手術記事は,単なる記録ではなく手術内容が理解しやすいことが重要であり,文章のみではなく,絵を多用することで理解度が深まる.執刀医が自ら手術記事を書く意味は,手術内容・局所解剖をどれだけ理解しているかを自問自答する勉強の場でもある.著者は,基本的に手術記事の下書きはせず,よく構図を考え,直接万年筆でシェーマを書き始める.シェーマは術中のビデオなどを参考に模写するよりは,自らも,読者にも理解しやすい構図を意識して書くことが重要である.シェーマが描ければ,手術のその局面を理解できている.逆に書けないということは十分理解していない可能性がある.絵の上手下手,得意不得意はあるが,努力を続ければ,分かりやすい手術記事が書けるようになると考えている.最近執刀した肝胆膵の高難度手術で頻度の高い膵頭十二指腸切除の症例と,恩師に前立をして頂き,肝膵十二指腸切除後5年以上無再発生存症例の手術記事を供覧する.
手術記事は,単なる記録ではなく手術内容が理解しやすいことが重要である.執刀医が自ら手術記事を書くことは,手術内容・局所解剖をどれだけ理解しているかを自問自答する勉強の場であり,学問的な意味を持つ.手術に関する書籍や,術式決定のための論文・ガイドラインは多数存在する一方で,手術記事の記載方法などを論議あるいは解説した文章は少ない1)2).肝胆膵外科医としての研鑽を積んできた著者の実際の手術記事を概説したい.
方法:手術記事の下書きは基本していない.鉛筆などで下書きを始めると書き直しができるものの満足のいく絵になるまで長時間を要し,きりがないと感じているからである.直接万年筆でシェーマを書き始める.よほど気に入らないと新しい紙に書き直すが,よく構図を考え,万年筆で書いている.シェーマは時間的余裕があれば色鉛筆で色を塗るが,通常は動脈を赤で,門脈を青で,胆道を緑で,4色ボールペンを用いて輪郭がわかるようにしている(Fig. 1).
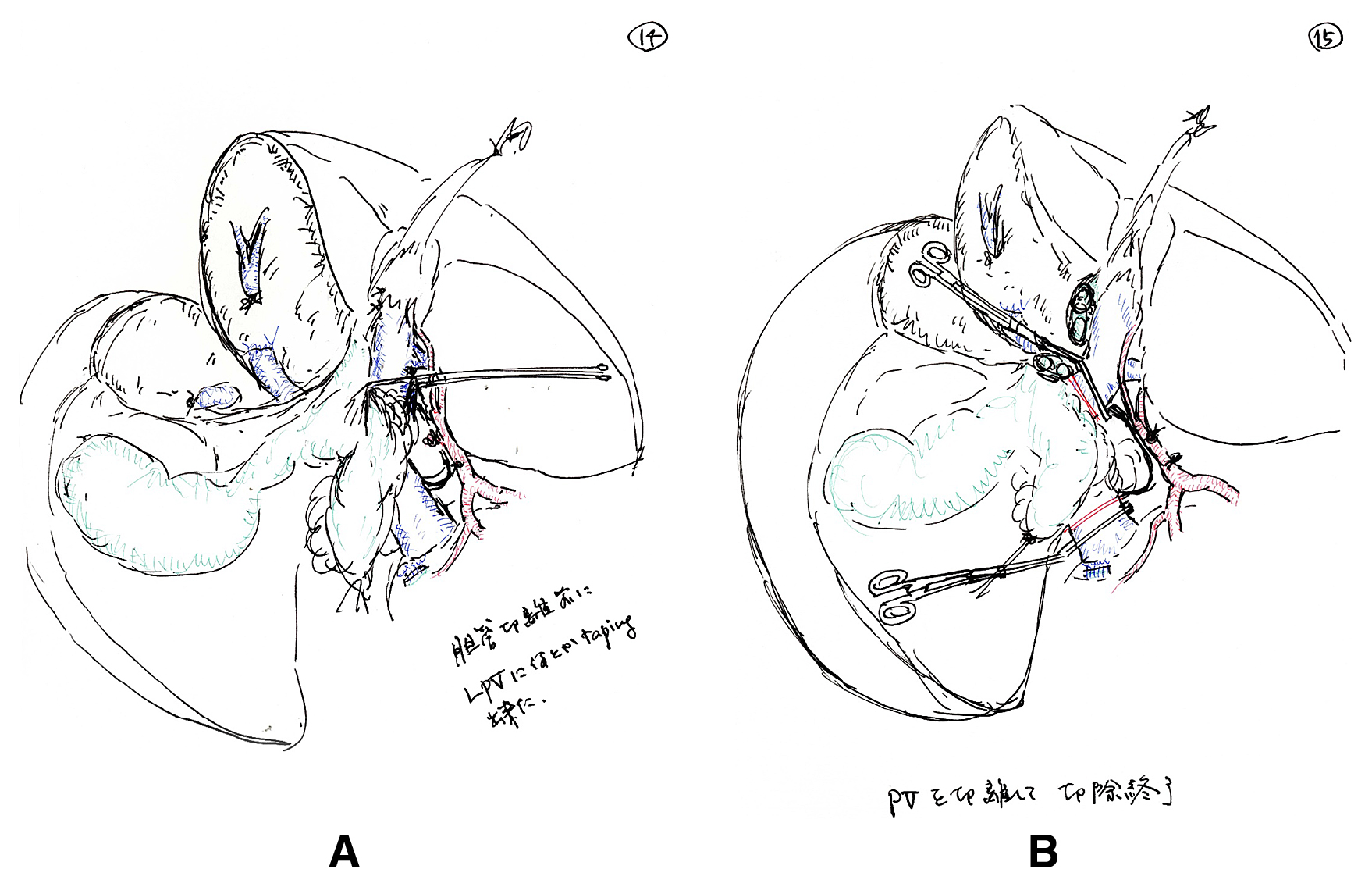
Black and white schematic drawings during a right hepatobiliary resection with portal vein resection and reconstruction using red, blue, and green colors. A: An operative schema just prior to bile duct resection during right hemihepatectomy. B: A schema presenting proximal and distal portal vein resection lines.
手術記事はなるべく記憶が確かなうちに,できれば手術当日に書き上げるべきである.しかし,長時間手術などでは,手術当日に書き上げるのは実際のところ難しいことが多い.まずは,記述すべき項目を箇条書きにしておき,後日そのシェーマを描いていき,少なくとも1週間以内には仕上げておく.手術記事の枚数については,シェーマの大きさなど各外科医のスタイルによって当然違ってくるが,他の外科医などが見ても容易に理解できる手術記事を心がけるべきである.そのためには,シェーマは術中のビデオなどを参考に模写するよりは,自らも,読者にも理解しやすい構図を意識して書くことが最も重要と考えている.
最近執刀した肝胆膵の標準的高難度手術である膵頭十二指腸切除の症例(Fig. 2)と,恩師に前立をして頂き,肝膵十二指腸切除後5年以上無再発生存症例の手術記事を供覧する(Fig. 3).この症例は40年以上前に胆囊摘出と左肝管十二指腸吻合,胃空調吻合術を受けている3).
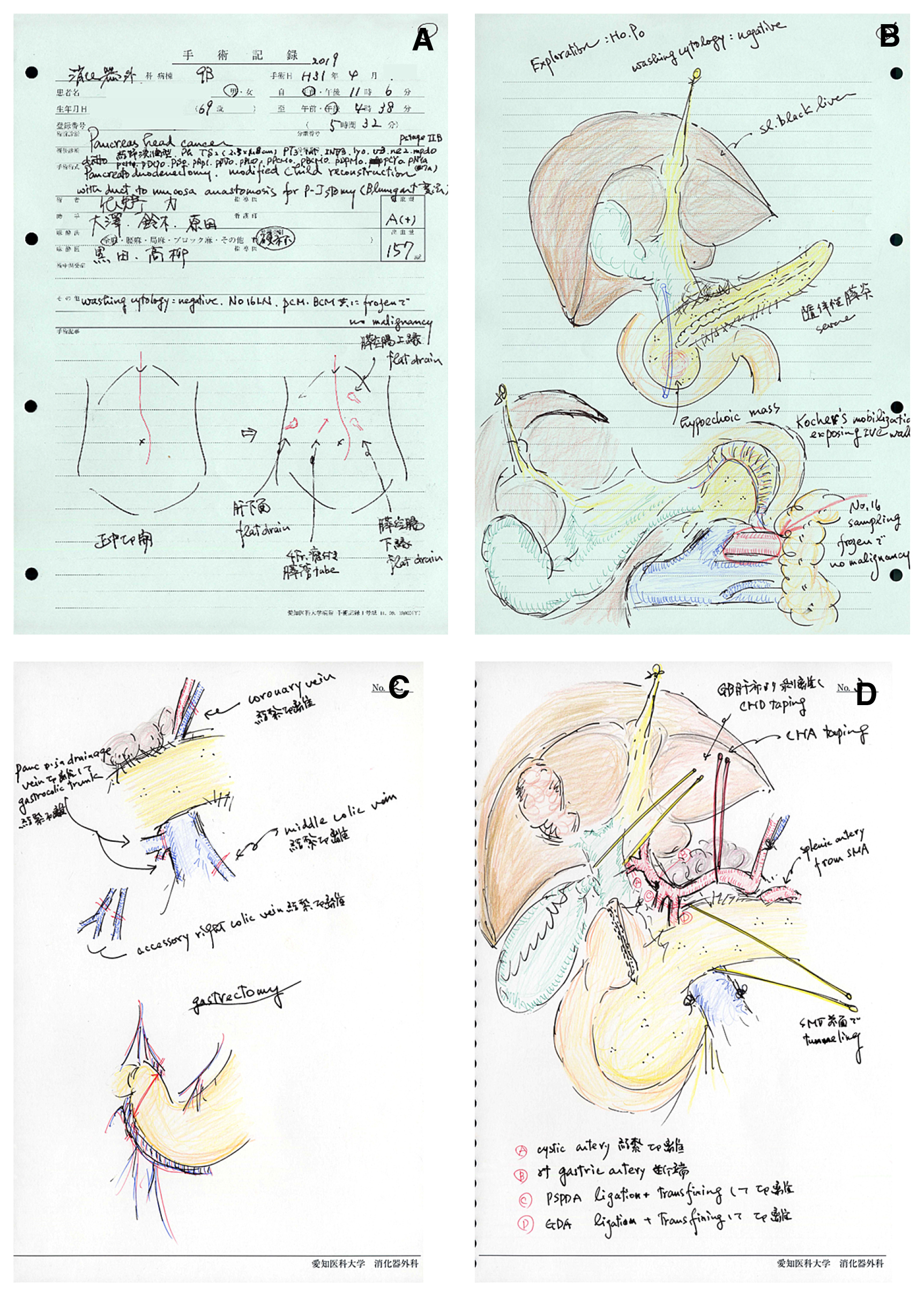
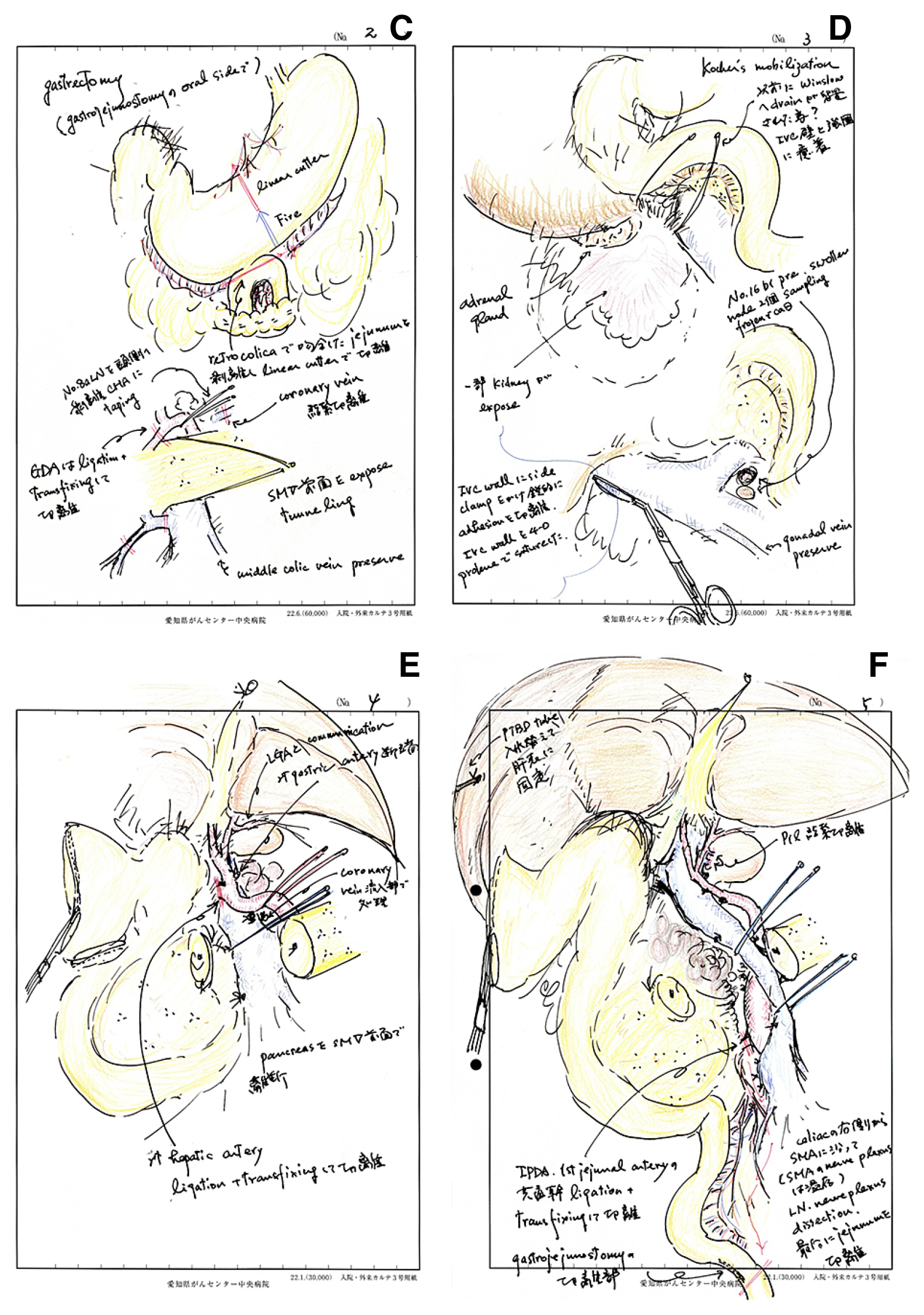
Schematic representations of a series of standard subtotal stomach preserving pancreatoduodenectomy in our recent case. A: Summary of operative details are described. The skin incision and drain positions after abdominal closure are also noted. B: Intraperitoneal findings of the tumor and visceral organs are described. Paraaortic lymph nodes sampling is performed. C: Management of gastrocolic trunk, superior mesenteric exposure, coronary vein division, and gastric transection are illustrated. D: Cholecystectomy, encircling of the common hepatic duct, and division of gastroduodenal and posterior superior pancreatoduodenal arteries are drawn. Common hepatic artery and pancreatic neck are encircled with tape.
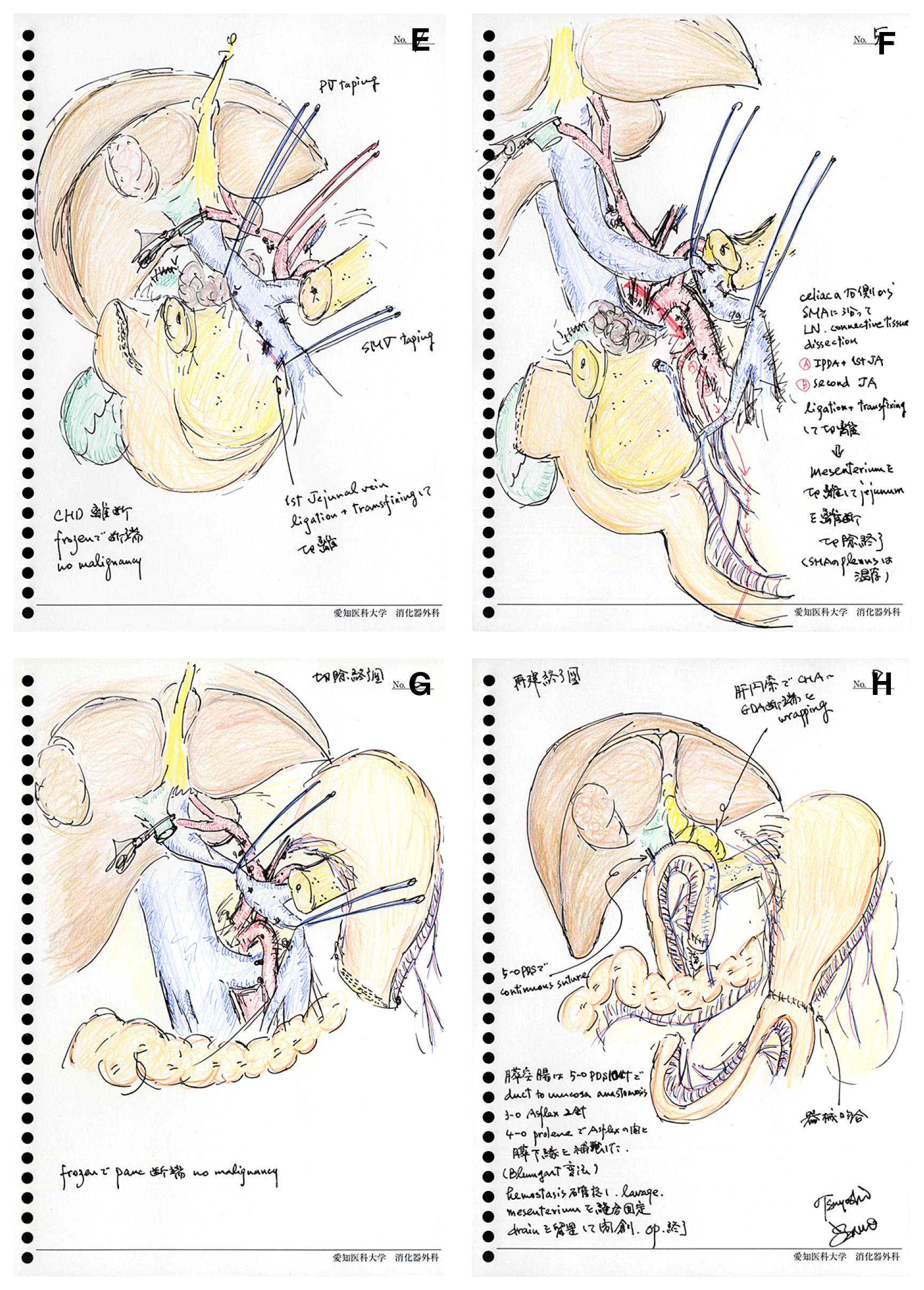
(Continued) E: The pancreatic neck and the common hepatic duct are divided, portal and superior mesenteric veins are encircled with tape. F: The lymph node and connective tissue dissection from the right side celiac axis along the superior mesenteric artery. The inferior pancreatoduodenal and the first jejunal arteries are ligated and divided. Mesenteric division is progressed and finally jejunum is transected. G: Schematic representation of operative field after pancreatoduodenectomy. H: Schematic representation after alimentary reconstruction.
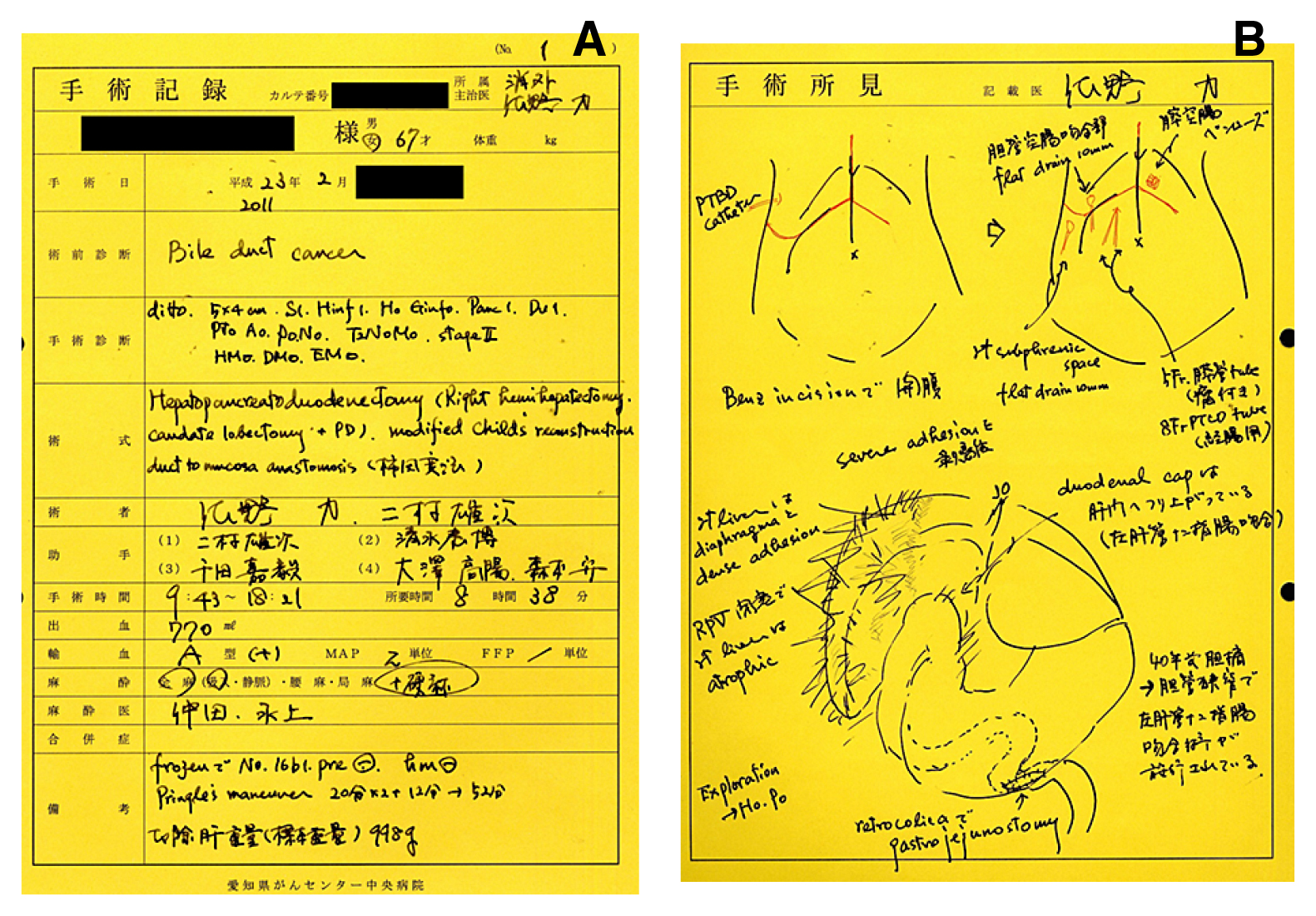
Schematic representations of a series of right hepatopancreatoduodenectomy in a patient surviving more than 5 years without tumor recurrence. A: Summary of operative details are described. B: The skin incision and drain positions after abdominal closure are also noted. Intraperitoneal findings of the tumor and previous surgical procedure are described.
(Continued) C: Gastric division is performed at the oral site of the previous gastrojejunostomy. Management of gastrocolic trunk, superior mesenteric exposure, coronary vein division are illustrated. The common hepatic artery is isolated and gastroduodenal artery is ligated and divided. D: Kocher’s mobilization during severe adhesion and paraaortic lymph nodes sampling is performed. E: The pancreatic neck and the right hepatic artery are divided. F: Portal and superior mesenteric veins are encircled with tape. The lymph node and connective tissue dissection from the right side of celiac axis along the superior mesenteric artery. The common trunk of the inferior pancreatoduodenal and the first jejunal arteries is ligated and divided. Mesenteric division is progressed and the jejunum is transected.
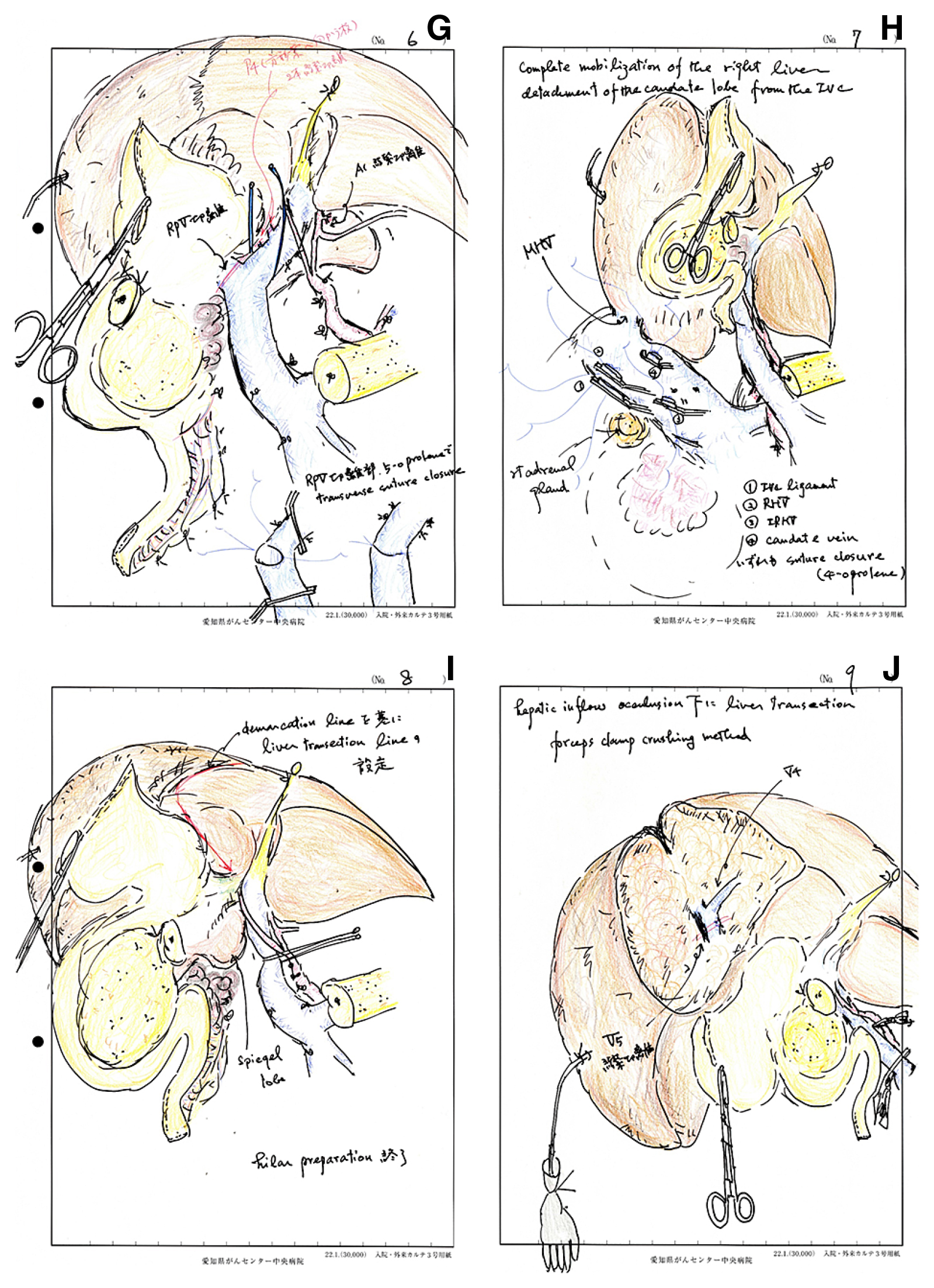
(Continued) G: The right portal vein is divided with suture closure. Skeletonization of the hepatoduodenal ligament is completed. H: The right liver is mobilized and the entire caudate lobe is detached from the inferior vena cava. Thick short hepatic veins and the right hepatic vein are transected with suture closure. I: The liver transection line is traced on the demarcation and the line on the ventral aspect of medial sector keeping from the hilar plate is critical. J: Liver transection is started under intermittent inflow occlusion using forceps clamp crushing method. The middle hepatic vein is exposed on the raw surface.
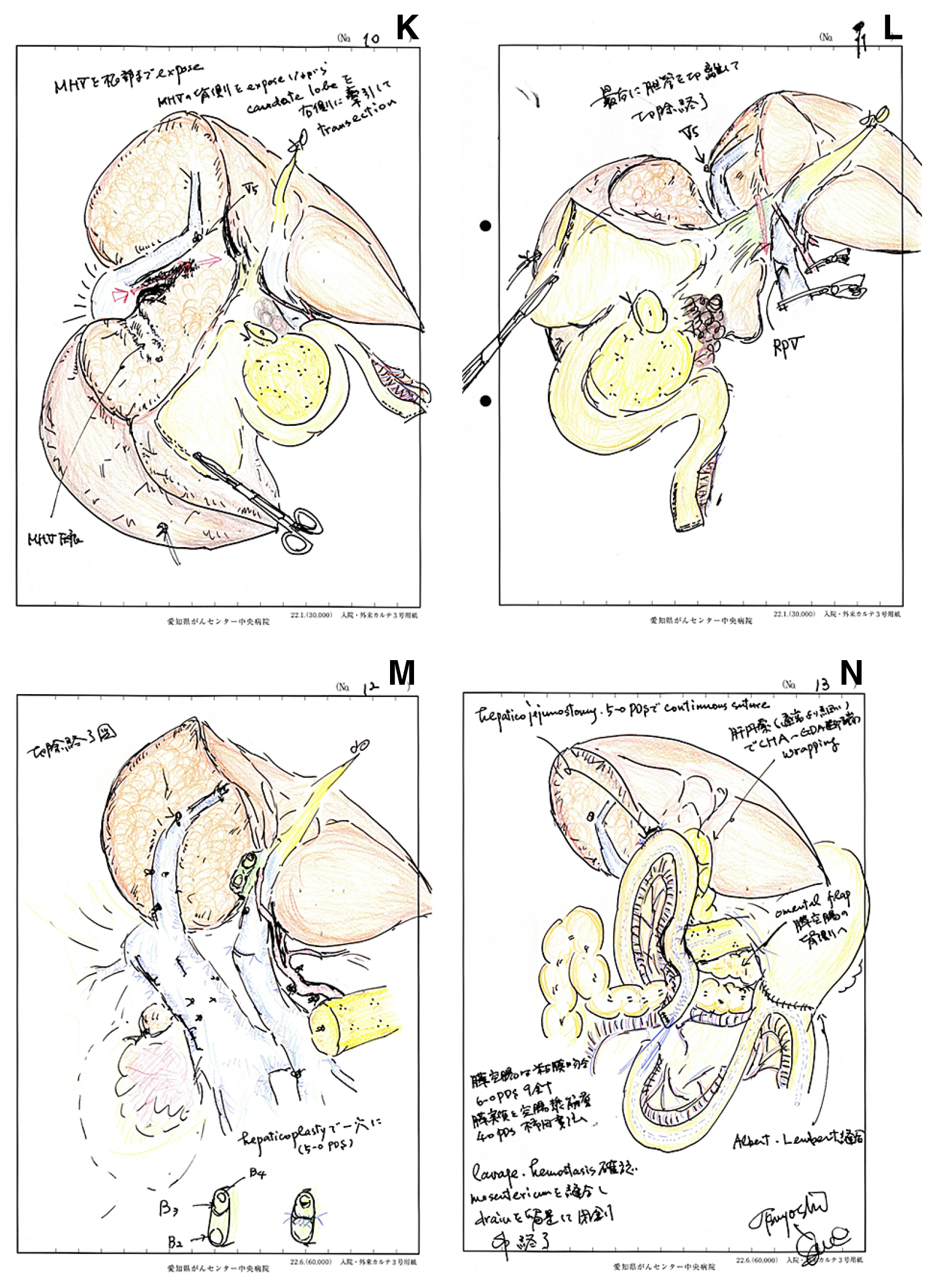
(Continued) K: The dorsal aspect of middle hepatic vein is exposed extracting the caudate lobe to the right side. L: The left hepatic duct is transected as the final resection procedure. M: Schematic representation of operative field after the right hepatopancreatoduodenectomy. N: Schematic representation after alimentary reconstruction.
絵で書く手術記事の趣旨を尊重し,個々の絵の詳細な記述は敢えて割愛する.
膵頭十二指腸切除の手術記事を記載するうえで必要な内容は
1.開腹所見と想定される癌の進展範囲.
2.Kocher授動と傍大動脈リンパ節の取り扱い.
3.膵頭部前面の剥離,上腸間膜静脈の露出.
4.胃(十二指腸)の切離.
5.膵上縁から肝門の剥離,胃十二指腸動脈の処理.
6.胆囊剥離,総胆管処理.
7.膵のトンネリングと膵切離.
8.空腸処理と門脈周囲の郭清,上腸間膜動脈神経叢の取り扱い.
9.切除終了図
10.再建方法.
11.ドレーン留置と閉腹.
の11項目と考えている.
肝膵十二指腸切除術では,膵頭十二指腸切除に加え,下記の項目を追加する必要がある.ただし胆囊・総胆管の処理は行わない.
1.右肝動脈の切離と左・中肝動脈の走行
2.右門脈の切離と左門脈臍部の露出,尾状葉門脈枝の切離
3.肝右葉・尾状葉の授動
4.右肝静脈の切離
5.肝実質の離断,中肝静脈の露出
6.胆管の切離
の6項目を追加する必要がある.
著者が外科研修医時代,上級指導医は自らシェーマを用いて手術記事を難なく書いていた.所属した名古屋大学第一外科(現腫瘍外科)では,教授であっても執刀医が自ら絵で手術記事を書くのが伝統であった.肝胆膵領域腫瘍に対する手術では教授のチェックをパスしなければ手術記事として認められなかった.一方,国立がんセンター(現国立がん研究センター)では外科レジデントが,執刀・前立にかかわらず,手術を勉強するという観点から手術記事を書いていた.前立の側にいながら,どうやって術者側から見た分かりやすいシェーマを書くのかに直面したが,その分手術のことを常に考えており,その後の手術記事作成に役立ったことは間違いない.著者は名古屋大学時代,愛知県がんセンター着任後は現在でも自ら絵で手術記事を書くことを遵守している.
シェーマが描ければ,手術のその局面を理解できている,逆に書けないということは十分理解していない可能性がある.絵の上手下手,得意不得意はあるが,努力を続ければ,分かりやすい,分かってもらえる手術記事が書けるようになると考えている.実際に自分自身の卒後5~6年の手術記事を見直すと,合格の評価は難しい.メディカルイラストレーションの成書を参考にするなどして,書き続けることこそが上達のコツで,まさに継続は力なりであると考えている.
また,手術記事は書きっ放しではなく,指導者・上級医のチェックを受け,質の向上につなげることが肝要である4).エビデンスはないが,手術記事の記載に努力が見られれば,実際の手術手技も向上していくと考える.研修途上の若手外科医には,上級医に手術執刀ならびに指導を受ける機会をもらい,絵を描いて恩返しするつもりで手術記事作成に精進することを望みたい.また,上級医は範を示し,手術記事作成を指導すべきと考える.また,肝胆膵外科学会の高度技能医を取得申請する際には症例の手術ビデオだけではなく,シェーマを用いた手術記事を提出することが求められている.この資格を目指すものは,提出用のみならず常日頃からシェーマを用いた手術記事を書き,質の向上を心掛けるべきである.
諸外国では,外科医が自ら手術記事を書くことが少なく,ましてや自らが作成したイラストを汎用することはまれである.文章の羅列から情報を読み解くのは,時間を要し,不完全になりやすいことから,絵で描く手術記事の重要性については議論の余地はない.いわゆる百聞は一見に如かずといえる.絵を汎用した手術記事は,日本の消化器外科の文化と伝統と考えており,これを踏襲することが現役消化器外科医の務めであろう.
結論:手術記事を絵で書くことは,読み手に理解しやすいだけではなく,書いた術者・作者の理解度を再確認するために必要な作業である.
利益相反:なし