Abstract
Adrenal epithelioidangiosarcoma (AEA) is a rare neoplasm that accounts for less than 1%
of sarcomas. Due to its rarity, it can easily be misdiagnosed, both by the clinician and
the pathologist. Data on the patient’s occupational history was collected and analyzed.
The bibliographic data was found on the PUBMED bibliographic search site after entering
the word “extrahepaticangiosarcoma”. We report a case of adrenal epithelioidangiosarcoma
(AEA) in a 68 yr-old Caucasian male factory worker exposed to Vinyl Chloride (VC) for
15 yr. He underwent surgery, chemotherapy and radiotherapy. Hepatic angiosarcoma is a
known consequence of VC exposure, but occupational causality of extra-hepatic angiosarcoma
is controversial. Extra-hepatic angiosarcomas have been reported in VC workers, but never
AEA. Cancerogenic effects of VC involve all endothelial areas of the body and
extra-hepatic endothelial tumors may also be caused by this substance. This is the first
published report of AEA diagnosed in a worker exposed to VC.
Introduction
Angiosarcoma is a rare malignant tumor (less than 1% of sarcomas), mainly localized in the
skin and superficial soft tissue1,2,3). Angiosarcomas have been reported as primary neoplasms in
numerous other sites, including breast, thyroid, heart, lung, pulmonary artery, liver,
spleen, kidney, adrenal gland, uterus, ovary, vagina, testis, bone, and serous
membranes4,5,6,7,8,9,10,11,12,13,14,15,16,17). Etiologic factors related to angiosarcomas are exposure to
arsenic18), thorium
dioxide19,20,21), vinyl chloride monomers22, 23), and therapeutic irradiation24,25,26,27). Since 1974, several reports have appeared regarding a
distinct relationship between exposure to vinyl chloride monomers and angiosarcomas of the
liver28,29,30,31,32,33,34). Adrenal epithelioidangiosarcoma (AEA) is one such rare
neoplasm, as reflected by its limited documentation in the literature. It is usually a very
aggressive tumor, and surgery is the treatment of choice with or without adjuvant therapy,
depending on the histopathological stage and subsequent prognostic factors. The most common
presenting symptoms are non-specific and include slight fever, anorexia, fatigue and chronic
pain, although the disease is frequently asymptomatic, as reported by Wenig et
al.2, 35,36,37). Finally bibliographic evidence is presented, found on the
PUBMED bibliographic search site after entering the word “extrahepaticangiosarcoma”.
Case Presentation


In April 2011, a 68 yr old Caucasian male was admitted to the surgery clinic at the General
Hospital “Perrino” in Brindisi (Italy) because of a pain in the left thorax. A CT scan
showed a suprarenal mass of 7 cm with intra-parenchymal calcifications and dishomogeneous
enhancement in contact with the gastric wall, left renal vein and splenic vessels (Fig. 1). On April 20, the patient underwent a
laparoscopic ablation of the suprarenal mass. Subsequently, in July 2011, a CT-PET showed
metastatic lesions in T4 and T5 and chemotherapy with anthracyclines was started in the
Oncology Clinic. In August 2011, a bone scan was required due to diffuse skeletal pain and
showed vertebral and costal metastases. Radiotherapy with a single fraction of 8 Gy to the
painful portion of the chest was performed. Pain control was unsuccessful since the Visual
Analogue Scale score remained constant (score 7–8). The patient died of neoplastic cachexia
in November 2011.The man had worked as a compressor operator from 1962–1972 at a chemical
factory in southern Italy, in a storage facility with vinyl chloride (VC). In 1991, the
sector management compiled a list of workers exposed to VC after 1970. On that list the man
resulted exposed to >500 ppm of VC from 1970 to 1972. From 1988 to 1993, the man worked
on the production of Polyvinyl Chloride (PVC) pipes from PVC waste material. The tumor was
diagnosed in 2011, 39 yr after his last direct VC exposition and 18 yr after working with
PVC. The tumor was surgically excised along with surrounding adipose tissue. The adrenal
gland had a nodular aspect and measured 8 × 5 × 4.5 cm, with a weight of 100 g. The cut
surface showed a variegated aspect with hemorrhagic areas infiltrating the residual adrenal
tissue, with a central zone of calcific fibrosis. Hematoxylin and eosin-stained sections of
the adrenal gland revealed a neoplasm characterized by predominantly epithelioid malignant
endothelial cells forming rudimentary vascular channels. These channels infiltrated the
surrounding adrenal tissue, which was diffusely hyperplastic; they had an irregular shape
and formed intercommunicating sinusoids with endothelial papillae (Fig. 2). Malignant epithelioid cells had abundant eosinophilic
cytoplasm and high nuclear grade with vescicular nuclei and prominent nucleoli. In some
areas the neoplastic cells had a prevalent solid pattern with slit-like vascular spaces.
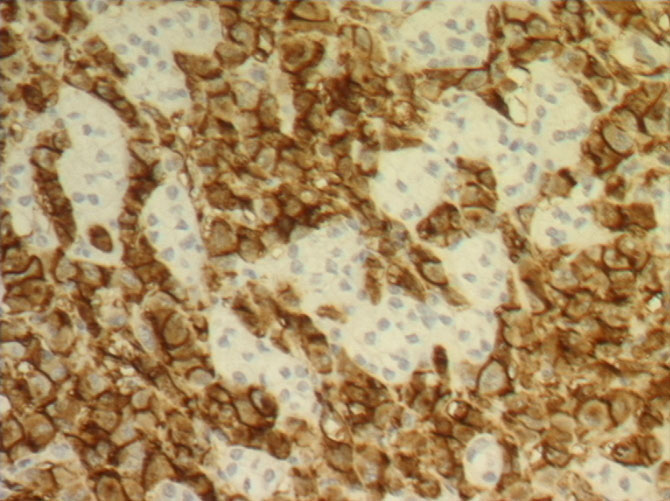
Wide fibrosis with microcalcifications was also present. Immunohistochemically, the
neoplastic cells were strongly and diffusely positive for platelet endothelial cell adhesion
molecule (PECAM-1) also known as cluster of differentiation 31 (CD31) (Fig. 3), Human von Willebrand Factor (Factor VIII-related antigen)
and focally positive for CKAE1AE3. Immunostains for is a cluster of differentiation molecule
(CD34), Inhibin Alpha and S100 were negative.
Discussion and Conclusion
AEA are extremely rare neoplasms. AEA must be differentiated from other neoplasms of the
adrenal gland such as adrenal cortical carcinoma, pheochromocytoma, metastatic carcinoma,
and metastatic malignant melanoma, but in all cases the immunohistochemical markers are a
good tool for differential diagnosis. AEA is a biologically malignant neoplasm that can
infiltrate locally and metastasize37). The etiology of the epitheloidangiosarcoma remains unknown.
There are only four cases described in the literature where the malignancy could be linked
with prolonged exposure to arsenic-containing insecticides and presence of mesenteric
fibromatosis. No other connection or correlation with a family history of adrenal neoplasms
(suggesting Multiple Endocrine Neoplasia syndrome), a prior history of abdominal
radiotherapy or long-term androgenic anabolic steroid treatment could be found36, 38). The disease generally affects more men than women
(21 men, 8 women, 1 not specified) with a wide age range from 34 to 85 yr, predominantly
patients in their 60s and 70s. The disease usually starts with pain and presence of
abdominal mass, followed by significant weight loss, fever episodes and weakness. In six
cases described in the literature the disease was asymptomatic but in four cases it was
associated with paraneoplastic syndrome and distant metastases to bone and liver38, 39). One patient had an unusual association with
Cushing’s disease while in one patient an adrenal tumor had accidentally been
discovered40, 41). In the sixth asymptomatic
patient, the angiosarcoma was revealed after surgery for abdominal trauma and suspected
hepatic rupture was performed42). Rasore-Quartino and Kern published the first two cases in
the late 1960s, but due to a lack of immunohistochemical analyses they are excluded from
this study43, 44). The first case confirmed by
immunohistochemical staining was published in 1988 by Kareti3). Several single case reports followed until Wenig et
al. described the largest study in 1994 where nine cases of adrenal angiosarcoma were
analyzed (eight new cases plus one previously published by Karety)36, 40, 45,46,47,48,49). Macroscopically the tumors varied from well-circumscribed to
invasive retroperitoneal masses, solid to cystic, with size from 5 to 16 cm in diameter. All
the cases described in the literature tended toward an epithelioid appearance. Among them 19
had immunoreactivity for keratins while only 3 were negative35, 36, 38,
39, 42, 46, 47, 52,
54,55,56,57,58,59). Reactivity for cytokeratin is typical of
epithelioidmorphology and is believed to represent aberrant or “atavistic” expression. Human
von Willebrand Factor (Factor VIII-related antigen) and platelet endothelial cell adhesion
molecule (PECAM-1) also known as cluster of differentiation 31 (CD31) positivity was
detected in 7 cases and 16 cases, respectively35, 36,
40,41,42, 47, 52,53,54,55,56,57,58,59). Prompt preoperative diagnosis is very complex since the
tumors can appear well-circumscribed and non-contrast-enhancing, suggesting a benign,
non-neoplastic formation. Their irregular histological and immunological attributes as well
as their relatively low incidence can cause pathologists to mistake them for adrenal
epithelial neoplasms. In clinical practice these neoplasms should always be differentiated
from other vascular neoplasms, pheochromocytoma, adrenal cortical carcinoma, metastatic
adenocarcinoma, metastatic malignant melanoma and other metastatic tumors as well as from
benign neoplasms such as adrenal adenomas with hemorrhage and
epithelioidhemangioendothelioma36, 38,
40, 50,51,52). The safest and easiest way to confirm or rule out this
malignancy is by using immunohistochemistry. Endothelial-related markers (CD34, Factor VIII
antigen and CD31) must be used in the antigen panel of these tumors, following their
limitations in terms of sensitivity and specificity36). The adrenal angiosarcoma is a malignant neoplasm that can
invade surrounding organs and tissue as well as metastasize in distant sites.
Epithelioidangiosarcoma of the adrenal gland may mimic much more common primary and
secondary tumors, and in view of cytokeratin positivity, especially metastatic carcinoma.
Despite its rarity, knowledge of its existence is important as its pathobiologic
characteristics may differ markedly from other primary and metastatic adrenal neoplasms.
Because of the infrequency of this entity, optimal therapy other than surgical eradication
is difficult to determine. The complete surgical resection of the adrenal gland with or
without any surrounding tissue or organ infiltrated with the tumor has good outcome despite
the biology of this tumor. Some cases may have been detected at an early enough stage to
enable surgical cure. In view of the aggressive nature of angiosarcoma in all sites,
adjuvant therapy appears justified for patients in whom complete surgical extirpation cannot
be ensured. Complete eradication combined with 3- to 6-month control intervals are essential
for detection of presence of local recurrence or distant metastases and their treatment with
adjuvant chemo- or radiotherapy. Presence of local or distant metastases at the time of the
primary detection of the tumor or in the first 6 months postoperatively is a negative
prognostic parameter that shortens the overall survival of the patient. This is the first
published report of adrenal angiosarcoma diagnosed in a worker exposed to VC.
References
- 1) Enzinger
FM (2001)
Malignant vascular tumors. In: Soft Tissue tumors, 4th Ed. Mosby, St.
Louis.
- 2) Lack
EE, Graham
CW, Azumi
N (1991)
Primary leiomyosarcoma of the adrenal gland: case report with
immunohistochemical and ultrastructural study. Am J Surg
Pathol
15, 899–905.
- 3) Kareti
R, Katlein
S, Siew
S, Blauvelt
A (1988)
Angiosarcoma of the adrtenal gland. Arch Pathol
Lab Med
112, 1163–5.
- 4) Macías-Martinez
V,
Murrieta-Tiburcio
L,
Molina-Cardenas
H,
Domínguez-Malagón
H (1997)
Epithelioidangiosarcoma of the breast: clinicopathological,
immunohistochemical, and ultrastructural study of a case. Am J
Surg Pathol
21, 599–604.
- 5) Eusebi
V, Carcangiu
ML, Dina
R, Rosai
J (1990)
Keratin-positive epithelioidangiosarcoma of the thyroid: a report of four
cases. Am J Surg Pathol
14, 737–47.
- 6) Wakely
PEJr (1987)
Angiosarcoma of the heart in an adolescent. Arch
Pathol Lab Med
111, 472–5.
- 7) Sheppard
MN, Hansell
DM, Du Bois
RM, Nicholson
AG (1997)
Primary epithelioidangiosarcoma of the lung presenting as pulmonary
hemorrhage. Hum Pathol
28, 383–5.
- 8) Goldblum
JR, Rice
TW (1995)
Epithelioidangiosarcoma of the pulmonary artery.
Hum Pathol
26, 1275–7.
- 9) Popper
H, Thomas
LB, Telles
NC, Falk
H, Selikoff
IJ (1978)
Development of hepatic angiosarcoma in man induced by vinyl chloride,
thorotrast, and arsenic: comparison with cases of unknown etiology.
Am J Pathol
92, 349–76.
- 10) Falk
H, Thomas
LB, Popper
H, Ishak
KG (1979)
Hepatic angiosarcoma associated with androgen-anabolic
steroids. Lancet
2, 1120–3.
- 11) Falk
S, Krishnan
J, Meis
JM (1993)
Primary angiosarcoma of the spleen: a clinicopathologic study of 40
cases. Am J Surg Pathol
17, 959–70.
- 12) Schammel
DP, Tavassoli
FA (1998)
Uterine angiosarcomas: a morphologic and immunohistochemical study of
four cases. Am J Surg Pathol
22, 246–50.
- 13) Nucci
MR, Krausz
T,
Lifschitz-Mercer
B, Chan
JK, Fletcher
CD (1998)
Angiosarcoma of the ovary: clinicopathologic and immunohistochemical
analysis of four cases with a broad morphologic spectrum. Am J
Surg Pathol
22, 620–30.
- 14) McAdam
JA, Stewart
F, Reid
R (1998)
Vaginal epithelioidangiosarcoma. J Clin
Pathol
51, 928–30.
- 15) Masera
A, Ovcak
Z, Mikuz
G (1999)
Angiosarcoma of the testis. Virchows
Arch
434, 351–3.
- 16) Marthya
A,
Patinharayil
G, Puthezeth
K, Sreedharan
S, Kumar
A, Kumaran
CM (2007)
Multicentricepithelioidangiosarcoma of the spine: a case report of a rare
bone tumor. Spine J
7, 716–9.
- 17) Lin
BTY, Colby
T, Gown
AM, Hammar
SP, Mertens
RB, Churg
A, Battifora
H (1996)
Malignant vascular tumors of the serous membranes mimicking mesothelioma:
a report of 14 cases. Am J Surg Pathol
20, 1431–9.
- 18) Regelson
W, Kim
U, Ospina
J, Holland
JF (1968)
Hemangioendothelial sarcoma of liver from chronic arsenic intoxication by
Fowler’s solution. Cancer
21, 514–22.
- 19) Ito
Y, Kojiro
M, Nakashima
T, Mori
T (1988)
Pathomorphologic characteristics of 102 cases of thorotrast-related
hepatocellular carcinoma, cholangiocarcinoma, and hepatic angiosarcoma.
Cancer
62, 1153–62.
- 20) Macmahon
HE, Murphy
AS, Bates
MI (1947)
Endothelial cell sarcoma of liver following thorotrast
injections. Am J Pathol
23, 585–611.
- 21) Naka
N, Ossawa
M, Tomita
Y, Kanno
H, Uchida
A, Aozasa
K (1995)
Angiosarcoma in Japan. A review of 99 cases.
Cancer
75, 989–96.
- 22) Falk
H (1983) Vinyl
chloride and polyvinyl chloride. In: Environmental and occupational medicine, Rom W (Ed.),
pp 579–588, Little, Brown, Boston.
- 23) Thomas
LB, Popper
H, Berk
P, Selikoff
I, Falk
H (1975)
Vinyl-chloride-induced liver disease. From idiopathic portal hypertension
to angiosarcomas. N Engl J Med
292, 17–22.
- 24) Brady
MS, Gaynor
JJ, Brennan
MF (1992)
Radiation-associated sarcoma of bone and soft tissue.
Arch Surg
127, 1379–85.
- 25) Cafiero
F, Gipponi
M, Peressini
A, Queirolo
P, Bertoglio
S, Comandini
D, Percivale
P, Sertoli
MR, Badellino
F (1996)
Radiation associated angiosarcoma: diagnostic and therapeutic
implications-two case reports and a review of the literature.
Cancer
77, 2496–502.
- 26) Chen
KTK, Hoffman
KD, Hendricks
EJ (1979)
Angiosarcoma following therapeutic irradiation.
Cancer
44, 2044–8.
- 27) Fineberg
S, Rosen
PP (1994)
Cutaneous angiosarcona and atypical vescular lesions of the skin and
breast after radiation therapy for breast carcinoma. Am J Clin
Pathol
102, 757–63.
- 28) Baxter
PJ, Anthony
PP, MacSween
RN, Scheuer
PJ (1977)
Angiosarcoma of the liver in Great Britain, 1963–73.
BMJ
2, 919–21.
- 29) Creech
JL, Johnson
MN (1974)
Angiosarcoma of the liver in the manufacture of polynyl
chloride. J Occup Med
16, 150–1.
- 30) Doll
R (1988)
Effects of exposure to vinyl chloride. An assessment of the
evidence. Scand J Work Environ Health
14, 61–78.
- 31) Jones
RD, Smith
DM, Thomas
PG (1988)
A Mortality study of vinyl chloride monomer workers employed in the
United Kingdom in 1940–1974. Scand J Work Environ
Health
14, 153–60.
- 32) Pirastu
R, Comba
P, Reggiani
A, Foa
V, Masina
A, Maltoni
C (1990)
Mortality from liver disease among Italian vinyl chloride
monomer/polyvinyl chloride manufacturers. Am J Ind Med
17, 155–61.
- 33) Wong
O, Whorton
MD, Foliart
DE, Ragland
D (1991)
An industry-wide epidemiologic study of vinyl chloride workers,
1942–1982. Am J Ind Med
20, 317–34.
- 34) Wu
W, Steenland
K, Brown
D, Wells
V, Jones
J, Schulte
P, Halperin
W (1989)
Cohort and case-control analyses of workers exposed to vinyl
chloride. J Occup Med
31, 518–23.
- 35) MayayoArtal
E,
Gomez-Aracil
V,
Sole-Poblet
JM, Pereira
Lopez
JA (2002)
Epithelioidangiosarcoma of the adrenal gland. Report of a
case. Arch Esp Urol
55, 261–4.
- 36) Wenig
BM,
Abbondanzo
SL, Heffess
CS (1994)
Ephitelioidangiosarcoma of the adrenal gland. A clinicopatholocical study
of nine cases with a discussion of the implication of finding epithelial specific
markers. Am J Surg Pathol
18, 62–73.
- 37) Stavridis
S, Mickovski
A, Filipovski
V, Banev
S, Dohcev
S, Lekovski
L, (2010)
Epithelioid Angiosarcoma of the Adrenal Gland. Report of a case and
Rewiew of the Literature. Macedonian Journal of Medical
Sciences
3, 388–94.
- 38) Jochum
W, Schroder
S, Risti
B, Marincek
B, von
Hochstetter
A (1994)
Cytokeratin-positive angiosarcoma of the adrenal gland.
Pathologe
15, 181–6.
- 39) Bosco
PJ, Silverman
ML, Zinman
LM (1991)
Primary angiosarcoma of adrenal gland presenting as paraneoplastic
syndrome: case report. J Urol
146, 1101–3.
- 40) Croitoru
AG, Klausner
AP, Mc
Williams
G, Unger
PD (2001)
Primary epithelioidangiosarcoma of the adrenal gland.
Ann Diagn Pathol
5, 300–303.
- 41) Ferrozzi
F, Tognini
G, Bova
D, Zuccoli
G, Pavone
P (2001)
Hemangiosarcoma of the adrenal glands: CT findings in two
cases. Abdom Imaging
26, 336–9.
- 42) Gambino
G, Mannone
T, Rizzo A
Scio
A, Branca
M, Airò
Farulla
M, Guccione
M, Spallitta
IS, Nicoli
N (2008)
Adrenalepithelioid angiosarcoma: a case report.
Chir Ital
60, 463–7.
- 43) Rasore-Quartino
A (1967)
Congenitaladrenaltumor (angiosarcoma) in a monozygotic
twin. Pathologica
59, 153–8.
- 44) Kern
WH, Smart
RD, Sherwin
RP (1967)
Angiosarcoma of lungs and adrenal gland: unusual clinical and pathologic
manifestations. Minn Med
50, 1339–43.
- 45) Caplan
RH, Kisken
WA, Huiras
CM (1991)
Incidentally discovered adrenal masses. Minn
Med
74, 23–6.
- 46) Livaditou
A, Alexiou
G, Floros
D, Filippidis
T, Dosios
T, Bays
D (1991)
Epithelioid angiosarcoma of the adrenal gland associated with cronic
arsenic intoxication?Pathol Res Pract
187, 284–9.
- 47) Ben-Izhak
O, Auslander
L, Rabinson
S, Lichtig
C, Sternberg
A (1992)
Epithelioidangiosarcoma of the adrenal gland with cytokeratin expression.
Report of a case with accompanying mesenteric fibromatosis.
Cancer
69, 1808–12.
- 48) Fiordelise
S, Zangrandi
A, Tronci
A, Rovereto
B, Valentino
RV, Bezzi
E (1992)
Angiosarcoma of the adrenal gland: case report.
Arch Ital Urol Nefrol Androl
64, 341–3.
- 49) Schwenk
W, Sarbia
M, Haas
R, Stock
W (1994)
Primary hemangiosarcoma as a rare form of an incidentally discovered mass
of the adrenal glands. Dtsch Med Wochenschr
119, 217–21.
- 50) McCleary
AJ (1994)
Massive haemothorax secondary to angiosarcoma.
Thorax
49, 1036–7.
- 51) Sasaki
R, Tachiki
Y, Tsukada
T, Miura
K, Kato
T, Saito
K (1995)
A case of adrenal angiosarcoma. Nippon Hinyokika
Gakkai Zasshi
86, 1064–7 (in Japanese).
- 52) Abboud
E, Weisenberg
E, Khan
S, Rhone
DP (1999)
Pathologic quiz case. Arch Pathol Lab
Med
123, 157–8.
- 53) Invitti
C,
PecoriGiraldi
F, Cavagnini
F, Sonzogni
A (2001)
Unusual association of adrenal angiosarcoma and Cushing’s
disease. Horm Res
56, 124–9.
- 54) Krüger
S, Kujath
P,
Johannisson
R, Feller
AC (2001)
Primary epithelioidangiosarcoma of the adrenal gland. Case report and
review of the literature. Tumori
87, 262–5.
- 55) Rodríguez-Pinilla
SM,
Benito-Berlinches
A, Ballestin
C, Usera
G (2002)
Angiosarcoma of adrenal gland report of a case and review of the
literature. Rev Esp Patol
352, 227–32.
- 56) Pasqual
E, Bertolissi
F, Grimaldi
F, Beltrami
CA, Scott
CA, Bacchetti
S, Waclaw
BU, Cagol
PP (2002)
Adrenal angiosarcoma: report of a case. Surg
Today
32, 563–5.
- 57) Sidoni
A, Magro
G, Cavaliere
A, Scheibel
M, Bellezza
G (2003) Primaryadrenal
angiosarcoma. Pathologica
95, 60–3.
- 58) Galmiche
L, Morel
HP, Moreau
A, Labrosse
PA, Coindre
JM, Heymann
MF (2004)
Primaryadrenal angiosarcoma. Ann Pathol
24, 371–3.
- 59) Azurmendi
Sastre
V, Llarena
Ibarguren
R, Eizaguirre
Zarza
B, Pertusa
Peña
C (2004)
Adrenalspindlecell angiosarcoma. Report of one case.
Arch Esp Urol
57, 156–60.
