A 71-year-old man was admitted to our hospital complaining of nausea and waterly diarrhea. Physical examination on admission showed low grade fever, lower abdominal pain and increasing bowel sound. Laboratory data on admission showed leukocytosis (21,700/mm3) and hypoproteinemia (4.3g/dl) . Occult blood of stool was positive, but stool culture showed no significant bacteria.
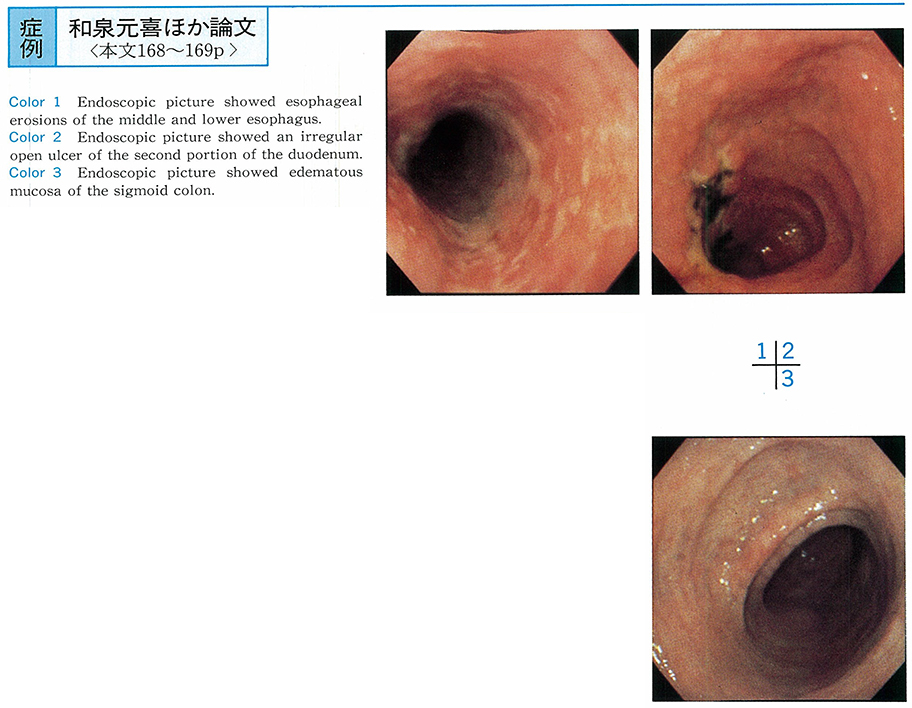
Esophagogastroduodenoscopy showed erosions from middle to lower esophagus, edematous mucosa of the 1st and 2nd portion of duodenum and irregular open ulcers coated with white fur on the 2nd portion of the duodenum. But gastric mucosa was normal. Colonoscopy showed endematous and reddened mucosa of Bauhin's valve, sigmoid colon and rectum, but no abnormal findings were recognized from ascending to descending colon. Histological examination of biopsy specimens of these lesions showed only infiltration of inflammatory cells in the mucosal layer and fibrosis in the submucosal layer, but no granuloma was found.
We suspected Crohn's disease because of endoscopic findings and clinical course, and so prednisolone 30 mg/day and salazosulfapyridine 3 g/day were given, clinical course and endoscopic findings were improved. But pathologically diagnostic creteria for Crohn's disease were not satisfied and considering of his age, ischemic change was most suspected. So careful follow-up of his clinical course and repeated endoscopic examination are important for establishment of the diagnosis.