Abstract
症例は45歳の女性で,偶発的に腹部造影CTにて20 mm大の虫垂腫瘤を指摘され,FDG-PET/CTで同部位に異常集積を認めた.下部消化管内視鏡検査では虫垂開口部に隆起性病変を認め,生検を施行したが,腫瘍性変化を認めなかった.画像検査所見から虫垂癌を疑い,腹腔鏡下回盲部切除術を施行した.病理組織学的検査では,病変部に線維化とリンパ球や形質細胞主体の炎症細胞浸潤を認め,IgG4/IgG陽性細胞比は78.3%,IgG4陽性形質細胞数は112/HPFであり,IgG4関連虫垂偽腫瘍が疑われた.しかしながら,本症例では炎症細胞浸潤が巣状にしか認められなかったこと,好中球浸潤や肉芽組織増生を伴っていたこと,高IgG4血症や他臓器病変を認めなかったことがIgG4関連疾患として非典型的であった.本症例のような虫垂病変が真にIgG4関連疾患であるか否かを決定するには類似症例の蓄積によるさらなる解析が必要である.
Translated Abstract
A 45-year-old woman was referred to our department with a diagnosis of appendiceal cancer. Contrast enhanced CT revealed a 20 mm appendiceal mass that showed high FDG accumulation on FDG-PET/CT. Lower gastrointestinal endoscopy demonstrated a protruding lesion in the appendiceal orifice, but no neoplastic changes were found in biopsy specimens. Laparoscopic ileocecal resection was performed. Histopathological examination showed dense fibrosis and lymphoplasmacytic infiltration in the appendiceal mass. The number of IgG4-positive plasma cells was 112/HPF and the IgG4-positive/IgG-positive plasma cell ratio was 78.3%; therefore, IgG4-related inflammatory pseudotumor was suspected. However, there were some atypical points in this case for diagnosis of IgG4-related disease: focal inflammatory cell infiltration, the presence of neutrophilic infiltration and granulation tissue, and the absence of elevated serum IgG4 concentrations and other organ involvement. Further analysis of similar cases is needed to determine if this appendiceal lesion is truly IgG4-related disease.
はじめに
IgG4関連疾患は,リンパ球や形質細胞の著明な浸潤と線維化によって,全身の諸臓器に腫大,腫瘤,結節,肥厚を生じる原因不明の疾患である1).膵臓や胆管や涙腺・唾液腺などに好発し,虫垂に発生することは極めてまれである.今回,我々は虫垂癌との鑑別が困難でありIgG4関連偽腫瘍が疑われた虫垂腫瘤の1例を経験したため,若干の文献的考察を加えて報告する.
症例
患者:45歳,女性
主訴:なし.
既往歴:Wilson病(23歳時に診断され,以降内服加療中)
家族歴:妹がWilson病
現病歴:Wilson病による肝硬変に対するスクリーニング目的で撮像された腹部造影CTで偶発的に虫垂根部に腫瘤を認め,追加で精査を行ったが確定診断に至らなかった.画像検査所見からは虫垂癌が疑われたため,手術目的で当科に紹介となった.
血液検査所見:特記すべき異常を認めなかった.腫瘍マーカー(CEA・CA19-9)の上昇も認めなかった.
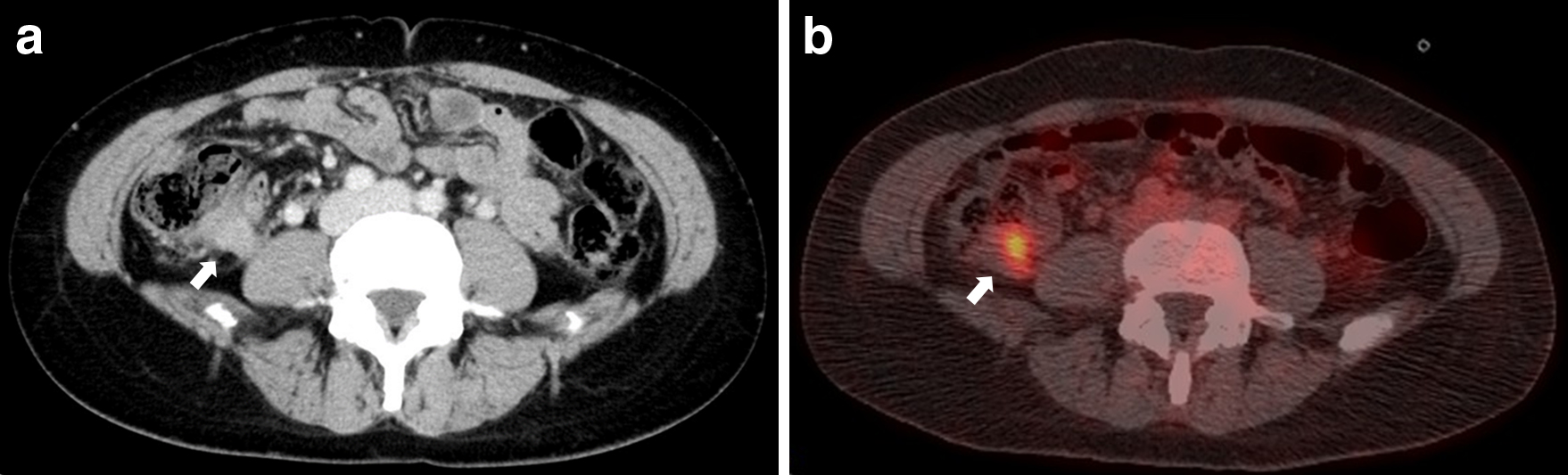
腹部造影CT所見:虫垂根部に造影効果を伴う20 mm大の腫瘤を認めた(Fig. 1a).
FDG-PET/CT所見:虫垂根部の腫瘤にSUVmax=5.39の集積を認めた.その他の部位に明らかな異常集積を認めなかった(Fig. 1b).
下部消化管内視鏡検査所見:虫垂開口部に隆起性病変を認め,生検を施行した(Fig. 2).
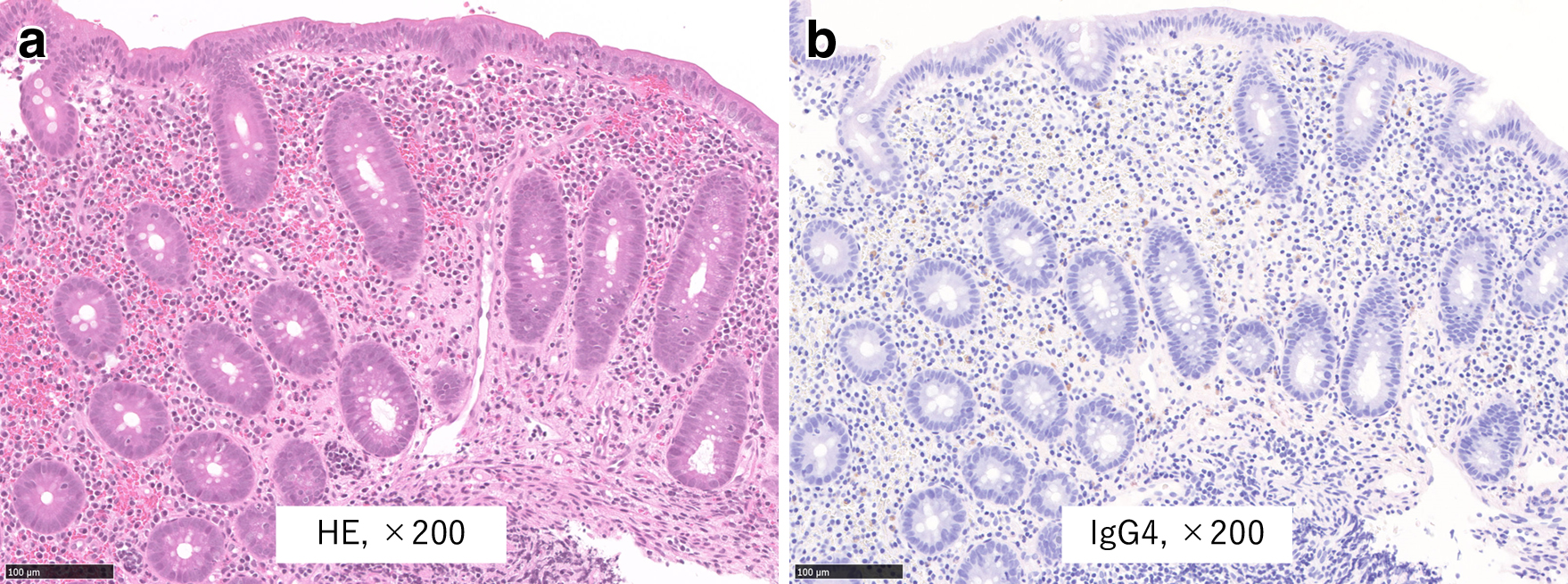
生検所見:形質細胞を含む炎症細胞浸潤を認め,腫瘍性変化を認めなかった.術後に生検組織の免疫染色検査を追加したが,IgG4陽性形質細胞浸潤は指摘されなかった(Fig. 3).
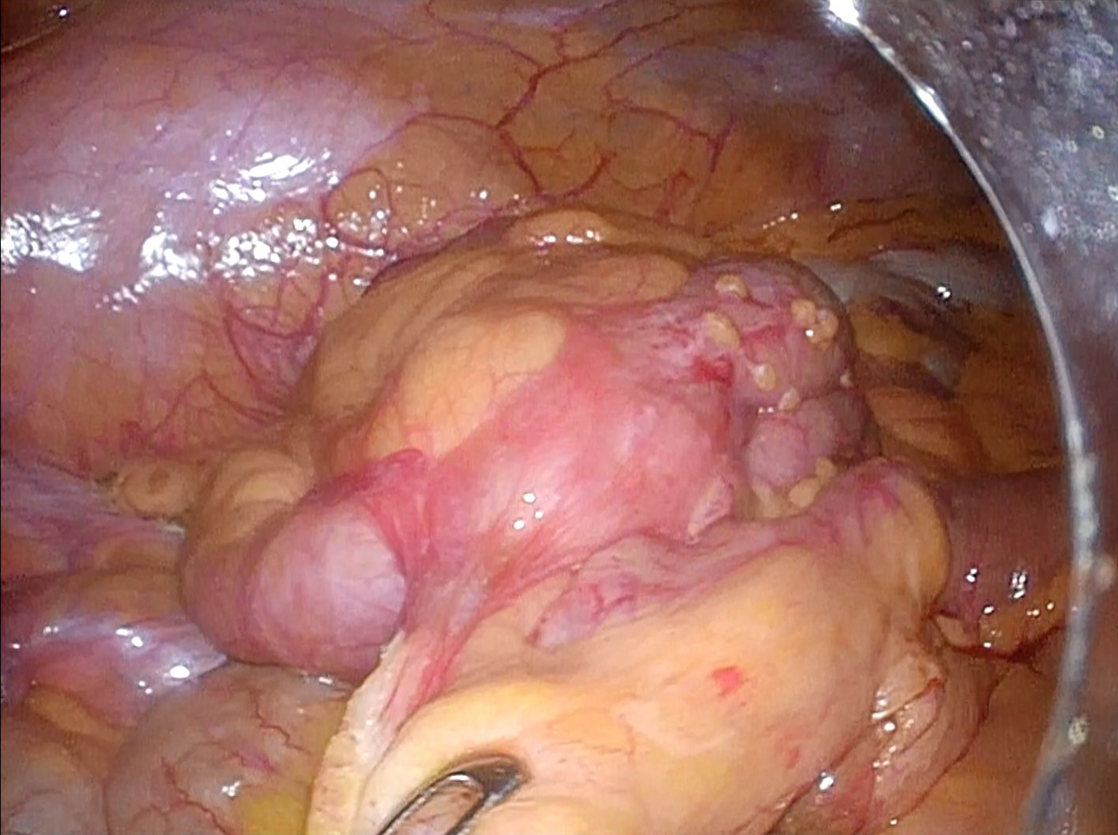
手術所見:病変部の漿膜面に明らかな変化を認めなかったが,虫垂は僅かに腫大していた(Fig. 4).腹腔鏡下回盲部切除術(D2リンパ節郭清)を施行した.手術時間は153分,出血量は15 mlであった.
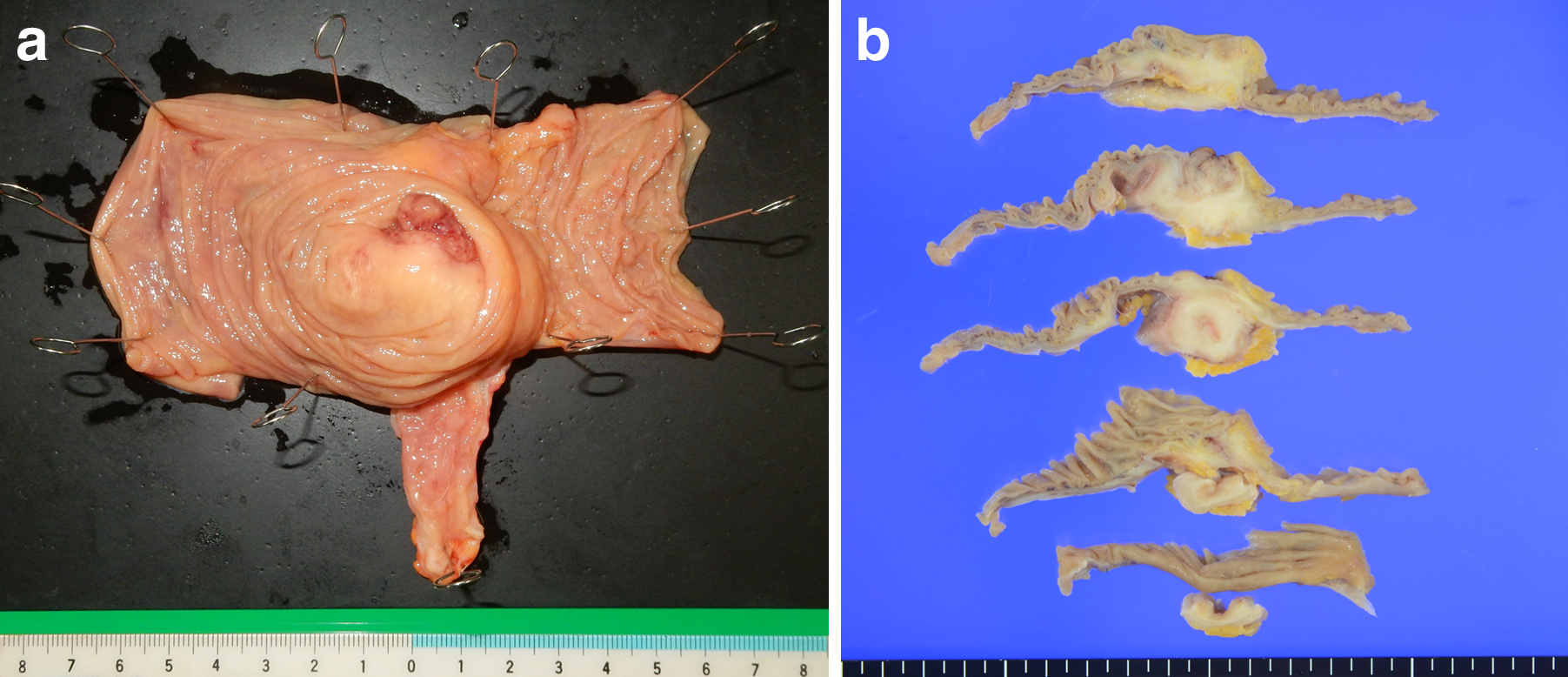
摘出標本肉眼所見:虫垂根部に20 mm大の腫瘍様病変を認めた(Fig. 5).
術後経過:術後経過は良好であり,術後8日目に退院となった.現在,術後2年経過しており,再燃を認めていない.
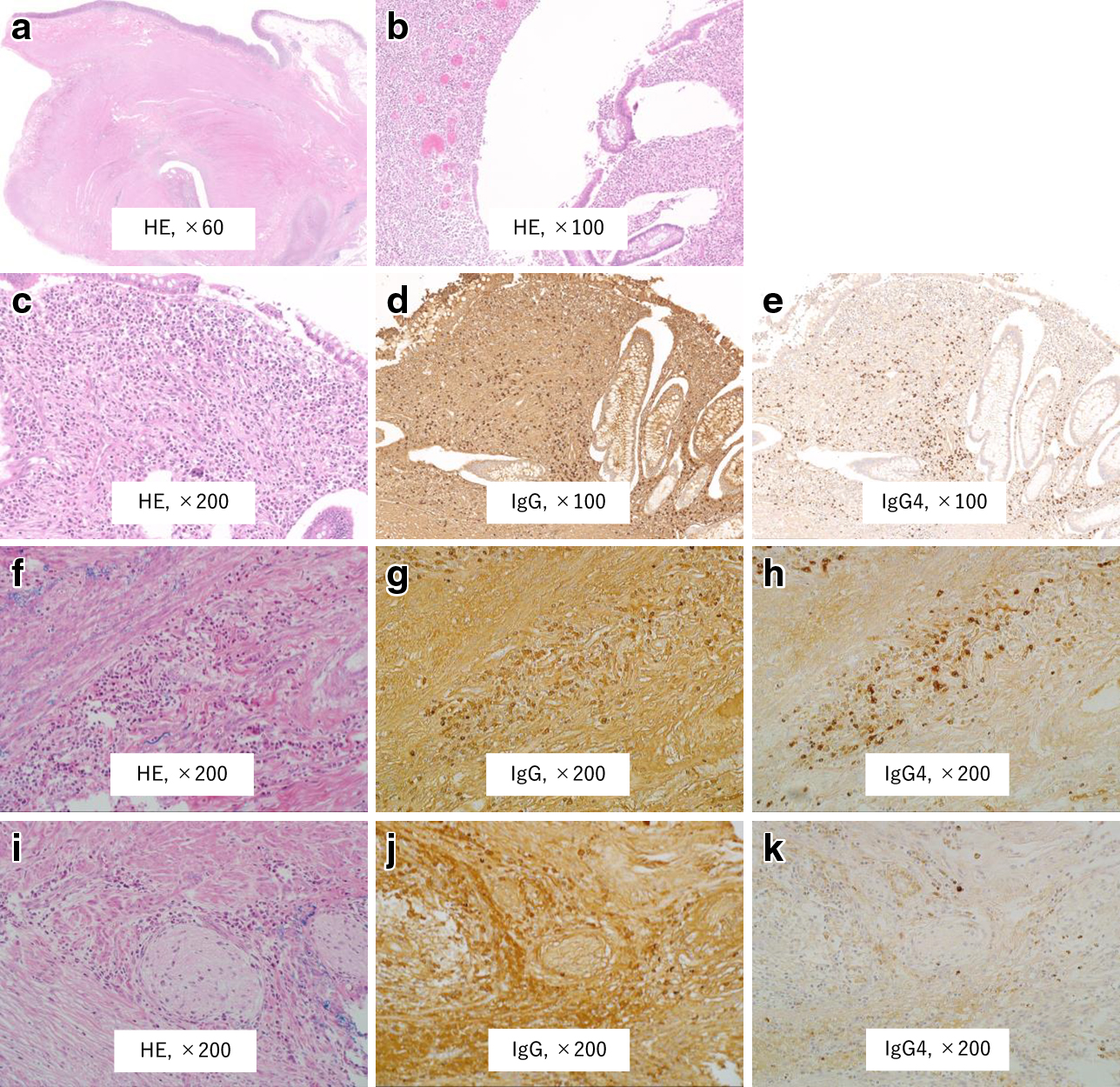
病理組織学的検査所見:虫垂の腫瘤形成部の粘膜固有層,粘膜下層および固有筋層の筋間神経叢・血管周囲に密なリンパ球や形質細胞主体の炎症細胞浸潤を認めた.著明な線維化を伴っており,炎症細胞浸潤は巣状に認められた.IgG4陽性形質細胞浸潤は粘膜固有層から粘膜下層で顕著であり,固有筋層では疎であった.IgG4/IgG陽性細胞比は78.3%であり,IgG4陽性形質細胞数は112/HPF(high-power field)であった.粘膜固有層に微小な花筵状線維化を認めた.閉塞性または非閉塞性静脈炎を認めなかった.好酸球の浸潤を認めた.好中球の浸潤や肉芽組織の増生を認め,陰窩は消失していた.形質細胞による陰窩の破壊は明らかでなかった.郭清したリンパ節を含め,悪性所見を認めなかった(Fig. 6).
考察
IgG4関連疾患は,リンパ球や形質細胞の著明な浸潤と線維化によって,同時性あるいは異時性に全身の諸臓器にびまん性あるいは限局性の腫大,腫瘤,結節,肥厚を生じる疾患であり,いまだに原因は不明であるが,免疫遺伝学的背景に基づいた異常な免疫学的機序が関連していると考えられている1).病理組織学的には,著明なリンパ球・形質細胞浸潤,花筵状線維化,閉塞性静脈炎が特徴的であり(花筵状線維化や閉塞性静脈炎は罹患臓器によって認められない場合もある),その他の特徴として非閉塞性静脈炎や好酸球浸潤を認めることもある2).また,膵臓や胆管や涙腺・唾液腺などに好発し,消化管に発生することはまれである.Koizumiら3)は,自己免疫性膵炎患者の中には,腫瘤形成や線維化や閉塞性静脈炎を伴わず,胃や結腸の粘膜や十二指腸乳頭にIgG4陽性形質細胞の浸潤を認めることがあるが,これらはIgG4関連消化管疾患とは診断できず,IgG4関連消化管疾患の診断には,臨床所見として腫瘤形成を認め,且つ,病理組織学的検査所見として線維化を伴う著明なIgG4陽性形質細胞浸潤を認めることが必須であるとしている.さらに,IgG4関連消化管疾患には,食道や胃に著しい壁肥厚を生じるものと,胃や結腸や十二指腸乳頭にポリープ様または腫瘍様病変を生じるものがあるとしている.PubMed(1950年~2019年4月)で「IgG4 related disease」,「esophagus,stomach,duodenum,small intestine,colon,rectum」をキーワードとして検索し,それらの参考文献も含めて検討したところ,IgG4関連消化管疾患の臓器別の報告症例数は,食道が14例4)~10),胃が27例7)11)~33),十二指腸が3例34)~36),小腸が3例37)~39),結腸が6例14)40)~43),直腸が1例44)であり(Table 1),胃が最も多く,次に食道,結腸の順に多かった.
Table 1
Reported cases of IgG4-related gastrointestinal disease
|
n |
| esophagus |
14 |
| stomach |
27 |
| duodenum |
3 |
| small intestine |
3 |
| colon |
6 |
| rectum |
1 |
| appendix |
4 |
虫垂に発生することは極めてまれであり,医学中央雑誌(1964年~2019年4月)およびPubMed(1950年~2019年4月)で「IgG4関連疾患」,「虫垂」,「IgG4 related disease」,「appendix」をキーワードとして検索したところ(会議録除く),過去の報告例は4例のみであり45)~48),本邦での報告はなかった(Table 2).臨床症状は罹患臓器によって異なるが,虫垂に発生した過去の報告例4例では腹痛を認めた.CT所見としては,2例で虫垂に腫瘤形成を認め,1例では内腔に液貯留を伴った虫垂の腫大および壁肥厚を認めた.自験例では,FDG-PET/CTにて虫垂腫瘤に異常集積を認めたことで虫垂癌がより強く疑われたが,IgG4関連疾患でも疾患活動性の高い部位に異常集積を認めることが知られており,罹患臓器の全身検索やステロイド治療後の効果判定に有用であるとされている49).
Table 2
Reported cases of IgG4-related appendiceal lesions
| No. |
Author/Year |
Age/Sex |
Symptom |
CT appearance of appendiceal lesion |
Treatment |
Serum IgG4 |
Histopathological findings |
Other IgG4-RD |
| Lymphoplasmacytic infiltration |
Storiform fibrosis |
Obliterative phlebitis |
IgG4+/IgG+ratio |
Number of IgG4+ plasma cells |
| 1 |
Comtesse45)/2014 |
20/F |
abdominal pain |
N/A |
appendectomy |
N/A |
+ |
N/A |
+ |
>40% |
N/A |
none |
| 2 |
Kim46)/2016 |
51/M |
right lower quadrant abdominal pain |
mass forming |
right hemicolectomy |
N/A |
+ |
− |
− |
>50% |
N/A |
none |
| 3 |
Veerankutty47)/2018 |
57/M |
right lower quadrant abdominal pain |
swelling and wall thickening with intraluminal fluid |
right hemicolectomy |
N/A |
+ |
+ |
− |
41.66% |
100/HPF |
none |
| 4 |
Kwon48)/2019 |
46/F |
right lower quadrant abdominal pain |
mass forming |
right hemicolectomy |
N/A |
+ |
+ |
+ |
>50% |
>100/HPF |
none |
| 5 |
Our case |
43/F |
none |
mass forming |
ileocecal resection |
6 mg/dl* |
+ |
+ |
− |
78.30% |
112/HPF |
none |
N/A: not available, IgG4-RD: IgG4-related disease, *Measured postoperatively
IgG4関連疾患の診断には,「IgG4関連疾患包括診断基準2011」50)が用いられ,「1)臨床的に単一または複数臓器に特徴的なびまん性あるいは限局性腫大,腫瘤,結節,肥厚性病変を認める,2)血液学的に高IgG4血症(135 mg/dl以上)を認める,3)病理学的に以下の二つを認める(①著明なリンパ球,形質細胞の浸潤と線維化を認める,②IgG4/IgG陽性細胞比40%以上,且つIgG4陽性形質細胞が10/HPFを超える)」の3項目が挙げられている.自験例では術前に血清IgG4値の測定を行っておらず,術後7日目に血清IgG4値を測定したところ,6 mg/dlであり上昇を認めなかったが,前述の診断基準の1)+3)を満たしていた.しかしながら,病理組織学的検査所見において,リンパ球・形質細胞浸潤が“びまん性”でなく“巣状”であったことや,好中球浸潤や肉芽組織増生を認めたことがIgG4関連疾患として非典型的であった.また,虫垂の粘膜固有層内に多数のIgG4陽性細胞を認めたことについては,通常でも同部位にリンパ装置を認めることはありえるが,背景の盲腸の粘膜固有層内のリンパ装置にはIgG4陽性細胞を認めないことから,虫垂病変と一連の変化である可能性が疑われた.IgG4陽性形質細胞数とIgG4/IgG陽性細胞比の計測は,Consensus statement2)に推奨されているように,IgG4陽性形質細胞を最も多く認める3箇所で計測し,その平均値を求めた.好酸球浸潤はIgG4関連疾患の診断において感度・特異度ともに高くはないが2),支持的な所見であった.さらに,IgG4陽性形質細胞を多数認める可能性がある鑑別すべき非IgG4関連疾患として,炎症性腸疾患や悪性リンパ腫や癌が考えられたが,病歴や検査所見からこれらは否定的であった.本症例では,高IgG4血症を認めず,病理組織学的検査で非典型的な所見を含んでいたため,確定診断はできなかったが,IgG4関連疾患に類似する複数の所見と非IgG4関連疾患の鑑別をもとに,IgG4関連虫垂偽腫瘍が疑われた.
IgG4関連疾患に対する治療としては,ステロイド治療が標準的であるが,その治療効果は罹患臓器や線維化の程度によって異なる51).IgG4関連虫垂病変に対するステロイド治療の有効性については,過去の報告例4例全てで外科的治療が行われているため不明であるが,他の臓器と同様にステロイド治療が有効である可能性があり,術前に確定診断が得られれば,不要な手術を回避することができるかもしれない.そのためには,生検にて腫瘍性変化を認めず,リンパ球や形質細胞の浸潤を伴う虫垂腫瘤を認める症例においては,鑑別疾患としてIgG4関連疾患を考慮し,血清IgG4値の測定や生検組織の免疫染色検査を追加することが望まれる.診断目的でのステロイド投与については,他のIgG4関連疾患と同様に慎重に判断するべきである.
最後に,IgG4関連虫垂病変についてはいまだ一定の見解がなく,本症例のようにIgG4陽性形質細胞浸潤と線維化を伴う腫瘤形成を認めるものの,前述のようなIgG4関連疾患としては非典型的な病理組織学的検査所見を有し,高IgG4血症や他臓器病変を伴わない虫垂病変が真にIgG4関連疾患であるか否かを決定するには,類似症例の蓄積によるさらなる解析が必要である.
利益相反:なし
文献
- 1) Okazaki K, Umehara H. Current concept of IgG4-related disease. Curr Top Microbiol Immunol. 2017;401:1–17.
- 2) Deshpande V, Zen Y, Chan JK, Yi EE, Sato Y, Yoshino T, et al. Consensus statement on the pathology of IgG4-related disease. Mod Pathol. 2012;25:1181–1192.
- 3) Koizumi S, Kamisawa T, Kuruma S, Tabata T, Chiba K, Iwasaki S, et al. Immunoglobulin G4-related gastrointestinal diseases, are they immunoglobulin G4-related diseases? World J Gastroenterol. 2013;19(35):5769–5774.
- 4) Lopes J, Hochwald SN, Lancia N, Dixon LR, Ben-David K. Autoimmune esophagitis: IgG4-related tumors of the esophagus. J Gastrointest Surg. 2010;14(6):1031–1034.
- 5) Lee H, Joo M, Song TJ, Chang SH, Kim H, Kim YS, et al. IgG4-related sclerosing esophagitis: a case report. Gastrointest Endosc. 2011;73(4):834–837.
- 6) Dumas-Campagna M, Bouchard S, Soucy G, Bouin M. IgG4-related esophageal disease presenting as esophagitis dissecans superficialis with chronic strictures. J Clin Med Res. 2014;6(4):295–298.
- 7) Yang L, Jin P, Sheng JQ. Immunogloblin G4-related disease (IgG4-RD) affecting the esophagus, stomach, and liver. Endoscopy. 2015;47:96–97.
- 8) Oh JH, Lee TH, Kim HS, Jung CS, Lee JS, Hong SJ, et al. Esophageal involvement of immunoglobulin G4-related disease: a case report and literature review. Medicine (Baltimore). 2015;94(50):1–4.
- 9) Obiorah I, Hussain A, Palese C, Azumi N, Benjamin S, Ozdemirli M. IgG4-related disease involving the esophagus: a clinicopathological study. Dis Esophagus. 2017;30(12):1–7.
- 10) Mori S, Tahashi Y, Uchida K, Ikeura T, Danbara N, Wakamatsu T, et al. Sclerosing esophagitis with IgG4-positive plasma cell infiltration. Intern Med. 2017;56(22):3023–3026.
- 11) Fujita T, Ando T, Sakakibara M, Hosoda W, Goto H. Refractory gastric ulcer with abundant IgG4-positive plasma cell infiltration: a case report. World J Gastroenterol. 2010;16(17):2183–2186.
- 12) Baez JC, Hamilton MJ, Bellizzi A, Mortelé KJ. Gastric involvement in autoimmune pancreatitis: MDCT and histopathologic features. JOP. 2010;11(6):610–613.
- 13) Kaji R, Okabe Y, Ishida Y, Takedatsu H, Kawahara A, Aino H, et al. Autoimmune pancreatitis presenting with IgG4-positive multiple gastric polyps. Gastrointest Endosc. 2010;71(2):420–422.
- 14) Chetty R, Serra S, Gauchotte G, Märkl B, Agaimy A. Sclerosing nodular lesions of the gastrointestinal tract containing large numbers of IgG4 plasma cells. Pathology. 2011;43(1):31–35.
- 15) Rollins KE, Mehta SP, O’Donovan M, Safranek PM. Gastric IgG4-related autoimmune fibrosclerosing pseudotumour: a novel location. ISRN Gastroenterol. 2011;2011:873087.
- 16) Na KY, Sung JY, Jang JY, Lim SJ, Kim GY, Kim YW. Gastric nodular lesion caused by IgG4-related disease. Pathol Int. 2012;62(10):716–718.
- 17) Bateman AC, Sommerlad M, Underwood TJ. Chronic gastric ulceration: a novel manifestation of IgG4-related disease? J Clin Pathol. 2012;65(6):569–570.
- 18) Kim DH, Kim J, Park DH, Lee JH, Choi KD, Lee GH, et al. Immunoglobulin G4-related inflammatory pseudotumor of the stomach. Gastrointest Endosc. 2012;76(2):451–452.
- 19) Frydman J, Grunner S, Kluger Y. IgG4-related disease manifestating as an acute gastric-pericardial fistula. World J Gastroenterol. 2014;20(44):16782–16785.
- 20) Inoue K, Okubo T, Kato T, Shimamura K, Sugita T, Kubota M, et al. IgG4-related stomach muscle lesion with a renal pseudotumor and multiple renal rim-like lesions: a rare manifestation of IgG4-related disease. Mod Rheumatol. 2018;28(1):188–192.
- 21) Woo CG, Yook JH, Kim AY, Kim J. IgG4-related disease presented as a mural mass in the stomach. J Pathol Transl Med. 2016;50(1):67–70.
- 22) Zhang H, Jin Z, Ding S. Gastric calcifying fibrous tumor: a case of suspected immunoglobulin G4-related gastric disease. Saudi J Gastroenterol. 2015;21(6):423–426.
- 23) Kawano H, Ishii A, Kimura T, Takahashi T, Hironaka H, Kawano M, et al. IgG4-related disease manifesting the gastric wall thickening. Pathol Int. 2016;66(1):23–28.
- 24) Cheong HR, Lee BE, Song GA, Kim GH, An SG, Lim W. Immunoglobulin G4-related inflammatory pseudotumor presenting as a solitary mass in the stomach. Clin Endosc. 2016;49(2):197–201.
- 25) Otsuka R, Kano M, Hayashi H, Hanari N, Gunji H, Hayano K, et al. Probable IgG4-related sclerosing disease presenting as a gastric submucosal tumor with an intense tracer uptake on PET/CT: a case report. Surg Case Rep. 2016;2(1):33.
- 26) Bulanov D, Arabadzhieva E, Bonev S, Yonkov A, Kyoseva D, Dikov T, et al. A rare case of IgG4-related disease: a gastric mass, associated with regional lymphadenopathy. BMC Surg. 2016;16(1):37.
- 27) Inoue D, Yoneda N, Yoshida K, Nuka H, Kinoshita J, Fushida S, et al. Imaging and pathological features of gastric lesion of immunoglobulin G4-related disease: a case report and review of the recent literature. Mod Rheumatol. 2019;29(2):377–382.
- 28) Mine S, Ozawa E, Ohnita K, Abe K, Nakao K. A case of IgG4-related disease presenting with multiple gastric submucosal tumors. Gastrointest Endosc. 2018;87(2):608–610.
- 29) Seo HS, Jung YJ, Park CH, Song KY, Jung ES. IgG4-related disease in the stomach which was confused with gastrointestinal stromal tumor (GIST): two case reports and review of the literature. J Gastric Cancer. 2018;18(1):99–107.
- 30) Bohlok A, Khoury ME, Tulelli B, Verset L, Zaarour A, Demetter P, et al. A rare presentation of IgG4 related disease as a gastric antral lesion: case report and review of the literature. Int J Surg Case Rep. 2018;51:244–247.
- 31) Skorus U, Kenig J, Mastalerz K. IgG4-related disease manifesting as an isolated gastric lesion—a literature review. Pol Przegl Chir. 2018;90(4):41–45.
- 32) Lim DY, Cheng LT, Tan DMY, Al Jajeh I. Isolated IgG4-related gastric disease presenting as diffuse gastric wall thickening with ulcer. J Radiol Case Rep. 2018;12(9):9–20.
- 33) Berger Z, Lea-Plaza Puig MI, Varela C, Becerra M, Capetillo M, Vargas J. IgG4 related hypertrophic gastropathy. Report of one case. Rev Med Chil. 2019;147(1):119–124.
- 34) Hisa T, Ohkubo H, Shiozawa S, Ishigame H, Furutake M, Takamatsu M. Lymphoplasmacytic granuloma localized to the ampulla of Vater: an ampullary lesion of IgG4-related systemic disease? Gastrointest Endosc. 2008;68(6):1229–1232.
- 35) Matsunaga K, Hayashi R, Otsuka T, Kaida D, Ueda N, Kosaka T, et al. A case of IgG4-related disease complicated by duodenal bulbitis with IgG4-positive plasma cell infiltration. Endoscopy. 2014;46:E408–410.
- 36) Deng X, Fang R, Zhang J, Li R. Multivisceral IgG4-related disease presenting as recurrent massive gastrointestinal bleeding: a case report and literature review. BMC Gastroenterol. 2018;18(1):136.
- 37) Joo M, Chang SH, Kim H, Gardner JM, Ro JY. Primary gastrointestinal clear cell sarcoma: report of 2 cases, one case associated with IgG4-related sclerosing disease, a review of literature. Ann Diagn Pathol. 2009;13(1):30–35.
- 38) Wong DD, Pillai SR, Kumarasinghe MP, McGettigan B, Thin LW, Segarajasingam DS, et al. IgG4-related sclerosing disease of the small bowel presenting as necrotizing mesenteric arteritis and solitary jejunal ulcer. Am J Surg Pathol. 2012;36(6):929–934.
- 39) Ko Y, Woo JY, Kim JW, Hong HS, Yang I, Lee Y, et al. An immunoglobulin G4-related sclerosing disease of the small bowel: CT and small bowel series findings. Korean J Radiol. 2013;14(5):776–780.
- 40) Ueno K, Watanabe T, Kawata Y, Gotoh T, Tsuji Y, Ida H, et al. IgG4-related autoimmune pancreatitis involving the colonic mucosa. Eur J Gastroenterol Hepatol. 2008;20(11):1118–1121.
- 41) Hiyoshi Y, Oki E, Zaitsu Y, Ando K, Ito S, Saeki H, et al. IgG4-related disease of ileocecal region mimicking malignancy: a case report. Int J Surg Case Rep. 2014;5(10):669–672.
- 42) Malik SM, Raina A, Hartman DJ. Immunoglobulin G4-related pseudotumor presenting as metastatic colon cancer. Clin Gastroenterol Hepatol. 2015;13(1):e1–2.
- 43) Yorita K, Iwamura S. Can colonic inflammatory polyp with numerous immunoglobulin G4-positive plasma cells represent a colonic manifestation of immunoglobulin G4-related disease? A case report. Clin J Gastroenterol. 2019;12(5):398–402.
- 44) Choi SB, Lim CH, Cha MG, Kang WK. IgG4-related disease of the rectum. Ann Surg Treat Res. 2016;90(5):292–295.
- 45) Comtesse S, Friemel J, Fankhauser R, Weber A. Enterocolic lymphocytic phlebitis of the cecal pole and appendix vermiformis with increase of IgG4-positive plasma cells. Virchows Arch. 2014;464(1):113–116.
- 46) Kim HS, Kang WK, Chung DJ. Appendiceal immunoglobulin G4-related disease mimicking appendiceal tumor or appendicitis: a case report. Korean J Radiol. 2016;17(1):56–58.
- 47) Veerankutty FH, Saleem S, Chacko S, Sreekumar VI, Krishnan P, Varma D, et al. IgG4-related disease of the appendix. J Gastrointest Surg. 2018;22:1124–1126.
- 48) Kwon DH, Kallakury B, DeBrito P, Azumi N. IgG4-related appendiceal disease: a first case report fulfilling all pathological diagnostic criteria and with concomitant S100-positive dendritic/schwann cell hyperplasia. Int J Surg Pathol. 2019;27(5):541–546.
- 49) Nakatani K, Nakamoto Y, Togashi K. Utility of FDG PET/CT in IgG4-related systemic disease. Clin Radiol. 2012;67(4):297–305.
- 50) Umehara H, Okazaki K, Masaki Y, Kawano M, Yamamoto M, Saeki T, et al. Comprehensive diagnostic criteria for IgG4-related disease (IgG4-RD), 2011. Mod Rheumatol. 2012;22(1):21–30.
- 51) Kamisawa T, Zen Y, Pillai S, Stone JH. IgG4-related disease. Lancet. 2015;385:1460–1471.