography (CT) (Figs. 1B, 1C, 1D, 1E and 1F). We could not detect the findings of pneumoconiosis, asbestosis, or talcosis.
Moreover, multiple calcified plaques along the diaphragmatic pleura in the right lower lung
and mediastinal pleura in the left lower lung were seen on chest CT (Figs. 2A, 2B, 2C and 2D).
A complete blood count with differential counts and the results of serum chemical tests,
including tests of liver function and renal function, were within normal limits. Fiberoptic
bronchoscopy was performed under conscious anesthesia. Bronchoscopy revealed several
anthracotic plaques and a nodular mass in the left lower bronchus. The pathologic diagnosis
from the bronchoscopic biopsy was squamous cell carcinoma. The clinical stage was assessed
as stage IIIa, but the patient refused curative treatment and wanted best supportive care.
He died due to pneumonia four months after the first diagnosis. The publication of this case
was conducted with the approval of the Kosin University Gospel Hospital Ethics
Committee.

Discussion
Diseases related to talc exposure can be divided into four main categories: talco-silicosis
due to inhalation of talc associated with free silica; talco-asbestosis due to inhalation of
talc contaminated with asbestos; pure talcosis due to inhalation of talc in the absence of
other minerals; and pulmonary disease secondary to the use of injected talc among
intravenous drug users2).
The term talc is applied to a heterogeneous group of hydrated magnesium silicates that are
commonly found in mineral deposits containing varying quantities of other minerals including
carbonates, quartz, amphiboles, and serpentines3). Occupational exposure can occur during the mining, milling,
packaging, and distribution of talc and in secondary industries, such as ceramics and
rubber, and from contact with the final product (cosmetic talc)4). Therefore, the talc likely contained asbestos. The
pure form of talc has relatively fewer health effects on humans, but talc contaminated with
asbestos, especially asbestos particulates that are longer than 5 µm with a length-to-width
ratio of 3:1 or more, causes severe health problems5). Inhalation of asbestos can result in chronic inflammatory
pulmonary response. In the worst cases, asbestos inhalation can result in malignant
neoplasms, such as mesothelioma and lung cancer, which generally occur some 20–40 yr after
the onset of asbestos exposure; however, asbestosis can appear in 8–25 yr6).
The recent report by Kim described an issue of talc contaminated by asbestos in Korea that
the Korea Food and Drug Administration found that 11 talc powders for babies contained
asbestos plus with 1,120 drugs and medical goods have been confirmed to contain talc
contaminated with asbestos which resulted in a ban of circulation of more than 1%
asbestos-containing industrial talc in 2010 which meant the industrial talc contaminated
with asbestos had been used without government regulation for a long time7). In the present case, the talc was
used in balloons to keep the latex from sticking to itself8). The length of exposure to talc in this case was
20 yr, which was a relatively long time for respiratory symptoms, radiological
abnormalities, and diminished pulmonary function to develop due to exposure to mineral dust.
In this case, the isolated finding of multiple diaphragmatic and mediastinal pleural plaques
in both side lower lung is likely associated with past exposure to asbestos fibers, which
are present in industrial talc. Pleural plaques are the most common asbestos-related
disease8), and their
prevalence grows with increasing latency period. Twenty years after the initial exposure,
around 10% of exposed individuals will develop plaques9).
With regard to smoking, the mean pack-year index was 30, which was considered relatively
high. There are reports in the literature regarding synergistic effects between smoking and
lung cancer, especially among workers exposed to asbestos10). Without the occupational history of asbestos
exposure in this case, most clinicians would suggest the patient’s lung cancer was caused by
smoking. However, primary physicians and consultants should consider the possibility of
asbestos exposure as another potential cause of lung cancer.
References
- 1) Paoletti L, Caiazza S, Donelli G, Pocchiari F (1984) Evaluation by electron
microscopy techniques of asbestos contamination in industrial, cosmetic, and
pharmaceutical talcs. Regul Toxicol Pharmacol 4, 222–35.
- 2) Feigin DS (1986) Talc: Understanding its manifestations in the chest. AJR Am
J Roentgenol 146, 295–301.
- 3) Gamble JF, Fellner W, Dimeo MJ (1979) An epidemiologic study of a group of a
talc workers. Am Rev Respir Dis 119, 741–53.
- 4) Gibbs AE, Pooley FD, Griffiths DM, Mitha R, Craighead JE, Ruttner JR (1992)
Talc pneumoconiosis: a pathologic and mineralogic study. Hum Pathol 23,
1344–54.
- 5) Gamble JF, Gibbs GW (2008) An evaluation of the risks of lung cancer and
mesothelioma from exposure to amphibole cleavage fragments. Regul Toxicol Pharmacol 52,
S154–86.
- 6) Wylie AG, Skinner HC, Marsh J, Snyder H, Garzione C, Hodkinson D, Winters R,
Mossman BT (1997) Mineralogical features associated with cytotoxic and proliferative
effects of fibrous talc and asbestos on rodent tracheal epithelial and pleural mesothelial
cells. Toxicol Appl Pharmacol 147, 143–50.
- 7) Kim HR (2009) Overview of asbestos issues in Korea. J Korean Med Sci 24,
363–7.
- 8) Landgraf KF (1988) Evidence of mineral impurities in Talc. Pharmazie 43,
20–3.
- 9) Gevenois PA, Maertelaer V, Madani A, Winant C, Sergent G, De Vuyst P (1998)
Asbestosis, pleural plaques and diffuse pleural thickening: three distinct benign
responses to asbestos exposure. Eur Respir J 11, 1021–7.
- 10) Kamp DW (2009) Asbestos-induced lung diseases: an update. Transl Res 153,
143–52.