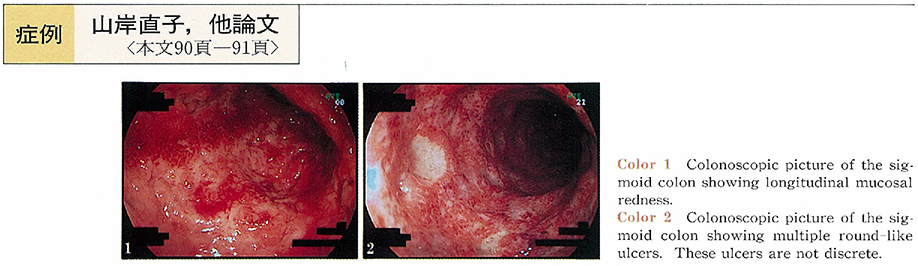
This paper represents a 40-year-old UC case, of which lesion was un-favorably reactivated after proctopexy. She was diagnosed as UC (total colitis type) in 1984 and had been medicated with by prednisolone (PSL) and salazosalfapyridine (SASP) . Ever since medication was quitted in 1988, she had been in remission stage successfully. There had been neither clinical symptoms nor colonoscopical finding which would suggest relapsing. In July 1998, she was performed proctopexy for proctoptosis under spinal anesthesia. Although only negligible erosions were seem in rectal mucosa during the surgery, severe low abdominal pain and bloody diarrhea (4-5 times/day) happened to appear two days after the surgery (Day2) . Diclofenac sodium suppository had been used as antipyresis and analgesic for four days (Day 6-9) . Sigmoidscopy was performed at 10 days after proctopexy. It was observed that diffuse mucosal edema and erosions in the rectum and sigmoid colon, diagnosed as severe UC. Furthermore, longitudinal mucosal redness and round-like ulcers in the sigmoid colon were also observed. Immediately PSL (50mg/day) and antibiotics were administered by bolus drip infusion for one hour under fasting and hyperalimentation control and the symptoms had disappeared mostly within a week. This onset might result from surgical procedures and/or NSAID suppository.