抄録
A 50-year-old male with diabetes melitus and chronic pancreatitis complained of left hypochondralgia. He continued to have high fever and CRP value on laboratory studies. Gastroendoscopy showed a small protusion on the mucosal surface of the gastric corpus. Abdominal US revealed cystic mass lesion with internal debris in the upper abdomen. Abdominal CT scan revealed unilobular cystic mass located just adjacent to the posterior wall of the stomach. ERCP disclosed that the cystic lumen of this tumor was communicating with pancreatic duct.
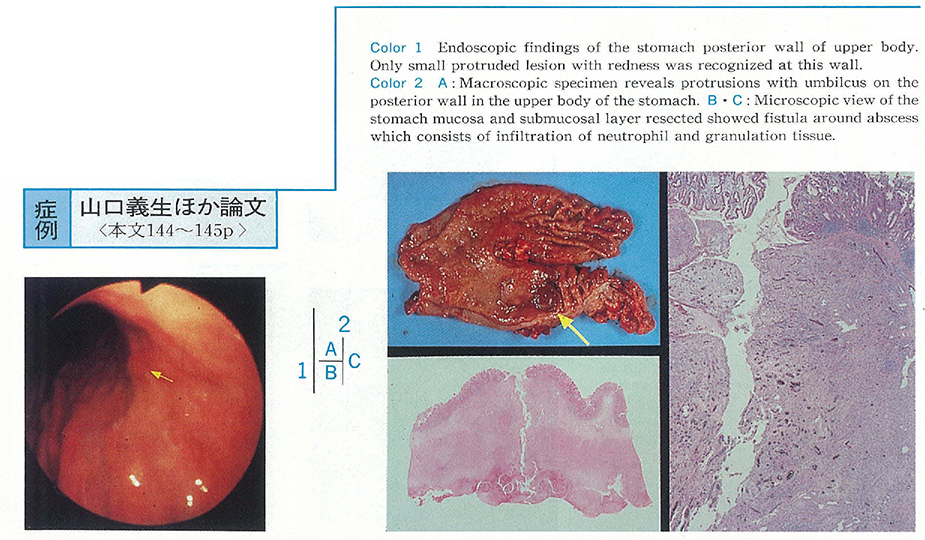
At surgery, a large cystic mass was noted to locate between stomach and pancreas and closely attached to the stomach wall. Cut surface of the stomach wall demonstrated a narrow fistula that penetrating the whole thickness of the stomach wall. Histologically, the cystic mass proved to be a chronic active abscess involving subserosal layer of the stomach.
Our patient had suffered from repeated pancreatitis, diabetes mellitus and habitual alchol intake, and an abdominal mass had developed subsequently, all of these evidences were retospectively suggestive of pancreatic pseudocyst with secondary abscess. In this case, fistulization into the stomach failed to serve as an adequate drainage because of such a complicated pattern of fistulization as likely to be termed“pancreatic duct-infected pseudocyst-stomach”fistulae.