Abstract
In order to assess the long-term impact of the Great East Japan Earthquake on the oral health of disaster victims and to evaluate gene-environmental interactions in the development of major oral diseases and oral-systemic associations, the oral part of two large-scale genome cohort studies by the Tohoku Medical Megabank Organization (ToMMo), including the Community-based cohort (CommCohort) study and the Birth and Three-Generation cohort (BirThree) study, have been conducted. The study population comprised 32,185 subjects, including 16,886 participants in the CommCohort study and 15,299 participants in the BirThree cohort study, recruited from 2013 to 2017. The oral studies consist of a questionnaire regarding oral hygiene behavior, clinical examinations by dentists, and oral plaque and saliva sampling for microbiome analyses, which were carried out at seven community support centers in Miyagi prefecture. The median age of all participants was 55.0 years, and 66.1% of participants were women. Almost all participants reported that they brushed their teeth more than once a day. The median number of present teeth was 27.0, and the decayed, missing and filled tooth number was 16.0, with a significant difference according to age and sex. The median periodontal pocket and clinical attachment level was 2.48 mm and 4.00 mm, respectively. Periodontal parameters increased significantly according to age, except for the accumulation of dental calculus. The oral part of these extensive cross-sectional studies provides a unique and important platform for future studies on oral health and diseases that elicit through interactions with systemic diseases, lifestyles, life events and genetic backgrounds, and contributes to researches clarifying the long-term effects of disasters on oral health.
Introduction
After the Great East Japan Earthquake (GEJE) in 2011, the regional and community medical systems in the Tohoku district of Japan collapsed (Ishigaki et al. 2013). To foster creative reconstruction after the disaster and establish an advanced medical system aimed toward personalized medicine and healthcare, we established the Tohoku Medical Megabank Organization of Tohoku University (ToMMo) and the Iwate Tohoku Medical Megabank Organization (IMM) (Kuriyama et al. 2016). Both organizations set up a common framework, the Tohoku Medical Megabank Organization (TMM), and in collaboration developed a common TMM biobank that combines medical and genomic information under the concept of an integrated biobank (Minegishi et al. 2019). The TMM has been conducting two large-scale, prospective, genome cohort studies, the Community-based cohort (CommCohort) study, consisting of a population-based cohort with approximately 88,000 participants (Hozawa et al. 2020), and the Birth and Three-Generation (BirThree) cohort study, with approximately 73,500 participants, including babies and their parents, siblings, grandparents, and extended family members (Kuriyama et al. 2019). Both cohorts started recruit in 2013 and completed recruitment by 2017. Detailed follow up examinations of participants in both cohorts have been conducted since 2017 at an interval of approximately 5 years.
To date, there have been a number of investigations on the impacts of this major disaster on the general and oral health conditions of the inhabitants in the affected area, including physical and mental stressors caused by the earthquake. For instance, there are reports on myocardial infarction (Hao et al. 2014), stroke (Omama et al. 2013), depression (Sakuma et al. 2015), diabetes (Tanaka et al. 2015), pneumonia (Ohkouchi et al. 2013), and periodontitis (Tsuchiya et al. 2015). We surmise that oral hygiene deterioration due to devastation of the living environment, especially water shortage, could lead to various dental problems in the aftermath. Most dental problems, such as dental caries and periodontitis, that emerge in the inhabitants of a disaster-affected area are common chronic infectious diseases occurring in the human oral cavity and are major causes of missing teeth.
Recent population-based studies have revealed strong associations between oral conditions and systemic diseases, such as diabetes mellitus (Kim et al. 2018), arteriosclerosis (Aarabi et al. 2015), aspiration pneumonia (Taylor et al. 2000), and pregnancy complications (Michalowicz et al. 2006). A remarkable coincidence among oral and systemic diseases has also been noted for lifestyle-related diseases (Lira-Junior and Figueredo 2016; Aarabi et al. 2017; Chapple et al. 2017; Strauss et al. 2018). The following explanations may be pertinent to explain these links between oral and systemic diseases: 1) the inflammatory burden of oral infectious diseases may influence general conditions; 2) genetic risk factors common affect both oral and systemic diseases may reside; and 3) unexplained confounding factors related to both oral and systemic diseases may exist.
Based on these observations, we designed the scope of the oral health studies of the ToMMo cohort projects. We aimed to establish a database on the oral health of the people who suffered from the 2011 GEJE by assessing dental caries and tooth loss, restorative treatments, periodontitis, oral mucosa conditions, signs of temporomandibular joint (TMJ) function, oral care habits and oral health-related quality of life in the Miyagi prefecture. We also aimed to gather evidence of the links between oral health/diseases and general/systemic conditions through examinations of the population’s lifestyle and genetic predisposition. In the present article, the design of the oral health studies is documented along with the examination methods, study populations, and questionnaire content. We also documented some of the baseline results related to oral health, such as dental and periodontal conditions.
Materials and Methods
Data collection methods and management
The examination was conducted with a plane dental mirror (11B1X1000625D001, YDM Corporation, Tokyo), and a sharp-pointed dental explorer (11B1X1000664D103, YDM Corporation) was used to detect caries or other defects, as necessary. No radiographs were collected from any participant.
Dentition status
The dentition status was obtained for all teeth, including primary teeth and third molars, in all participants. Before the oral examination, dentures were removed, but teeth were not air-dried or cleaned. The tooth status was recorded at ten (1-10) or eleven (1-11) levels. The levels were determined as follows, sound (level 1); decayed, with/without filling (2); filled, no decay (3); missing, need for prosthesis (4); missing, no need for prosthesis, or unerupted (5); artificial tooth of fixed prosthesis (6); artificial tooth of removable prosthesis (7); unrestored stump covered with removable prosthesis (8); restored stump covered with removable prosthesis (9); dental implant (10) and sealed fissure (11). The level 11 was assessed for only under-20 aged participants.
Abnormal tooth growth
The following abnormal tooth growth was recorded for each tooth: hyperdontia; microdontia; fused tooth; enamel hypoplasia (molar-incisor hypomineralization; MIH); and congenital anodontia.
Tooth wear
When a tooth was visually examined for the presence of exposed dentine, tooth wear was recorded for each tooth according to the simplified scoring criteria for the tooth wear index (Bardsley et al. 2004), because the correlation of the accuracy of visual and histological examinations is poor (Ganss et al. 2006).
Periodontal examination
The periodontal examination was performed at several locations around the entire circumference of all present teeth, including the third molars, using a disposable WHO periodontal probe furnished with a ball tip (11B1X1000664D004, YDM Corporation). Several clinical measures of periodontal conditions were recorded in millimeters regarding the deepest periodontal pocket site of each tooth, including the probing depth (PD), defined as the distance from the gingival margin to the base of the gingival sulcus, and the clinical attachment level (CAL), defined as the distance from the cemento-enamel junction (CEJ) to the base of the sulcus, although we did not record the CAL if the CEJ was not visible. Bleeding on probing (BOP) indicated whether bleeding from within the periodontal pocket of each tooth occurred when performing a probing operation. The mobility of each tooth was examined using dental forceps (27B3X00017000012, Nichiei Co., Ltd., Osaka) and one finger to move the tooth in the horizontal and vertical directions, and tooth mobility (TM) was scored according to Miller’s criteria (Salvi et al. 2015). Identification of the presence of dental calculus (DC) on the supra- and subgingival surfaces of teeth was carried out using a disposable WHO probe and recorded as “absent” or “present” for teeth #11, 16, 17, 26, 27, 31, 36, 37, 46, and 47, numbered using the Zsigmondy-Palmer system.
Oral hygiene status
Plaque deposition on the tooth surface was classified as small, medium, high, or extremely high. The tongue coating was assessed using the following codes (Miyazaki et al. 1995): absence of plaque on tongue (code 0); thin plaque covering less than one-third of the tongue surface (code 1); thin plaque covering less than two-thirds of the tongue surface or thick dental plaque covering less than one-third of the tongue surface (code 2); thin plaque covering more than two-thirds of the tongue surface or thick dental plaque covering less than two-thirds of the tongue surface (code 3); and thick plaque covering more than two-thirds of the tongue surface (code 4).
Soft tissue conditions in the orofacial area
The location, size and color of oral mucosa lesions and the soft tissue conditions in the orofacial area were recorded in all participants.
Frenal attachment
The presence of abnormalities in the attachment of the tongue and superior labial frenum was assessed.
Oral tori
The location and size of palatal and mandibular tori, buccal exostoses and any bone outgrowths in the oral cavity were recorded. Participants with these bony outgrowths were asked whether they had oral habits, such as tooth clenching and grinding, and the answers were recorded as “present with self-awareness,” “present without self-awareness,” “absent,” or “unknown.”
TMJ function
Voluntary maximum mouth opening was measured as the distance between the edges of the lower and upper incisors using a digital caliper (AD-5765-100, A&D Company, Limited, Tokyo, Japan) to the nearest 0.1 mm. TMJ noise was examined on each side, as follows: “absent” or “present,” including clicking, popping, or crepitus. Pain or tenderness in the TMJ and associated masticatory muscles was checked during mandibular functions, including mouth opening, mouth closing, and chewing, or spontaneously. TMJ and associated masticatory muscle pain were also assessed by means of manual palpation.
Occlusion (tooth contact)
Each contacted tooth was recorded during intercuspal occlusion. Overjet and overbite were recorded as the distance, in millimeters, between the ridge of the upper and lower central incisors in the intercuspal position. Cross-bite, which is a form of malocclusion in which there is a reversal of the normal relationship of the mandibular and maxillary teeth, with lateral displacement of opposing teeth, was recorded as “absent” or “present.”
Collection of dental plaque, tongue coating, and saliva samples
Supragingival plaque was obtained from two molars (#16 and #26) by swiping the tooth surface with a sterile Gracey Curette (ROUND SAKURA H #G11-12, 11B1X1000662D102, YDM Corporation). If the index first molar was missing and the second molar in the same quadrant was present, the sample was obtained from the second molar instead. If both the first and second molars were absent, the sample were collected from the premolar closest to the missing index teeth. If all maxillary molars in the quadrant were absent, the sample was obtained from mandibular molars on the same side. A tongue coating specimen was obtained from the dorsum of the tongue by swabbing with a plastic spatula. After collection, the plaque and tongue coating samples were immediately immersed in saline in a polypropylene tube (CryoELITE, 2 ml, W985865, Weathon, NJ). Unstimulated saliva samples were collected in sterilize centrifuge tubes (50 ml, VIO-50 #150065, AS ONE Corp., Tokyo). The samples were immediately stored at –80℃ until transportation to our laboratory. Then, the saliva samples were thawed at room temperature and separated into the following three portions: 1) whole saliva (1 ml); 2) solid components of remaining saliva (1 ml), including pelleted oral microbiota, after centrifugation at 20,000 g for 10 min at 4℃; and 3) the supernatant separated from the same saliva by centrifugation. Each portion was dispensed into a Matrix storage tube (1.4 ml, Thermo Fisher Scientific, Inc., MA) and stored at –80℃ until use in future experiments (Yamagishi et al. 2016).
Statistical analysis
Numerical data are presented as the median and interquantile range. The interquartile range (IQR) represents the range from the 25th percentile to the 75th percentile, or the middle 50 percent as median, of each data set. The distributions of dental and periodontal parameters were tested for normality using the Kolmogorov-Smirnov (KS) test. The Kruskal-Wallis test was used to examine differences among age groups. Differences in dental and periodontal parameters among age groups were tested by chi-squared test. All statistical analyses were performed using SAS software (SAS 9.4, SAS Institute, NC, USA) and SAS enterprise guide. P values less than 0.05 were considered to indicate statistical significance.
Results
Populations of the oral health study and age distribution of participants
Participants who visited seven ToMMo community support centers in Miyagi prefecture from October 28, 2013, to June 30, 2017, and received an oral examination and/or general health check were registered for this oral health survey. As shown in Fig. 1, a total of 37,575 residents, including 13,459 males (median age 45.0 years (IQR: 32.0-65.1)), and 24,116 females, (median age 52.1 years (IQR: 34.0-63.1)) were included in either the CommCohort or BirThree cohort study. Among the participants, 4,695 who discontinued oral examinations were excluded. We also excluded 90 participants who withdrew consent and 222 died before March 05, 2020. In addition, 383 under 20 years old participants were excluded. Consequently, there was a total of 32,185 participants, including 16,886 participants (males, 4,982; median age 65.1 years (IQR: 55.0-77.1); females, 11,904; median age 60.1 years (IQR: 48.6-66.1)) in the CommCohort study, 15,299 participants (males, 5,928; median age 38.0 years (IQR: 32.0-59.1); females, 9,371; median age 37.1 years (IQR: 31.1-58.1)) in the BirThree cohort study, who served as the subjects of the baseline oral health survey in this cohort (Fig. 1). Note that 945 participants, who were recruited in both cohort studies, were received oral health examination for either or both cohort studies. Among them, 42 participants were examined oral health for both cohorts. In order to avoid the potential inclusion of duplicate data, in the present study we divided the 945 participants into either cohort (CommCohort; 634, BirThree cohort; 311) according to their initial oral health examination.
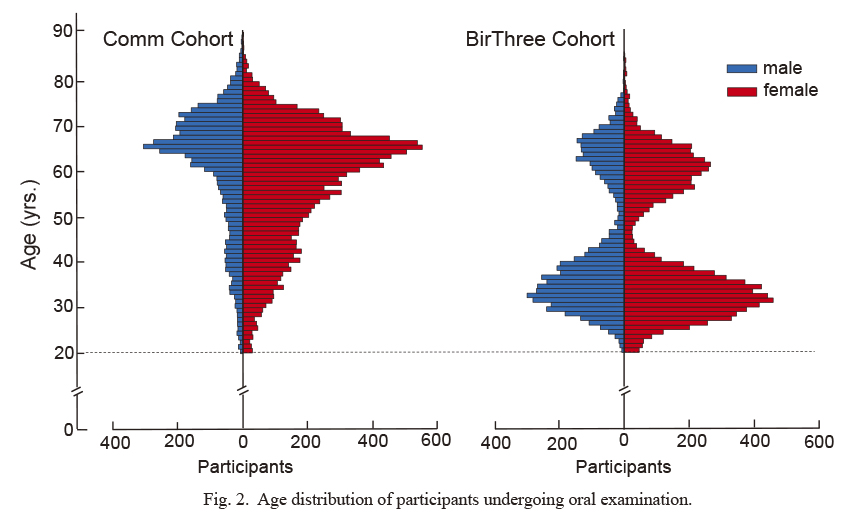
We examined the age distribution of 32,185 participants who underwent oral examinations for the CommCohort and BirThree cohort studies (Fig. 2). It should be noted that the participants in these cohort studies showed a wide age distribution. The CommCohort participants showed a peak age in the 60s in the age distribution (Hozawa et al. 2020), while the BirThree participants showed two peaks, one in the 30s and the other in 60s, reflecting the two major generations i.e., parents and grandparents (Kuriyama et al. 2019). Thus, a significant difference between the CommCohort and BirThree cohort studies was found in the median age (62.0 years and 38.0 years, respectively; p < 0.001). In addition, there is another significant difference in the female-to-male ratio (2.39 and 1.58, respectively; p < 0.001).
We further examined and collected data and samples from children in the BirThree cohort study who were elder siblings of newborns or adults. Table 1 shows the extent of examinations performed for the children, adolescents, and adults. While we executed this plan for studying children, in the current baseline analysis we excluded 383 of the children, as our recruitment of children and adolescents is ongoing to increase the sample size. Analyses of the children and adolescents will be reported elsewhere.
Examiners, oral health questionnaire, and ethical considerations
We wished to conduct a comprehensive oral examination of participants by dentists. To this end, we organized a team of 133 examiners, which comprised 7 assistant professors in the ToMMo and 126 dentists/graduate students who belong the Graduate School of Dentistry, Tohoku University. All examiners retained a dentist’s license in Japan and not only were given specific instructions in an orientation meeting regarding the oral examination methods in the ToMMo cohort studies but also received on-the-job training before participation in the oral examination program. Through this design, a high level of quality control for the collection of plaque and saliva samples was attained.
Participants in the present oral health survey completed a questionnaire consisting of 8 questions (Table 2). The questionnaire asked about oral health status, oral health problems, oral hygiene habits and the utilization of dental care. Almost all (98.6%) participants answered they brushed their teeth more than once a day (male; 96.7%, female; 99.4%). However, males brushing their teeth more than twice a day were significantly fewer than females (male: 65.8%, female: 86.5%, p < 0.0001, Chi-square-test).
Our genome medical research coordinator (GMRC), who was specially trained in house and licensed, informed eligible persons of the aims and protocols of the ToMMo oral health study and obtained their informed consent (Sakurai-Yageta et al. 2019). We adopted general and continuing consent to participate in the TMM studies. At baseline, we specifically explained the protocols of the cohort studies, biobanking, and general research methods for the genomic analyses, other omic analyses, and immortalized cell preparation.
Approval was obtained from the Institutional Review Board (IRB) and Ethics Committee of Tohoku University Graduate School of Medicine. This study was conducted in accordance with the Declaration of Helsinki, Ethical Guidelines for Human Genome/Gene Analysis Research, and other appropriate guidelines.
Present tooth number and tooth loss
Data regarding the dental examinations, questionnaires, oral samples, basic information, blood samples, and numbers of participants in our oral health cohort study are shown in Table 3. Especially, our participants almost fully finished genome analysis using Japanese-specific full custom array, which is referred to as Japonica Array™ (JPA) (Fuse et al. 2019; Yasuda et al. 2019). Details of the other surveys will be published elsewhere. Utilizing the data collected from the CommCohort and BirThree cohorts, we conducted a series of analyses of the basic dental health care data.
We first examined how many natural teeth the participants of the CommCohort and BirThree cohort studies retained, in reference to sex, age group and geographical location (Table 4) The locations of the community support centers were described previously (Kuriyama et al. 2019). In both cohort populations, most adults had 20 or more teeth (CommCohort: 83.7%, BirThree cohort: 93.2%). The number of teeth present decreased with age, and significant differences were observed in the number of teeth present among the age groups (p < 0.001). A minority (CommCohort: 1.5%, BirThree cohort: 0.5%) of the present study population had no natural teeth, and most of the edentulous persons were 55 years old or older. Significant variation in edentulousness was observed in relation to sex (p < 0.001), geographical location (p < 0.001) and cohort (p < 0.001).
The median number of natural teeth present in the BirThree cohort was 28.0, which was significantly higher than that of 26.0 in the CommCohort (p < 0.001). We surmised that this difference in the number of natural teeth reflected the difference in the age distribution of the cohorts (Fig. 2). Geographical variation was also observed regarding the number of teeth among the participants (p < 0.05). Participants in heavily Tsunami devastated area (Ishinomaki and Kesennuma) tended to show fewer numbers of natural teeth than those in inland area (Osaki and Shiroishi).
Caries and caries expression
We then examined the burden of caries in the participants of the CommCohort and BirThree cohort studies in reference to sex, age group and geographical location. The caries burden is expressed for the whole study population according to the following components: decayed teeth (DT); missing teeth (MT); and filled teeth (FT). These components were grouped and are referred to as DMFT (Table 5). The median DMFT value was 18.0 (IQR: 13.0-22.0) for the CommCohort and 14.0 (IQR: 9.0-19.0) for the BirThree cohort, indicating a significant difference in the median DMFT value between these two cohorts (p < 0.001). The difference in the median DMFT value was reproducible when the data were examined separately by sex (p < 0.001). Participants in heavily Tsunami devastated area (Ishinomaki and Kesennuma) tended to show higher DMFT values than those in inland area (Osaki and Shiroishi).
We found that the median DMFT was increased in both cohorts gradually with age and was increased by over 10 teeth in those aged 55-64 years when compared with those aged 20-24 years. This increase persisted in the oldest age group (Table 5). On the other hand, the occurrence of untreated caries (the DT component) was very low, with a median value of almost 0.0 DT for all age groups except for younger groups. In both cohorts, the median MT component increased with age (p < 0.001), and in the oldest age group, the value was 9.0 in the CommCohort (IQR: 4.0-17.0) and in the BirThree cohort (IQR: 4.0-15.0). In contrast, the FT component started decreasing in those aged 55-64 years and continued decreasing to the oldest age group in both cohorts. This was inversely correlated with an increase in missing teeth, or the MT component. The FT component was larger in females than in males (p < 0.01). Regarding geographical differences, we did not find large differences among the seven support center regions.

We also examined the periodontal conditions of the participants in the CommCohort and BirThree cohort studies in reference to sex and age group. Periodontal parameters were estimated, excluding the edentulous participants. We found that in both cohort populations, the median periodontal pocket depth (PPD) became deeper with age (Table 6). Except for those in the oldest age group (over 75 years old), the median PPD of males was significantly larger than that of females, at 2.65 vs. 2.46 in the CommCohort and 2.54 vs. 2.39 in the BirThree cohort (both p < 0.001). Posterior teeth showed a deeper PPD than anterior teeth (data not shown). The PPD in the total CommCohort and BirThree cohort populations also showed a significant difference, and this difference was reproducible in both the male and female participants in the two cohorts.
In this study, we measured the CAL for each tooth when the CEJ was visually recognized at the measurement site. Only 1.4-2.2% of the participants in the youngest age group (20-24 years old) had at least one tooth with a measurable CAL. The proportion of participants with a measurable CAL increased with age and reached 25.8-42.1% at 75 years old and older (Fig. 3). Table 7 shows the number of participants with at least one CAL and the median CAL (mm). A larger median CAL in males than in females (p < 0.001) and in older age groups than younger age groups (p < 0.001) was found in both cohorts. These results indicate that there are differences in periodontal regeneration according to sex and age.
We also measured BOP to assess periodontal inflammation in the participants. Table 8 shows the number of participants and the number of teeth with BOP. Consistent with previous observations, we observed more teeth with BOP in the youngest age group and in males than in the older age groups and in females in both the CommCohort and BirThree cohort (Table 8). With aging, the number of teeth with BOP decreased more significantly in males than females (males: 2.0-4.0, females: 0.5-3.0). The prevalence of teeth with BOP was higher in males than in females. Both cohorts showed almost the same tendency in these parameters.
We measured the nonphysiological tooth mobility (TM) of all teeth of the participants in both cohorts with Miller’s criteria, and expressed the result as either negative or positive. Table 9 presents the median percentage of positive tooth among present teeth of participants. Nonphysiological TM was not observed often in either cohort until the age of 45 years. However, after that age, the median number of teeth with nonphysiological TM progressively increased with age (Table 9). This trend in the prevalence of nonphysiological TM according to age was statistically significant in both the CommCohort and the BirThree cohort studies, but there was no difference according to sex.
The presence of DC on the present indexed teeth was measured and is expressed as a ratio. In both cohort populations, the number of index teeth positive for supra- and subgingival calculus was significantly lower in females than in males, indicating a strong difference according to sex (Table 10). Almost all participants in their 20s had every index tooth, whereas elderly participants had a small percentage of the index teeth. This loss of index teeth with aging was related to the tooth type; the lower incisors (94.7%) showed the highest survival rate, followed by the upper incisors (88.3%), upper molars (82.3%) and lower molars (74.3%). The presence of DC on each type of tooth is shown in Table 11. The frequency at which DC was detected on the lower incisors was 63.2% in males and 48.1% in females. DC was observed on the other nine index teeth at a similar low frequency (males, 17.7 to 24.1%; females, 10.4 to 14.8%).
Discussion
To clarify the interactive effects of genetic and environmental factors on the occurrence of common diseases, large-scale cohort studies with various genomic and other omic analyses have been conducted in a number of countries (Miyamoto et al. 2016; Kalsbeek et al. 2018; Rutten-Jacobs et al. 2018). Recent progress in the technical, ethical and social aspects of these genome cohort studies has allowed us to collect a large number of healthy residents using a questionnaire-based survey (Hayasaka et al. 2013). Although many reports from such studies suggested a close relationship between oral conditions and general health/diseases (Dorfer et al. 2017), large-scale genome cohort studies focusing on the association of oral conditions and general health/diseases have not yet been established. The ToMMo project aims to address this issue, and elaborate objective oral examinations have been designed within genome cohort studies. Here, as the first step to accomplish this goal, we describe the initial progress and findings of the oral examinations, as well as the design of the cohort studies, especially focusing on the oral examinations.
Of the participants in two ToMMo cohorts, i.e., the CommCohort and the BirThree cohort, 32,185 participants underwent an oral examination performed by specially trained dentists. This number is equivalent to 25.3% of all participants in the two genome cohort studies. It should be noted that over 90% of the participants who were less than 60 years old retained more than 20 natural teeth. After the age of 60 years, the proportion of edentulous participants progressively increased; nonetheless, 55.0% of the participants aged 75 years or more had more than 20 natural teeth. These observations show very good agreement with the results of the previous survey of the Japanese adult population, with approximately 3820 participants (Ministry of Health, Labour and Welfare, Japan 2016). In collaboration with the previous study, the rate of edentulism in our survey conclusively proves that the rate in Japan is much lower than that in most countries in the world (World Health Organization 2019). We surmise that the lower tooth mortality rate in our participants and in Japan is achieved by the high level of hygiene habits and development of the dental health care system. In fact, regarding the former, 98% of our participants answered in the questionnaire that they brush their teeth more than once a day.
The total caries experience among our participants aged 35-44 years, indicated by a median DMFT index of 14.0 in the CommCohort and 13.0 in the BirThree cohort, is slightly higher than that among adults in Japan (DMFT index, 12.1; 35-44 years) (Ministry of Health, Labour and Welfare, Japan 2016). Whereas several industrialized Western countries, including Sweden (12.5), Denmark (13.5), the UK (16.6) and the USA (10.9), showed comparable DMFT indices in those aged 35-44 years, the caries burden in our cohorts and in the Japan national survey were appreciably higher than those in neighboring countries in East Asia (China, 3.11; Korea 5.5; both 35-44 years) (World Health Organization 2019). These differences suggest that the etiology and progression of dental caries are influenced by both lifestyle and genetic factors. We noted that participants living in the heavily disaster-affected areas (Ishinomaki and Kesennuma) tended to show a higher DMFT index than those living inland areas (Osaki and Shiroishi). To further validate the relationship of stress/disaster experience and caries development, we are planning to analyze the other environmental factors recorded simultaneously in our cohort studies, which include changes in amounts of drinking and smoking and stressors caused by drastic changes in living environments.
Periodontal registrations in the present survey were performed at one site per tooth, during which the deepest PPD and CAL around each tooth was recorded. This simplified method for recording the pathology of the periodontal tissue is designed for cohort studies (Salvi et al. 2015). We envision that in large-scale epidemiological analyses, even if multiple-site measurements are conducted, the largest value of periodontal parameters will be considered the representative value of the tooth concerned (Zimmermann et al. 2015). The CAL is used to estimate the amount of tissue lost in periodontal diseases and to identify the apical extension of the inflammatory lesion. If the CEJ appears at the crown side of the gingival margin, the CAL measurement is simple. However, if the CEJ is located at the same level as the gingival margin or at the root side of the margin, the examiners have to detect the CEJ using a periodontal probe under blind conditions. In the latter case, accurate measurement of the CAL becomes difficult (Leroy et al. 2010). Therefore, in this study, if the CEJ was visible, we measured the CAL, but if the CEJ was not visible, we avoided measuring the CAL. A small proportion (1.4-2.2%) of participants with a visible CEJ was observed in the youngest age group (20-24 years), but the proportion increased with age and reached 25.8% in females and 42.1% in males in the BirThree cohort above the age of 75 years, indicating that the proportion of individuals with a visible CEJ is much smaller than previously expected (Holtfreter et al. 2010; Yin et al. 2017).
The median CAL in the present study was 4.38 mm in males in the CommCohort and 4.50 mm in males in the BirThree cohort, whereas the median CAL was 4.00 mm in females in the respective cohorts. These indices are higher than those reported in previous population-based studies, such as 1.9 mm in Japan (median age, 55.7 years) (Shimazaki et al. 2007), 1.59 mm in the USA (those aged 30 years or more) (Eke et al. 2012a), 3.7 ± 1.1 mm in China (nonpregnant women, 27.1 ± 4.0 years) (Wu et al. 2013), and 3.62 mm (females, 55-64 years) and 3.97 mm (males, 55-64 years) in Denmark (Kongstad et al. 2013). Upon the interpretation of these data, it is important to consider the fact that the assessment rule used in the present survey tends to exclude healthy subjects without gingival recession. Therefore, the comparison should not be evaluated directly.
TM represents the movement of loose teeth within their sockets. As a periodontal parameter, TM is an effective indicator of external force applied to teeth, including bite force. TM also serves as an effective parameter of periodontal tissue destruction by inflammation in the periodontal pocket (Reinhardt and Killeen 2015). In this survey, we found that TM increased sharply with age. TM was higher in males than in females. These changes are similar to those observed in the PPD and CAL (Wu et al. 2016). In contrast, in this study, we found that there was no significant change in BOP with increasing age. This point is controversial in the literature, as similar findings have been shown by several epidemiological reports (Eke et al. 2012b; Zimmermann et al. 2015), while one other report showed that the percentage of participants with BOP increased with age (Kongstad et al. 2013). Our results are similar to the former results and support the notion that BOP is an early sign of gingivitis rather than of the progression of periodontal disease (Greenstein 1984).
Our survey demonstrates that DC formed most abundantly on the surfaces of the mandibular incisors, detected at a rate of, 63.1% among males in the CommCohort and 63.2% among males in the BirThree cohort and, 50.3% and 45.5% among females in the respective cohorts, followed by the maxillary and mandibular molars. In contrast, the least amount of DC formed on the maxillary incisors, detected at a rate of, 18.8% among males in the CommCohort and 17.0% among males in the BirThree cohort and 11.3% and 8.5% among females in the respective cohorts. These results show very good agreement with the finding that supragingival calculus accumulates on the surface of teeth close to the orifices of major salivary glands in both the mandible and maxilla (White 1997; Jin and Yip 2002). These results support the contention that DC itself may not be pathogenic but serves as a contributing factor, leading to the accumulation of dental plaque on the rough surface generated by DC.
The present study reveals a higher prevalence and severity of periodontal disease in males than in females. This difference in periodontal disease has been considered to be associated with hormones, pregnancy in young females, and behavioral differences between the sex, such as higher rates of smoking and relatively poor oral hygiene in males (Shiau and Reynolds 2010; Eke et al. 2012a; Cepeda et al. 2017). Meanwhile, many studies have identified a higher prevalence and susceptibility to dental caries in females (Martinez-Mier and Zandona 2013; Shaffer et al. 2015). Our results provide further insights into their observations. For instance, we found a higher number of FT but lower numbers of DT and MT in females than in males, supporting the hypothesis that females compensate for their susceptibility to caries by more frequently visiting dental clinics (Ministry of Health, Labour and Welfare, Japan 2010).
In conclusion, we document the results of oral health examinations of more than 33,000 inhabitants who experienced the GEJE and participated in our two large-scale genome cohort studies. The prevalence and severity of dental caries and periodontal disease among the participants are higher than those in population-based surveys executed previously in Japan and several other countries. It is difficult to obtain oral health data of our participants from before the GEJE, and an accurate assessment of the impact of natural disaster-related stressors on oral health cannot be carried out. We hope that our present data will be useful for future disaster-based oral health studies in the world. The oral health data will be combined with general health data in our cohort studies. Oral health/disease and general conditions, including genetic background, should be longitudinally followed to elucidate lifestyle-related, common diseases. The causal relationships between oral and general health, including the long-lasting effects of the GEJE, should also be investigated.
Acknowledgments
The authors sincerely express their gratitude to the people of Japan and of the world for their valuable support to the GEJE-affected areas after the disaster. We would also like thank all participants and all municipality staff who helped our project. We also thank the members of the ToMMo and IMM, including the GMRCs, office and administrative personnel, and software engineers, for their assistance with the projects. The complete list of members is available at https://www.megabank.tohoku.ac.jp/english/a191201/ for the ToMMo and at http://iwate-megabank.org/en/about/departments/ for the IMM. The TMM is supported by grants from the Reconstruction Agency, from the Ministry of Education, Culture, Sports, Science and Technology (MEXT), and from the Japan Agency for Medical Research and Development (AMED) under Grant Number JP19km0105001.
Conflict of Interest
The authors declare no conflict of interest.
References
-
Aarabi,
G.,
Eberhard,
J.,
Reissmann,
D.R.,
Heydecke,
G. &
Seedorf,
U.
(2015) Interaction between periodontal disease and atherosclerotic vascular disease: fact or fiction? Atherosclerosis, 241, 555-560.
-
Aarabi,
G.,
Zeller,
T.,
Seedorf,
H.,
Reissmann,
D.R.,
Heydecke,
G.,
Schaefer,
A.S. &
Seedorf,
U.
(2017) Genetic susceptibility contributing to periodontal and cardiovascular disease. J. Dent. Res., 96, 610-617.
-
Bardsley,
P.F.,
Taylor,
S. &
Milosevic,
A.
(2004) Epidemiological studies of tooth wear and dental erosion in 14-year-old children in North West England. Part 1: the relationship with water fluoridation and social deprivation. Br. Dent. J., 197, 413-416; discussion 399.
-
Cepeda,
M.S.,
Weinstein,
R.,
Blacketer,
C. &
Lynch,
M.C.
(2017) Association of flossing/inter-dental cleaning and periodontitis in adults. J. Clin. Periodontol., 44, 866-871.
-
Chapple,
I.L.,
Bouchard,
P.,
Cagetti,
M.G.,
Campus,
G.,
Carra,
M.C.,
Cocco,
F.,
Nibali,
L.,
Hujoel,
P.,
Laine,
M.L.,
Lingstrom,
P.,
Manton,
D.J.,
Montero,
E.,
Pitts,
N.,
Range,
H.,
Schlueter,
N., et al.
(2017) Interaction of lifestyle, behaviour or systemic diseases with dental caries and periodontal diseases: consensus report of group 2 of the joint EFP/ORCA workshop on the boundaries between caries and periodontal diseases. J. Clin. Periodontol., 44 Suppl 18, S39-S51.
-
Dorfer,
C.,
Benz,
C.,
Aida,
J. &
Campard,
G.
(2017) The relationship of oral health with general health and NCDs: a brief review.. Int. Dent. J., 67 Suppl 2, 14-18.
-
Eke,
P.I.,
Dye,
B.A.,
Wei,
L.,
Thornton-Evans,
G.O. &
Genco,
R.J.
(2012a) Prevalence of periodontitis in adults in the United States: 2009 and 2010. J. Dent. Res., 91, 914-920.
-
Eke,
P.I.,
Page,
R.C.,
Wei,
L.,
Thornton-Evans,
G. &
Genco,
R.J.
(2012b) Update of the case definitions for population-based surveillance of periodontitis. J. Periodontol., 83, 1449-1454.
-
Fuse,
N.,
Sakurai-Yageta,
M.,
Katsuoka,
F.,
Danjoh,
I.,
Shimizu,
R.,
Tamiya,
G.,
Nagami,
F.,
Kawame,
H.,
Higuchi,
S.,
Kinoshita,
K.,
Kure,
S. &
Yamamoto,
M.
(2019) Establishment of Integrated Biobank for Precision Medicine and Personalized Healthcare: The Tohoku Medical Megabank Project. JMA J., 2, 113-122.
-
Ganss,
C.,
Klimek,
J. &
Lussi,
A.
(2006) Accuracy and consistency of the visual diagnosis of exposed dentine on worn occlusal/incisal surfaces. Caries Res., 40, 208-212.
-
Greenstein,
G.
(1984) The role of bleeding upon probing in the diagnosis of periodontal disease. A literature review. J. Periodontol., 55, 684-688.
-
Hao,
K.,
Takahashi,
J.,
Ito,
K.,
Miyata,
S.,
Sakata,
Y.,
Nihei,
T.,
Tsuburaya,
R.,
Shiroto,
T.,
Ito,
Y.,
Matsumoto,
Y.,
Nakayama,
M.,
Yasuda,
S. &
Shimokawa,
H.;
Miyagi AMI Registry Study Investigators
(2014) Emergency care of acute myocardial infarction and the great East Japan earthquake disaster. Circ. J., 78, 634-643.
-
Hayasaka,
K.,
Tomata,
Y.,
Aida,
J.,
Watanabe,
T.,
Kakizaki,
M. &
Tsuji,
I.
(2013) Tooth loss and mortality in elderly Japanese adults: effect of oral care. J. Am. Geriatr. Soc., 61, 815-820.
-
Holtfreter,
B.,
Kocher,
T.,
Hoffmann,
T.,
Desvarieux,
M. &
Micheelis,
W.
(2010) Prevalence of periodontal disease and treatment demands based on a German dental survey (DMS IV). J. Clin. Periodontol., 37, 211-219.
-
Hozawa,
A.,
Tanno,
K.,
Nakaya,
N.,
Nakamura,
T.,
Tsuchiya,
N.,
Hirata,
T.,
Narita,
A.,
Kogure,
M.,
Nochioka,
K.,
Sasaki,
R.,
Takanashi,
N.,
Otsuka,
K.,
Sakata,
K.,
Kuriyama,
S.,
Kikuya,
M., et al.
(2020) Study profile of The Tohoku Medical Megabank Community-Based Cohort Study. J. Epidemiol. doi.:10.2188/jea.JE20190271. [Epub ahead of print].
-
Ishigaki,
A.,
Higashi,
H.,
Sakamoto,
T. &
Shibahara,
S.
(2013) The Great East-Japan Earthquake and devastating tsunami: an update and lessons from the past Great Earthquakes in Japan since 1923. Tohoku J. Exp. Med., 229, 287-299.
-
Jin,
Y. &
Yip,
H.K.
(2002) Supragingival calculus: formation and control. Crit. Rev. Oral Biol. Med., 13, 426-441.
-
Kalsbeek,
A.,
Veenstra,
J.,
Westra,
J.,
Disselkoen,
C.,
Koch,
K.,
McKenzie,
K.A.,
O’Bott,
J.,
Vander Woude,
J.,
Fischer,
K.,
Shearer,
G.C.,
Harris,
W.S. &
Tintle,
N.L.
(2018) A genome-wide association study of red-blood cell fatty acids and ratios incorporating dietary covariates: Framingham Heart Study Offspring Cohort. PLoS One, 13, e0194882.
-
Kim,
O.S.,
Shin,
M.H.,
Kweon,
S.S.,
Lee,
Y.H.,
Kim,
O.J.,
Kim,
Y.J. &
Chung,
H.J.
(2018) The severity of periodontitis and metabolic syndrome in Korean population: the Dong-gu study. J. Periodontal Res., 53, 362-368.
-
Kongstad,
J.,
Ekstrand,
K.,
Qvist,
V.,
Christensen,
L.B.,
Cortsen,
B.,
Gronbaek,
M.,
Holm-Pedersen,
P.,
Holmstrup,
P.,
Bardow,
A.,
Twetman,
S. &
Fiehn,
N.E.
(2013) Findings from the oral health study of the Danish Health Examination Survey 2007-2008. Acta Odontol. Scand., 71, 1560-1569.
-
Kuriyama,
S.,
Metoki,
H.,
Kikuya,
M.,
Obara,
T.,
Ishikuro,
M.,
Yamanaka,
C.,
Nagai,
M.,
Matsubara,
H.,
Kobayashi,
T.,
Sugawara,
J.,
Tamiya,
G.,
Hozawa,
A.,
Nakaya,
N.,
Tsuchiya,
N.,
Nakamura,
T., et al.
(2019) Cohort Profile: Tohoku Medical Megabank Project Birth and Three-Generation Cohort Study (TMM BirThree Cohort Study): rationale, progress and Perspective. Int. .J Epidemiol., 49, 18-19m.
-
Kuriyama,
S.,
Yaegashi,
N.,
Nagami,
F.,
Arai,
T.,
Kawaguchi,
Y.,
Osumi,
N.,
Sakaida,
M.,
Suzuki,
Y.,
Nakayama,
K.,
Hashizume,
H.,
Tamiya,
G.,
Kawame,
H.,
Suzuki,
K.,
Hozawa,
A.,
Nakaya,
N., et al.
(2016) The Tohoku Medical Megabank Project: Design and Mission. J. Epidemiol., 26, 493-511.
-
Leroy,
R.,
Eaton,
K.A. &
Savage,
A.
(2010) Methodological issues in epidemiological studies of periodontitis: how can it be improved? BMC Oral Health, 10, 8.
-
Lira-Junior,
R. &
Figueredo,
C.M.
(2016) Periodontal and inflammatory bowel diseases: is there evidence of complex pathogenic interactions? World J. Gastroenterol., 22, 7963-7972.
-
Martinez-Mier,
E.A. &
Zandona,
A.F.
(2013) The impact of gender on caries prevalence and risk assessment. Dent. Clin. North Am., 57, 301-315.
-
Michalowicz,
B.S.,
Hodges,
J.S.,
DiAngelis,
A.J.,
Lupo,
V.R.,
Novak,
M.J.,
Ferguson,
J.E.,
Buchanan,
W.,
Bofill,
J.,
Papapanou,
P.N.,
Mitchell,
D.A.,
Matseoane,
S. &
Tschida,
P.A.;
the OPT Study
(2006) Treatment of periodontal disease and the risk of preterm birth. N. Engl. J. Med., 355, 1885-1894.
-
Minegishi,
N.,
Nishijima,
I.,
Nobukuni,
T.,
Kudo,
H.,
Ishida,
N.,
Terakawa,
T.,
Kumada,
K.,
Yamashita,
R.,
Katsuoka,
F.,
Ogishima,
S.,
Suzuki,
K.,
Sasaki,
M. &
Satoh,
M.;
Tohoku Medical Megabank Project Study Group &
Yamamoto,
M.
(2019) Biobank establishment and sample management in the Tohoku Medical Megabank Project. Tohoku J. Exp. Med., 248, 45-55.
-
Ministry of Health, Labour and welfare, Japan
(2010) Survey of health and nutrition of Japan 2010. https://www.e-stat.go.jp/stat-search/files?page=1&layout=datalist&toukei=00450171&tstat=000001041744&cycle=7&tclass1=000001041745&stat_infid=000012521724 [Accessed: April 30, 2020] (in Japanese).
-
Ministry of Health, Labour and Welfare, Japan
(2016) Survey of dental diseases 2016. https://www.e-stat.go.jp/stat-search/files?page=1&layout=datalist&toukei=00450131&tstat=000001104615&cycle=0&stat_infid=000031607230&tclass1val=0 [Accessed: April 30, 2020] (in Japanese).
-
Miyamoto,
K.,
Iwakuma,
M. &
Nakayama,
T.
(2016) Experiences and attitudes of residents regarding a community-based genome cohort study in Japan: a population-based, cross-sectional study. BMC Med. Genomics, 9, 14.
-
Miyazaki,
H.,
Sakao,
S.,
Katoh,
Y. &
Takehara,
T.
(1995) Correlation between volatile sulphur compounds and certain oral health measurements in the general population. J. Periodontol., 66, 679-684.
-
Ohkouchi,
S.,
Shibuya,
R.,
Yanai,
M.,
Kikuchi,
Y.,
Ichinose,
M. &
Nukiwa,
T.
(2013) Deterioration in regional health status after the acute phase of a great disaster: respiratory physicians’ experiences of the Great East Japan Earthquake. Respir. Investig., 51, 50-55.
-
Omama,
S.,
Yoshida,
Y.,
Ogasawara,
K.,
Ogawa,
A.,
Ishibashi,
Y.,
Nakamura,
M.,
Tanno,
K.,
Ohsawa,
M.,
Onoda,
T.,
Itai,
K. &
Sakata,
K.
(2013) Influence of the great East Japan earthquake and tsunami 2011 on occurrence of cerebrovascular diseases in Iwate, Japan. Stroke, 44, 1518-1524.
-
Reinhardt,
R.A. &
Killeen,
A.C.
(2015) Do mobility and occlusal trauma impact periodontal longevity? Dent. Clin. North Am., 59, 873-883.
-
Rutten-Jacobs,
L.C.,
Larsson,
S.C.,
Malik,
R.,
Rannikmae,
K.,
consortium,
M.,
International Stroke Genetics,
C.,
Sudlow,
C.L.,
Dichgans,
M.,
Markus,
H.S. &
Traylor,
M.
(2018) Genetic risk, incident stroke, and the benefits of adhering to a healthy lifestyle: cohort study of 306 473 UK Biobank participants. BMJ, 363, k4168.
-
Sakuma,
A.,
Takahashi,
Y.,
Ueda,
I.,
Sato,
H.,
Katsura,
M.,
Abe,
M.,
Nagao,
A.,
Suzuki,
Y.,
Kakizaki,
M.,
Tsuji,
I.,
Matsuoka,
H. &
Matsumoto,
K.
(2015) Post-traumatic stress disorder and depression prevalence and associated risk factors among local disaster relief and reconstruction workers fourteen months after the Great East Japan Earthquake: a cross-sectional study. BMC Psychiatry, 15, 58.
-
Sakurai-Yageta,
M.,
Kawame,
H.,
Kuriyama,
S.,
Hozawa,
A.,
Nakaya,
N.,
Nagami,
F.,
Minegishi,
N.,
Ogishima,
S.,
Takai-Igarashi,
T.,
Danjoh,
I.,
Obara,
T.,
Ishikuro,
M.,
Kobayashi,
T.,
Aizawa,
Y.,
Ishihara,
R., et al.
(2019) A training and education program for genome medical research coordinators in the genome cohort study of the Tohoku Medical Megabank Organization. BMC Med. Educ., 19, 297.
-
Salvi,
G.E.,
Berglundh,
T. &
Lang,
N.P.
(2015) Examination of patients. In clinical periodontology and implant dentistry, 6th ed., edited by
Lang,
N.P. &
Lindhe,
J.
John Wiley & Sons Ltd., UK. pp. 559-573.
-
Shaffer,
J.R.,
Wang,
X.,
McNeil,
D.W.,
Weyant,
R.J.,
Crout,
R. &
Marazita,
M.L.
(2015) Genetic susceptibility to dental caries differs between the sexes: a family-based study. Caries Res., 49, 133-140.
-
Shiau,
H.J. &
Reynolds,
M.A.
(2010) Sex differences in destructive periodontal disease: exploring the biologic basis. J. Periodontol., 81, 1505-1517.
-
Shimazaki,
Y.,
Saito,
T.,
Yonemoto,
K.,
Kiyohara,
Y.,
Iida,
M. &
Yamashita,
Y.
(2007) Relationship of metabolic syndrome to periodontal disease in Japanese women: the Hisayama Study. J. Dent. Res., 86, 271-275.
-
Strauss,
J.F.
3rd,
Romero, R.,
Gomez-Lopez,
N.,
Haymond-Thornburg,
H.,
Modi,
B.P.,
Teves,
M.E.,
Pearson,
L.N.,
York,
T.P. &
Schenkein,
H.A.
(2018) Spontaneous preterm birth: advances toward the discovery of genetic predisposition. Am. J. Obstet. Gynecol., 218, 294-314 e292.
-
Tanaka,
M.,
Imai,
J.,
Satoh,
M.,
Hashimoto,
T.,
Izumi,
T.,
Sawada,
S.,
Uno,
K.,
Hasegawa,
Y.,
Kaneko,
K.,
Yamada,
T.,
Ishigaki,
Y.,
Imai,
Y. &
Katagiri,
H.
(2015) Impacts of the Great East Japan Earthquake on diabetic patients. J. Diabetes Investig., 6, 577-586.
-
Taylor,
G.W.,
Loesche,
W.J. &
Terpenning,
M.S.
(2000) Impact of oral diseases on systemic health in the elderly: diabetes mellitus and aspiration pneumonia. J. Public Health Dent., 60, 313-320.
-
Tsuchiya,
M.,
Aida,
J.,
Hagiwara,
Y.,
Sugawara,
Y.,
Tomata,
Y.,
Sato,
M.,
Watanabe,
T.,
Tomita,
H.,
Nemoto,
E.,
Watanabe,
M.,
Osaka,
K. &
Tsuji,
I.
(2015) Periodontal disease is associated with insomnia among victims of the Great East Japan Earthquake: a panel study initiated Three Months after the Disaster. Tohoku J. Exp. Med., 237, 83-90.
-
White,
D.J.
(1997) Dental calculus: recent insights into occurrence, formation, prevention, removal and oral health effects of supragingival and subgingival deposits. Eur. J. Oral Sci., 105, 508-522.
-
World Health Organization
(2019) Oral health country/area profile project. https://capp.mau.se/country-areas/ [Accessed: Apriil 30, 2020].
-
Wu,
Y.,
Dong,
G.,
Xiao,
W.,
Xiao,
E.,
Miao,
F.,
Syverson,
A.,
Missaghian,
N.,
Vafa,
R.,
Cabrera-Ortega,
A.A.,
Rossa,
C. Jr. &
Graves,
D.T.
(2016) Effect of aging on periodontal inflammation, microbial colonization, and disease susceptibility. J. Dent. Res., 95, 460-466.
-
Wu,
Y.M.,
Liu,
J.,
Sun,
W.L.,
Chen,
L.L.,
Chai,
L.G.,
Xiao,
X. &
Cao,
Z.
(2013) Periodontal status and associated risk factors among childbearing age women in Cixi City of China. J. Zhejiang Univ. Sci. B, 14, 231-239.
-
Yamagishi,
J.,
Sato,
Y.,
Shinozaki,
N.,
Ye,
B.,
Tsuboi,
A.,
Nagasaki,
M. &
Yamashita,
R.
(2016) Comparison of boiling and robotics automation method in DNA extraction for metagenomic sequencing of human oral microbes. PLoS One, 11, e0154389.
-
Yasuda,
J.,
Kinoshita,
K.,
Katsuoka,
F.,
Danjoh,
I.,
Sakurai-Yageta,
M.,
Motoike,
I.N.,
Kuroki,
Y.,
Saito,
S.,
Kojima,
K.,
Shirota,
M.,
Saigusa,
D.,
Otsuki,
A.,
Kawashima,
J.,
Yamaguchi-Kabata,
Y.,
Tadaka,
S., et al.
(2019) Genome analyses for the Tohoku Medical Megabank Project towards establishment of personalized healthcare. J. Biochem., 165, 139-158.
-
Yin,
W.,
Yang,
Y.M.,
Chen,
H.,
Li,
X.,
Wang,
Z.,
Cheng,
L.,
Yin,
Q.D.,
Fang,
H.Z.,
Fei,
W.,
Mi,
F.L.,
Nie,
M.H.,
Hu,
T. &
Zhou,
X.D.
(2017) Oral health status in Sichuan Province: findings from the oral health survey of Sichuan, 2015-2016. Int. J. Oral Sci., 9, 10-15.
-
Zimmermann,
H.,
Hagenfeld,
D.,
Diercke,
K.,
El-Sayed,
N.,
Fricke,
J.,
Greiser,
K.H.,
Kuhnisch,
J.,
Linseisen,
J.,
Meisinger,
C.,
Pischon,
N.,
Pischon,
T.,
Samietz,
S.,
Schmitter,
M.,
Steinbrecher,
A.,
Kim,
T.S., et al.
(2015) Pocket depth and bleeding on probing and their associations with dental, lifestyle, socioeconomic and blood variables: a cross-sectional, multicenter feasibility study of the German National Cohort. BMC Oral Health, 15, 7.