臨床経験
直腸脱および直腸重積に対するlaparoscopic ventral rectopexyの術後QOL
キーワード:
laparoscopic ventral rectopexy,
QOL
2013 年 46 巻 9 号 p. 708-716
詳細
2013 年 46 巻 9 号 p. 708-716
目的:便失禁を有する直腸脱および直腸重積に対するlaparoscopic ventral rectopexy(以下,LVRと略記)術後のQOLを評価した.方法:対象は18例で,便失禁はfecal incontinence severity index(FISI),便秘はconstipation scoring system(CSS)で評価し,QOLはshort-forum 36 health survey(以下,SF-36と略記)とfecal incontinence quality of life scale(以下,FIQLと略記)を用いて術前と術後3~6か月に評価した.結果:便失禁と便秘は術後有意に改善した(P<0.0001,P=0.005).SF-36は五つの下位尺度で術後有意に改善した.FIQLは四つの下位尺度で術後有意に改善した.結語:直腸脱および直腸重積に対するLVRは術後短期において排便障害ならびにQOLを改善することが示唆された.
直腸脱は,external rectal prolapse(以下,ERPと略記)の文字どおり,直腸が全層性に肛門外に脱出するもので1),直腸重積はinternal rectal prolapse(以下,IRPと略記)ともいわれ,排便時などに直腸および肛門管内で直腸が重積することをいう2).IRPは無症状者でもみられることがあるが3),重積が進行するにつれて脱出感,疼痛,出血,粘液分泌,掻痒,テネスムス,便意促迫,便失禁,排便困難などの原因になる4).最近の研究によれば,IRPはERPに進展する可能性が示唆されており,その病態生理は共通すると考えられている5)6).IRPは症状に応じて内科的治療が優先されるが,無効の際には外科的治療の適応である.ERPと同様に,IRPの外科的治療には経腹的手術と経肛門的手術がある.経腹的手術のうち最近注目されている術式としてlaparoscopic ventral rectopexy(以下,LVRと略記)がある7).LVRはposterior rectopexyと異なり,直腸ならびに左側結腸を支配する自律神経の損傷がないことで,術後の便秘を来すことなく,便失禁の改善が得られるとされ,ERPおよびIRPの両者に適用され,良い成績が示されている7)~9).しかし,LVR術後のQOLについてほとんど知見がない.本研究の目的は便失禁を有するERPおよびIRPに対するLVR術後の健康関連QOLを評価することである.
2011年9月から2012年12月までの16か月間にERPまたは,IRPのためにLVRを行ったのは36例である.このうち,術後経過が3か月未満の11例,統合失調症など精神疾患を併存した5例,術前に便失禁が認められなかったIRPの2例の計18例を除く18例を対象とし,インフォームド・コンセントを得たうえで術前後のQOLを評価した.
ERPは視診で確認するか,または排便造影で肛門外に全層性に直腸が脱出する所見で診断された.IRPは便失禁または,排便困難などを主訴として来院した患者に行った排便造影で診断された.IRPの手術適応はCollinsonら8)の報告に準じた.すなわち,排便造影に基づくIRPの分類にOxford prolapse grade(以下,OPGと略記)があるが10),このうち排便時に直腸重積の先進部が肛門管上(OPG 3度)または肛門管内(OPG 4度)に位置する症例で,かつ排便コントロール,便性改善,止痢剤,などの内科的治療で奏効しない場合にLVRの適応とした.年齢,性,American Society of Anesthesiologistsの術前状態分類(以下,ASA-PSと略記),手術時間,出血量,入院期間,術後合併症について前向きに記録を行った.排便機能の評価については,便失禁はfecal incontinence severity index(以下,FISIと略記)11)(Table 1)で,便秘はconstipation scoring system(以下,CSSと略記)12)(Table 2)で,術前と術後3~6か月に評価した.QOLは包括的尺度であるshort-forum 36 health survey(以下,SF-36と略記)と便失禁患者専用の尺度であるfecal incontinence quality of life scale(以下,FIQLと略記)を用いて,排便機能の評価と同時期に調査を行った.なお,SF-36およびFIQLの日本語版(Fig. 1)の妥当性はすでに確認されている13)14).
| Type | Never | 1–3 times per month | Once per week | Twice per week | Once per day | More than twice per day |
|---|---|---|---|---|---|---|
| Gas | 0 | 4 | 6 | 8 | 11 | 12 |
| Mucus | 0 | 3 | 5 | 7 | 10 | 12 |
| Liquid stool | 0 | 8 | 10 | 13 | 17 | 19 |
| Solid stool | 0 | 8 | 10 | 13 | 16 | 18 |
| Symptom | 0 | 1 | 2 | 3 | 4 |
|---|---|---|---|---|---|
| Frequency of bowel movements | 1–2 times per 1–2 days |
2 times per week | Once per week | Less than once per week | Less than once per month |
| Difficulty: painful evacuation effort | Never | Rarely | Sometimes | Usually | Always |
| Completeness: feeling incomplete evacuation | Never | Rarely | Sometimes | Usually | Always |
| Pain: abdominal pain | Never | Rarely | Sometimes | Usually | Always |
| Time: minutes in lavatory per attempt | Less than 5 | 5–10 | 10–20 | 20–30 | More than 30 |
| Assistance: type of assistance | Without assistance | Stimulative laxatives | Digital assistance or enema | ||
| Failure: unsuccessful attempts for evacuation per 24 hours | Never | 1–3 | 3–6 | 6–9 | More than 9 |
| History: duration of constipation (yr) | 0 | 1–5 | 5–10 | 10–20 | More than 20 |
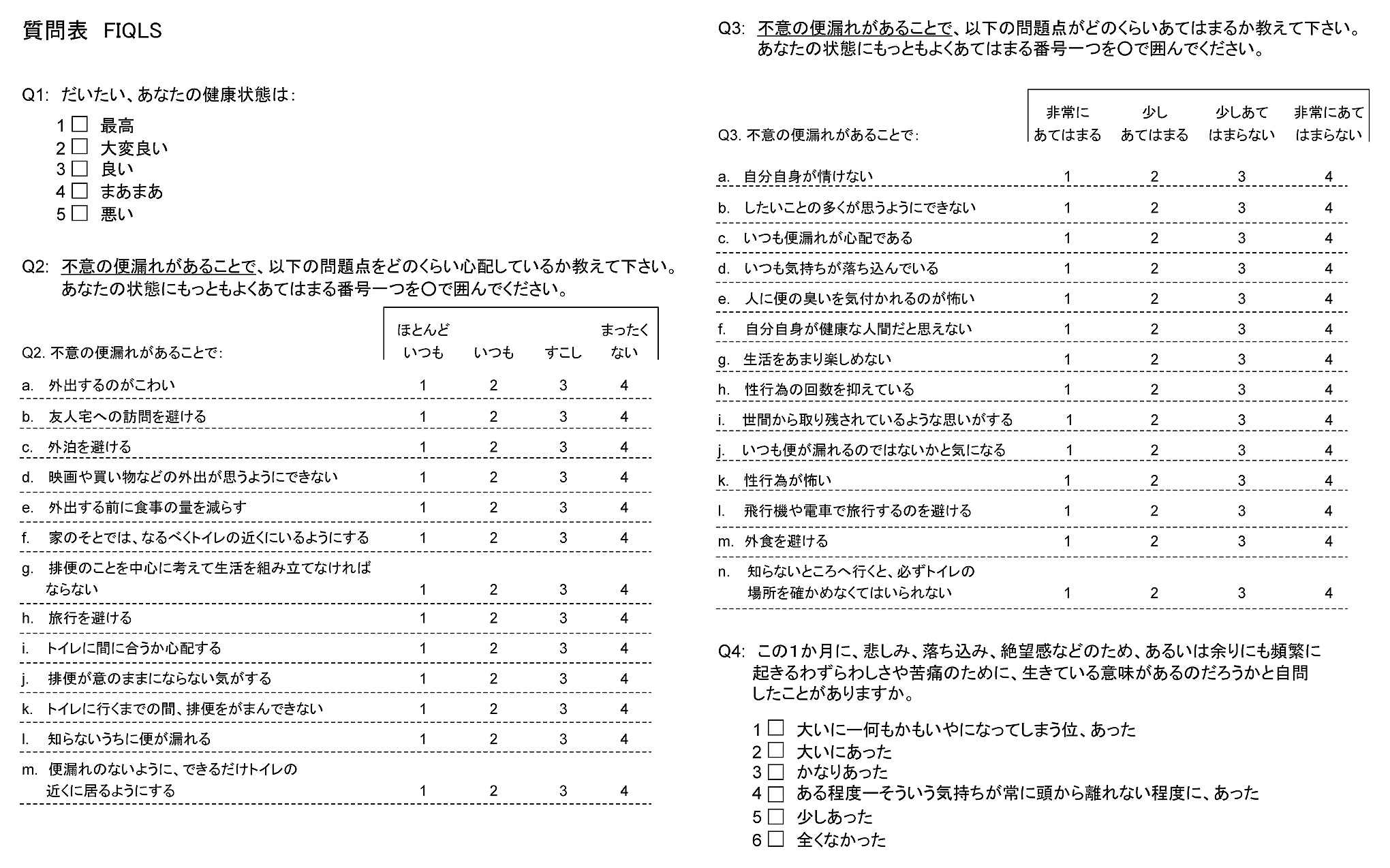
The Japanese version of the fecal incontinence quality of life scale.
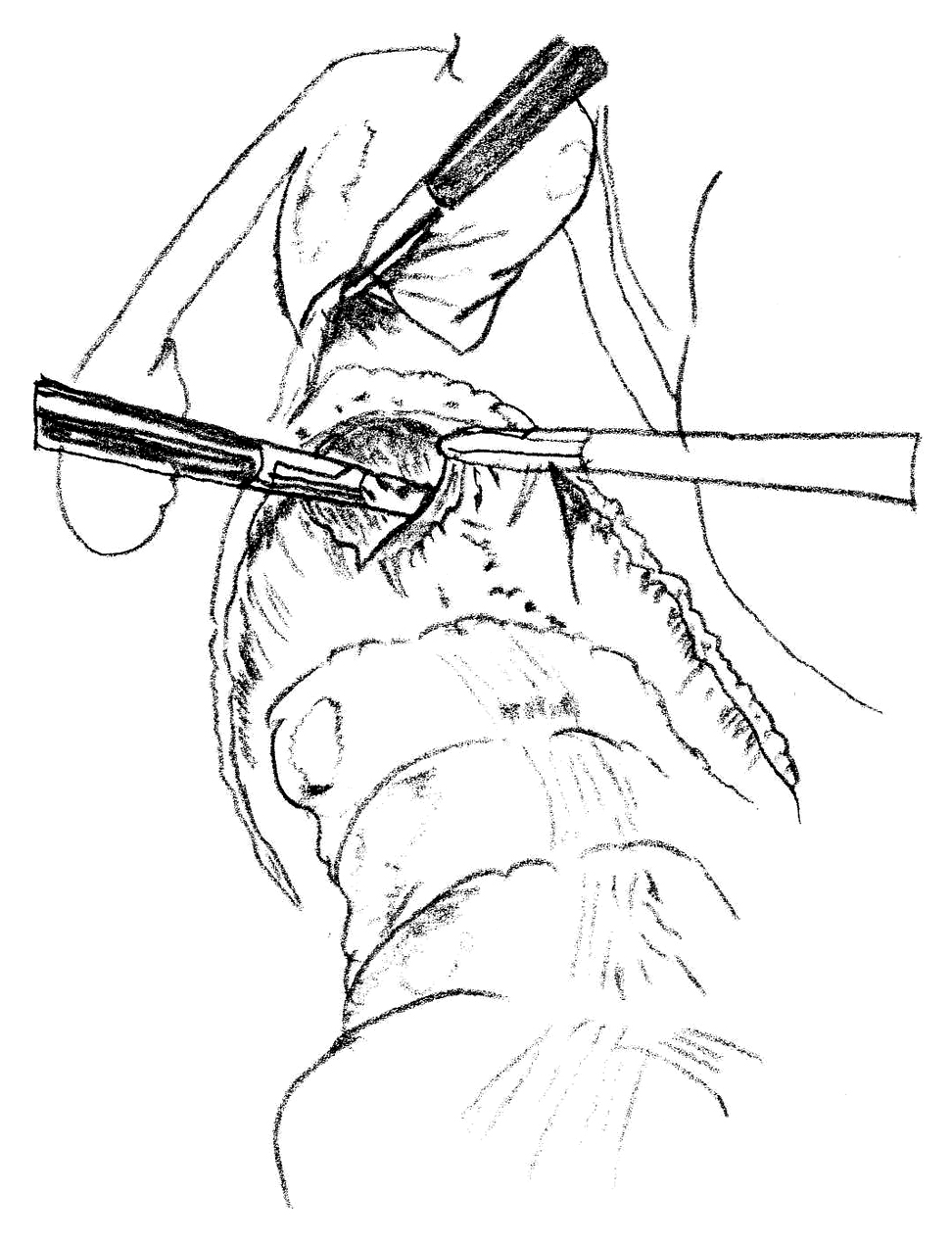
LVRの手技は基本的にD’Hooreら7)の方法に準じた(Fig. 2~5).我々は臍下にopen techniqueで第1トロカー(12 mm)を入れた後,右腸骨窩(10 mm),左腸骨窩(5 mm),左右の側腹部(5 mm)にトロカーを入れ,5孔式で行っている.子宮は直針を用いて2-0ナイロン糸で子宮底部を貫通して前腹壁に吊り挙げる.仙椎岬角の右側腹膜の切開から始めて,直腸間膜・右側縁の腹膜切開に連続させ,ダグラス窩右縁に達した後,ダグラス窩左縁まで腹膜を切開する.直腸膣中隔を骨盤底のレベルまで剥離し,直腸診で確認する.Polypropylene meshを3×17 cmにトリミングし,その一端を骨盤底に近接した下部直腸の前壁にnon absorbable braided polyester suture(2-0 Tycron, Covidien, USA)6針を用いて縫合固定する.他端はstaple(EndopathTM EMS; Ethicon Endo-Surgery INC., USA)を用いてmeshを過度に牽引しないで岬角の右側骨膜に固定し,余剰のmeshは切除する.続いて膣円蓋部をmeshに2針で縫合固定する.切開した腹膜を吸収糸(3-0 Vicryl, Ethicon LTD., Japan)で連続縫合してmeshを腹膜外に位置する.男性では直腸膀胱窩から骨盤底まで剥離し,meshを下部直腸前壁に縫合し岬角に固定する.データは中央値(範囲)で示す.群間比較はカテゴリー変数ではカイ二乗検定で,連続変数では対応のない場合はMann-Whitney U test,対応のある場合はWilcoxon signed rank testを用いた.P<0.05を有意差ありとした.

The schema of ventral rectopexy. The ventral portion of the mesh allows correction of rectorectal intussception.

Dissection starts at the sacral promontory. The dotted line shows the caudal extension of the peritoneal incision.
The rectovaginal septum is opened without any lateral dissection.

A strip of polypropylene mesh is sutured to the anterior aspect of the rectum and fixed without traction on the sacral promontory.
LVRが行われた18例のうちERPとIRPはおのおの10例,8例であった.全例女性であり,年齢は76(57~88)歳で,80歳以上が7例(39%)であった.ASA-PSは2(1~2)である.手術時間は201(157~319)分,出血量は10(0~150)ml,術後入院期間は4(1~7)日であった.術後合併症は創感染 3例,port-site hernia 1例,皮下出血1例認められ,port-site hernia併発例は術後9日に発症し再入院後に緊急手術を行った.感染,直腸・膣びらんなどmeshに関連する合併症は認められなかった.術後経過観察期間は8.5(3~15)か月で,この間にERPの再発はない.しかし,ERP 術後2例でIRPの発症を認め,術後の排便機能とQOLを調査した後にDelorme手術と高周波による粘膜凝固15)をおのおの行った(Table 3).
排便機能については,FISIは術前32.5(19~54),術後14(0~35)と便失禁は術後有意に改善し(P<0.0001)(Table 4),疾患別でも同様であった(Table 5, 6).CSSは術前9.5(2~15),術後4(1~14)と便秘は術後有意に改善した(P=0.005)(Table 4).疾患別ではERPでは術後有意に改善したが,IRPでは有意の差は認められなかった(Table 5, 6).
| Outcome | |
|---|---|
| Conversion to open surgery | 0 |
| Operative time (min, range) | 201 (157–319) |
| Blood loss (ml, range) | 19 (0–150) |
| Postoperative hospital stay (days, range) | 4 (1–7) |
| Overall complications | 5/18 (28%) |
| wound infection | 3 |
| port-site hernia | 1 |
| subcutaneous hemorrhage | 1 |
| Internal rectal prolapse found after LVR for ERP | 2 |
LVR, laparoscopic ventral rectopexy; ERP, external rectal prolapse
| Baseline | n | Postoperative | n | P* | |
|---|---|---|---|---|---|
| FISI | 32.5 (19–54) | 18 | 14 (0–35) | 18 | <0.0001 |
| CSS | 9.5 (2–15) | 18 | 4 (1–14) | 18 | 0.005 |
| FIQL | |||||
| Lifestyle | 2.7 (1.1–4.0) | 18 | 3.5 (1.0–4.0) | 18 | 0.01 |
| Coping | 2.4 (1.3–3.9) | 16 | 3.4 (2.2–4.0) | 16 | 0.002 |
| Depression | 2.9 (1.3–4.0) | 16 | 3.6 (2.0–4.1) | 16 | 0.002 |
| Embarrassment | 2.3 (1.0–4.0) | 18 | 3.3 (1.0–4.0) | 18 | 0.001 |
| SF-36 | |||||
| Physical functioning | 57.5 (15–90) | 18 | 65 (25–95) | 17 | 0.03 |
| Role physical | 0 (0–100) | 18 | 75 (0–100) | 17 | 0.18 |
| Pain | 41 (10–100) | 18 | 52 (0–100) | 17 | 0.04 |
| Health perception | 45 (10–72) | 17 | 52 (0–82) | 17 | 0.12 |
| Energy | 45 (5–70) | 17 | 65 (20–85) | 17 | 0.005 |
| Social functioning | 62.5 (12.5–100) | 18 | 87.5 (25–100) | 17 | 0.02 |
| Role emotional | 0 (0–100) | 18 | 100 (0–100) | 17 | 0.06 |
| Mental health | 52 (8–88) | 18 | 76 (24–96) | 17 | 0.005 |
FISI, fecal incontinence severity index; CSS, constipation scoring system; FIQL, fecal incontinence quality of life scale; SF-36, short-forum 36 health survey. * Wilcoxon signed rank test
| Baseline | n | Postoperative | n | P* | |
|---|---|---|---|---|---|
| FISI | 37.5 (19–54) | 10 | 14 (7–20) | 10 | 0.005 |
| CSS | 10 (8–15) | 10 | 4 (1–14) | 10 | 0.011 |
| FIQL | |||||
| Lifestyle | 2.5 (2.0–3.6) | 10 | 3.6 (2.6–4.0) | 10 | 0.03 |
| Coping | 2.2 (1.3–3.4) | 9 | 3.1 (2.3–4.0) | 9 | 0.02 |
| Depression | 2.9 (1.3–4.0) | 9 | 3.6 (2.3–4.1) | 9 | 0.02 |
| Embarrassment | 2.2 (1.0–3.0) | 10 | 3.3 (2.3–4.0) | 10 | 0.01 |
| SF-36 | |||||
| Physical functioning | 65 (20–95) | 10 | 65 (25–95) | 9 | 0.14 |
| Role physical | 0 (0–75) | 10 | 75 (0–100) | 9 | 0.24 |
| Pain | 41 (10–72) | 10 | 52 (41–74) | 9 | 0.04 |
| Health perception | 45 (10–72) | 9 | 52 (32–82) | 9 | 0.09 |
| Energy | 45 (5–70) | 9 | 60 (25–85) | 9 | 0.02 |
| Social functioning | 62.5 (24–100) | 10 | 75 (25–100) | 9 | 0.19 |
| Role emotional | 0 (0–100) | 10 | 100 (0–100) | 9 | 0.07 |
| Mental health | 48 (16–88) | 10 | 88 (40–92) | 9 | 0.01 |
FISI, fecal incontinence severity index; CSS, constipation scoring system; FIQL, fecal incontinence quality of life scale; SF-36, short-forum 36 health survey. * Wilcoxon signed rank test
| Baseline | n | Postoperative | n | P* | |
|---|---|---|---|---|---|
| FISI | 27.0 (20–49) | 8 | 14 (0–35) | 8 | 0.02 |
| CSS | 8 (2–15) | 8 | 3.5 (1–12) | 8 | 0.14 |
| FIQL | |||||
| Lifestyle | 2.8 (1.1–4.0) | 8 | 3.5 (1.0–4.0) | 8 | 0.20 |
| Coping | 2.6 (2.2–3.9) | 7 | 3.8 (2.2–4.0) | 7 | 0.05 |
| Depression | 3.0 (2.1–3.9) | 7 | 3.6 (2.0–4.1) | 7 | 0.06 |
| Embarrassment | 2.5 (1.0–4.0) | 8 | 3.3 (1.0–4.0) | 8 | 0.03 |
| SF-36 | |||||
| Physical functioning | 42.5 (15–95) | 8 | 57.5 (25–95) | 8 | 0.12 |
| Role physical | 0 (0–100) | 8 | 0 (0–100) | 8 | 0.42 |
| Pain | 46.5 (11–100) | 8 | 56.5 (0–100) | 8 | 0.40 |
| Health perception | 42.5 (10–72) | 8 | 51 (0–62) | 8 | 0.46 |
| Energy | 47.5 (5–60) | 8 | 65 (20–85) | 8 | 0.09 |
| Social functioning | 62.5 (25–100) | 8 | 100 (62.5–100) | 8 | 0.04 |
| Role emotional | 16.7 (0–100) | 8 | 100 (0–100) | 8 | 0.45 |
| Mental health | 58 (8–80) | 8 | 64 (24–96) | 8 | 0.23 |
FISI, fecal incontinence severity index; CSS, constipation scoring system; FIQL, fecal incontinence quality of life scale; SF-36, short-forum 36 health survey. * Wilcoxon signed rank test
QOL調査は術前と術後6(3~6)か月に行った.QOL調査票のうちSF-36では1例で術後の回答がまったく得られなかったことと,もう1例が術前の調査で下位尺度のうちenergyとhealth perceptionに含まれる項目で回答数が不足していたために,この二つの下位尺度ではスコアが得られなかった.SF-36の八つの下位尺度のうちphysical functioning,bodily pain,energy,social functioning,mental healthの五つで術後有意の改善がみられた(Table 4).疾患別ではERPではbodily pain,energy,mental healthで術後有意の改善がみられたが,IRPではsocial functioningのみで有意の改善がみられた(Table 5, 6).
FIQLでは18例中2例で術前・術後の両方で,性生活に関する項目Q3H,Q3Kに回答が得られなかったため,下位尺度であるcopingとdepressionのスコアが得られなかった.FIQLの四つの下位尺度は,いずれも術後有意の改善が得られた(Table 4).疾患別ではERPでは,FIQLの四つの下位尺度は全て術後有意の改善が得られたが,IRPではembarrassmentのみで有意の改善が得られた(Table 5, 6).
ERPの手術には経腹手術と経肛門的手術があり,一般的に前者は後者より再発率が小さいので,耐術性があれば経腹手術が勧められている16).経腹手術の代表的なものにposterior rectopexyがあるが,骨盤神経叢から上行して直腸および左側結腸を支配する副交感神経が切離されるため,便失禁は改善されるものの,便秘が増悪することが指摘されている17).これに対してventral rectopexyは直腸後・側方の操作がないために,自律神経の損傷がなく術後の便秘が改善すると報告されている7)~9).本研究でもLVR後にFISIとCSSの両者で有意の改善が認められた.
IRPの手術にも経腹手術と経肛門的手術がある.後者としてstapled trans-anal rectal resection(STARR)18)19)またはinternal Delorm20)が代表的な術式である.STARRは適切な患者選択がされれば,良い術式であるが,内肛門括約筋の損傷,直腸コンプライアンスや直腸貯留能の低下により術後便失禁が出現することが危惧されており21),術前に便失禁を有する患者では適応に注意が必要である.Internal Delormeは経肛門的に直腸粘膜を切除して,筋層を長軸方向に縫縮後に粘膜を合わせる方法で,70~75%で良好な成績が得られているが22)23),ERPに対するDelorme法の長期成績で再発が累積することを考えると24)25),いまだ一定の評価に至っていない.
IRPの経腹手術としてposterior rectopexyが行われたが,結果は不良で便秘が悪化すると報告されている17).その機序は上述した自律神経のdenervationが挙げられており,これを回避するventral rectopexyにより,便失禁と便秘のいずれも改善が得られている9)26).本研究ではLVR後にFISIで有意の改善がみられたが,CSSでは有意の差は認められなかった.
一方,直腸固定術のアプローチで腹腔鏡と開腹を比較すると前者は後者より,術後の疼痛が少なく,入院期間または,術後回復までの期間が短縮するとされている16).自験例では術後合併症は28%に生じているが,諸家の報告1.4~47%27)と比べて遜色なく,ほとんどが創感染のような軽症であった.また,開腹手術へのconvertの経験もなく,LVRは比較的安全な手術ということができる.
LVR術後のQOLに関する報告はキーワードにlaparoscopic ventral rectopexyとquality of lifeを指定してPubMed(1950~2012年)で調べたかぎり,Wongら28)の報告があるのみである.彼らは直腸瘤に小腸瘤やIRPが合併した症例に対するLVRの術後QOLをgastrointestinal quality-of-life indexという調査票で評価し,術後有意の変化が認められなかったとしている.この調査票は消化器疾患患者を対象として症候,身体面,心理面,社会面などでQOLを評価するものである.本研究では対象患者はWongら28)と異なりERPとIRPであり,主症状が便失禁であることに着目し,FIQLで評価した結果,LVR術後に四つの下位尺度全てで有意の改善が認められ,かつ包括的尺度であるSF-36でも五つの下位尺度で有意の改善が認められた.その他,術式は異なるが,便失禁を有する直腸瘤またはIRPの患者に対するSTARR術後のQOLをFIQLで評価した報告では,術後に便秘と便失禁が改善した症例ではFIQLの下位尺度全てで改善したが,術後に便秘と便失禁が改善しなかった症例ではFIQLの下位尺度全てで改善しなかった29).
以上,ERPおよびIRPに対するLVRは,術後短期において便失禁などの排便障害ならびにQOLを改善することが示唆された.本研究は,対象症例が少なく,術後観察期間が短期なことが欠点であり,今後経験症例数を重ねて,長期の観察により合併症,排便機能,QOLなどを再度評価する必要がある.
利益相反:なし