The patient, a-57-year-old female who had a history of cholecystitis about 25 years before, was seen in our hospital with a chief complaint of right hypochondralgia in September 1994.
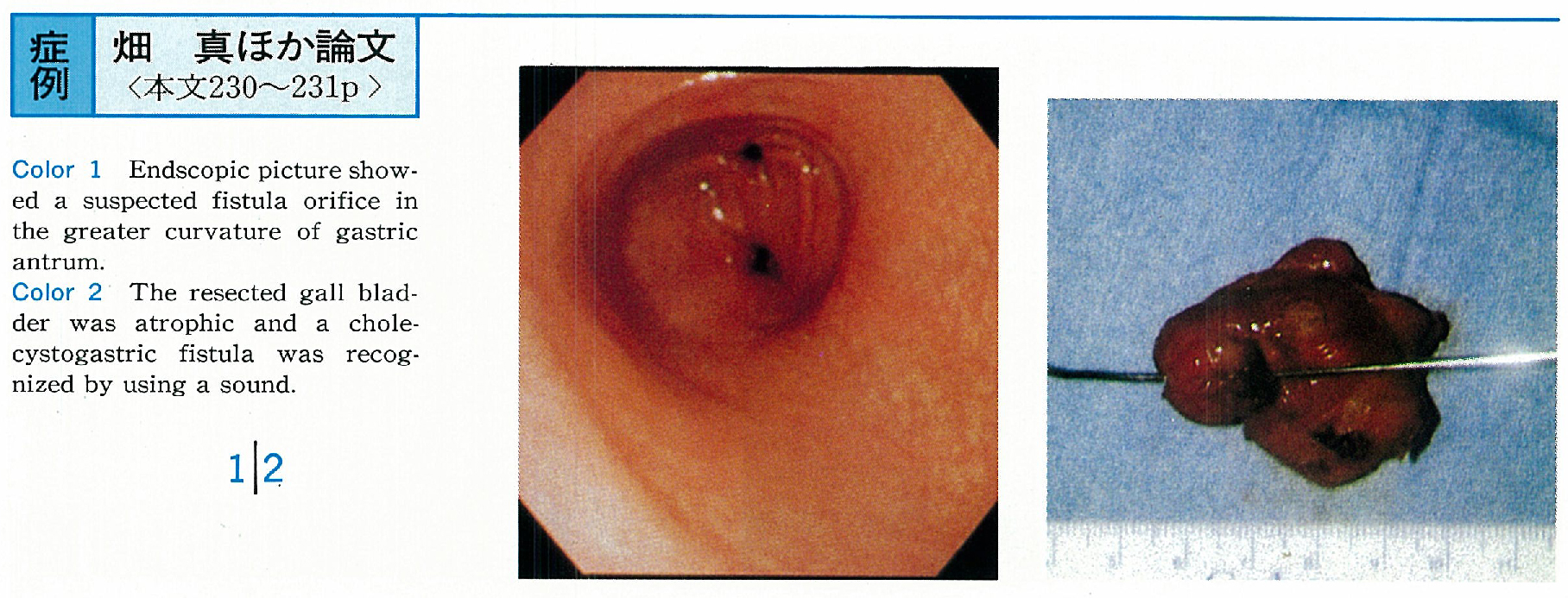
Abdominal plain X-ray revealed pneumobilia and she was admitted with a diagnosis of enterobiliary fistula. Pneumobilia and atrophic gall bladder were detected by CT and Ultrasonography. The orifice, which was considered to be a cholecystogastric fistula, was found in the antrum of the stomach by gastroendoscopy, but the fistula wasn't clearly visualized although endoscopic fistulography was tried. The fistula wasn't visualized by endoscopic retrograde cholangiography (ERC) and percutaneus transhepatic cholangiography (PTC) .
Surgical operation was performed with a diagnosis of cholecystitis, cholangitis and enterobiliary fistula. During the operation, the gall bladder was remarkablly contracted and adhered to the antrum of the stomach with a fistula formation. Cholecystectomy and closure of the fistula was performed. The cholecystogastric fistula was recognized by using a sound. Histologically, chronic cholecystitis pattern was demonstrated. It has been well known that cholecystogastric fistula is rare among the sponstaneous internal biliary fistulae.
We found 38 cases in the Japanese literature. Surgical therapy at an early stage is recommended even for asymptomatic patients in principle.