Abstract
Previous studies have shown that green tea catechins (GTCs) have beneficial effects on obesity and metabolic syndromes. In this study, we prepared kosen-cha from green tea using high pressure extraction, to reduce the astringent taste of the green tea. We identified a large quantity of polymerized GTCs in kosen-cha. To investigate the effects of kosen-cha containing polymerized GTCs in obese Japanese patients, we designed an open-label pilot study in which 6 obese subjects (body mass index (BMI) >25 kg/m2) were administered kosen-cha (5 g/L/d) for 12 weeks. Body composition, serum lipids, insulin resistance, vascular functions, and cardiac hypertrophy were measured before and 12 weeks after kosen-cha administration. Kosen-cha showed no significant adverse effects on the patients. Body weights, BMI, waist circumferences, serum triglyceride (TG) levels, and homeostasis model assessment as an index of insulin resistance (HOMA-IR) levels were significantly decreased after the 12 weeks of administration. Flow-mediated dilation (FMD) (p = 0.0214), brachial-ankle pulse wave velocity (baPWV)(p = 0.0141), left ventricular mass indexes (p = 0.0120), and plasma brain natriuretic peptide (BNP) (p = 0.0144) were significantly improved. Overall, kosen-cha reduced obesity and improved insulin resistance, vascular function, and cardiac hypertrophy, indicating its preventive potential in obesity and metabolic syndrome.
INTRODUCTION
The increasing prevalence of obesity and metabolic syndrome in developing countries has resulted in increased morbidity and mortality due to cardiovascular diseases.1) Metabolic syndrome is a complex condition defined by certain risk factors such as abnormal body mass index (BMI), waist circumference, fasting plasma glucose, blood pressure and serum lipids.2) Despite the proposed genetic and environmental factors that predispose individuals to weight gain, the fundamental cause of obesity is an imbalance between dietary intake and energy consumption.
There are a good number of functional foods that have been shown to improve energy balance in a manner that successfully reduces weight.3) Green tea (Camellia sinensis) is a very popular drink in Asia and contains high concentrations of polyphenolic compounds known as green tea catechins (GTCs). Reportedly, green tea exerts anti-obesity effects in animal and human subjects.2,4) Notably, the consumption of green tea is associated with reduced levels of body fat and waist circumference,5,6) and a lower risk of cardiovascular disease associated mortality.7) So far, (−)-epigallocatechin-3-gallate (EGCG) is the abundant and well-studied GTC. Kosen-cha is prepared from green tea using a high pressure process to reduce the astringent taste associated with green tea. The extracts prepared in this manner contains fewer GTCs, which have an astringent taste, and more polymerized catechins than regular green tea.8) Polymerized polyphenol-enriched oolong tea is reported to suppress postprandial serum triglyceride (TG) elevation after a high-fat meal.9) However, the effects of kosen-cha, containing polymerized GTCs, on obesity and metabolic syndrome remain unclear. In this study, we investigated the safety and effects of kosen-cha on body composition, and clinical parameters of metabolic syndrome, and cardiovascular diseases in an open-label pilot study in obese Japanese patients.
MATERIALS AND METHODS
SubjectsBefore participation in the study, informed consent was received from all subjects for inclusion. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of Shizuoka General Hospital (Project identification code: 12-09-19). This study was conducted between November 2012 and January 2013. Six obese subjects (BMI >25 kg/m2) from Shizuoka General Hospital were enrolled in the study. Screening procedures included a medical history, physical exam, hematological profile, and blood chemistry. Pregnant or breast-feeding women were excluded. All subjects maintained their regular diet and lifestyle and were requested to avoid consuming beverages and supplements that influence body composition.
Study DesignWe conducted a prospective, before-after study to investigate the safety and effects of kosen-cha in obese Japanese patients. The subjects consumed kosen-cha (333 mL/meal, equivalent to 1 L/d) for 12 weeks. Interviews and various measurements were performed on weeks 0, 4, 8, and 12 at the Shizuoka General Hospital. The height, body weight, waist circumference, serum TG, blood pressure, and plasma brain natriuretic peptide (BNP) of each subject were measured at each visit. BMI was calculated from the height and body weight. The flow-mediated dilation (FMD), brachial-ankle pulse wave velocity (baPWV), left ventricular (LV) mass index, and glucose tolerance were measured before and after 12 weeks of kosen-cha treatment. The primary endpoints were obesity-associated factors (body weight, BMI, and waist circumference) and possible adverse effects that may occur during the 12-week regimen.
Kosen-chaKosen-cha was obtained from Teacraft Corporation (Shizuoka, Japan) and prepared by exposing green tea (Camellia sinensis) to high pressure. It was provided to subjects as teabags, which they prepared (each morning) by adding a liter of boiled water to a teabag (5 g of tea leaf), followed by steeping for 10 min. The tea was consumed 3 times/d (at each meal), independent of water body requirements. The concentration and preparation method of kosen-cha used in this study was similar to that generally followed with kosen-cha preparation. GTC concentrations were determined from the HPLC analyses performed by the ECOPRO research (Shizuoka, Japan).
Blood Chemistry and HematologyBlood samples were collected from all subjects after an overnight fast for the following serum tests: aspartate aminotransferase (AST), alanine aminotransferase (ALT), lactate dehydrogenase (LD), creatine kinase (CK), amylase (AMY), total bilirubin (T-Bil), γ-glutamyltranspeptidase (γ-GTP), urine albumin (U-Alb), urea nitrogen (BUN), creatinine (Cre), estimated glomerular filtration rate (eGFR), uric acid (UA), sodium (Na), potassium (K), chlorine (Cl), total protein (TP), insulin, total cholesterol (T-CHO), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), and triglyceride (TG). Plasma glucose and BNP were also measured. White blood cell count (WBC), hemoglobin (HB), and platelet count (PLT) were measured in whole blood. These analyses were performed at the Shizuoka General Hospital.
Oral Glucose Tolerance Test (OGTT)Baseline blood samples were initially collected immediately after the overnight fast. Subjects were then administered 75 g of glucose (TRELAN-G75) purchased from Yoshindo Inc. (Toyama, Japan). Blood was collected at 30, 60, 120, and 180 min after glucose administration for the glucose tolerance test. Homeostasis model assessment as an index of insulin resistance (HOMA-IR) was calculated as follows:
Physiological TestsFMD, baPWV, and echocardiography were performed at the Shizuoka General Hospital according to the guidelines produced by appropriate societies in Japan. The values were calculated as follows:
where: IVST, interventricular septum thickness; LVID, LV internal dimension; PWT, LV posterior LV wall thickness; and BSA: body surface area.
Statistical AnalysisData are expressed as the mean ± standard deviation (S.D.). Statistical comparisons were performed using the paired t-test or one-way ANOVA followed by Dunnett’s post-hoc test. A p < 0.05 was considered significantly different. All statistical analyses were performed using GraphPad Prism version 6.0 (San Diego, CA, U.S.A.).
RESULTS
Components of Polyphenols in Kosen-chaKosen-cha was prepared by exposing green tea to high pressure, which helped reduce its astringent taste and changed the content of green tea. To determine the polyphenolic content of kosen-cha, we compared its HPLC analysis with that of regular green tea. The results are shown in Table 1. The polymerized GTC content per 100 mL was 55.9 mg in kosen-cha and 19.5 mg in regular green tea. The GTC (excluding polymerized catechin) content of kosen-cha and regular green tea was 87.1 and 142.8 mg, respectively.
Table 1. Components of Polyphenols in Green Tea and Kosen-cha
| Components | Original green tea (mg/100 mL) | Kosen-cha (mg/100 mL) |
|---|
| Total polyphenols | 162.3 | 143.0 |
| Garic acid | 0.6 | 7.7 |
| Polymerized catechin | 19.5 | 55.9 |
| Catechins | | |
| (−)-Gallocatechin | 9.4 | 19.0 |
| (−)-Epigallocatechin | 59.1 | 17.8 |
| (+)-Catechin | 1.4 | 3.0 |
| (−)-Epicatechin | 1.3 | 5.7 |
| (−)-Epigallocatechin gallate | 45.9 | 18.3 |
| (−)-Gallocatechin gallate | 3.9 | 9.6 |
| (−)-Epicatechin gallate | 8.8 | 5.4 |
| (−)-Catechin gallate | 0.7 | 0.6 |
Six obese patients aged 48 ± 10 years (BMI >25 kg/m2) were enrolled in this study after receiving written informed consent. Their demographic characteristics and dispositions are shown in Table 2. All subjects were hypertensive and were being treated with antihypertensive drugs such as Ca2+ antagonists and angiotensin-receptor blockers. These subjects were administered kosen-cha every day for 12 weeks. Kosen-cha administration resulted in no significant changes in blood pressure (Table 3), and liver and kidney functions (Table 3). These data indicate kosen-cha exhibited no significant side in the subjects.
Table 2. Demographic Characteristics of Subjects
| Age (year, mean ± S.D.) | 48 ± 10 |
| Gender, n | Male 4/Female 2 |
| Medical history | |
| Smoking, n | 1 |
| Alchol drinking, n | 4 |
| Hypertension, n | 6 |
| Diabetes mellitus, n | 3 |
| Hyperlipidemia, n | 1 |
| Hypertensive heart disease, n | 2 |
| Ischemic heart disease, n | 1 |
| Chronic kidney disease, n | 2 |
| Hyperuricemia, n | 1 |
Table 3. Safety Assessments in Subjects Taking Kosen-cha
| Before | 4 weeks | 8 weeks | 12 weeks |
|---|
| SBP (mmHg) | 134 ± 9 | 130 ± 9 | 134 ± 8 | 135 ± 5 |
| DBP (mmHg) | 84 ± 5 | 82 ± 6 | 86 ± 7 | 85 ± 5 |
| Pulse rate (rate/min) | 70 ± 7 | 75 ± 11 | 75 ± 18 | 72 ± 19 |
| WBC | 69 ± 10 | 78 ± 20 | 72 ± 15 | 80 ± 26 |
| HB (g/dL) | 14.8 ± 1 | 15.5 ± 1.2 | 15.5 ± 1.3 | 15.2 ± 1.6 |
| PLT | 23.1 ± 3.9 | 24.5 ± 3.4 | 24.7 ± 4.4 | 28.2 ± 5.7 |
| TP (g/dL) | 7.6 ± 0.3 | 7.7 ± 0.2 | 7.7 ± 0.2 | 7.7 ± 0.4 |
| Na (mmol/L) | 141 ± 1 | 140 ± 1 | 140 ± 2 | 140 ± 2 |
| K (mmol/L) | 4.1 ± 0.3 | 4.1 ± 0.3 | 4.2 ± 0.2 | 4.1 ± 0.3 |
| CL (mmol/L) | 105 ± 3 | 104 ± 2 | 104 ± 3 | 104 ± 3 |
| AST (U/L) | 24 ± 7 | 23 ± 7 | 25 ± 8 | 21 ± 5 |
| ALT (U/L) | 28 ± 9 | 28 ± 15 | 33 ± 20 | 25 ± 13 |
| LD (U/L) | 185 ± 46 | 189 ± 42 | 194 ± 43 | 187 ± 43 |
| CK (U/L) | 131 ± 103 | 179 ± 135 | 132 ± 96 | 119 ± 67 |
| AMY (pg/mL) | 56 ± 4 | 63 ± 10 | 66 ± 15 | 62 ± 10 |
| T-Bil (mg/dL) | 0.9 ± 0.3 | 0.8 ± 0.3 | 0.8 ± 0.3 | 0.9 ± 0.2 |
| γ-GTP (IU/L) | 61 ± 32 | 65 ± 32 | 76 ± 43 | 72 ± 41 |
| U-Alb (mg/dL) | 23.9 ± 36.1 | 34.7 ± 52.2 | 39.5 ± 62.6 | 19.4 ± 38.1 |
| BUN (mg/dL) | 13 ± 4 | 13 ± 3 | 12 ± 2 | 13 ± 2 |
| Cre (mg/dL) | 0.78 ± 0.12 | 0.81 ± 0.11 | 0.76 ± 0.13 | 0.73 ± 0.17 |
| eGFR (mL/min) | 78 ± 12 | 75 ± 7 | 81 ± 12 | 85 ± 15 |
| UA (mg/dL) | 6.0 ± 0.6 | 5.9 ± 0.9 | 5.8 ± 0.8 | 6.2 ± 1.1 |
Values shown are means ± standard deviation (S.D.). WBC, white blood cell; HB, hemoglobin; PLT, platelet count; TP, total protein; SBP, systolic blood pressure; DBP, diastolic blood pressure AST, aspartate aminotransferase; ALT, alanine aminotransferase; LD, lactate dehydrogenase; CK, creatine kinase; T-Bil, amylase, total bilirubin; γ-GTP, γ-glutamyltranspeptidase; BUN, urea nitrogen; Cre, creatinine; eGFR, estimated glomerular filtration rate; UA, uric acid.
Body weight, BMI, and waist circumference are important obesity indicators. We examined the effects of kosen-cha administration (4 weeks) on these 3 obesity-related measurements (Table 4). We observed that the body weights were significantly reduced by 2.2 kg (85.8 ± 11.0 vs. 83.6 ± 11.9 kg; p < 0.001), as well as the BMIs (32.4 ± 5.1 vs. 31.4 ± 5.3 kg/m2; p < 0.001) and waist circumferences (105 ± 9.1 vs. 102 ± 9.2 cm; p < 0.001).
Table 4. Effect of Kosen-cha on Body Weight, BMI and Waist Circumstance
| Before | 4 weeks | 8 weeks | 12 weeks |
|---|
| Body weight (kg) | 85.8 ± 11 | 85.1 ± 11.4 | 84.6 ± 11.2* | 83.6 ± 11.9** |
|---|
| BMI (kg/m2) | 32.4 ± 5.1 | 31.9 ± 5.3 | 31.8 ± 5.1* | 31.4 ± 5.3** |
| Waist circumstance (cm) | 105.0 ± 9.1 | 104.5 ± 9.7 | 103.7 ± 8.3* | 102.3 ± 9.2** |
Values shown are means ± S.D. BMI, body mass index. Statistical analysis is performed by Dunnett’s test. * p < 0.05, ** p < 0.001 (vs. Before).
Obesity is related to lipid metabolism, hypercholesterolemia, and hypertriglyceridemia. Dyslipidemia is one of the leading causes of severe stroke and myocardial infarction. We examined the effects of kosen-cha on lipid metabolism. T-CHO, LDL-C, and HDL-C were not altered by kosen-cha (Table 5). However, TG levels were significantly decreased (162 ± 82 vs. 135 ± 66 mg/dL; p = 0.0191; Table 5).
Table 5. Effect of Kosen-cha on Lipid Metabolism
| Before | 12 weeks | p Value |
|---|
| T-CHO (mg/dL) | 171 ± 12 | 184 ± 33 | 0.157 |
| LDL-C (mg/dL) | 103 ± 5 | 119 ± 27 | 0.101 |
| HDL-C (mg/dL) | 52 ± 7 | 53 ± 11 | 0.474 |
| TG (mg/dL) | 162 ± 82 | 135 ± 66 | 0.019 |
Values shown are means ± S.D. Statistical analysis is performed by paired t-test. T-CHO, total cholesterol; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; TG, tryglyceride.
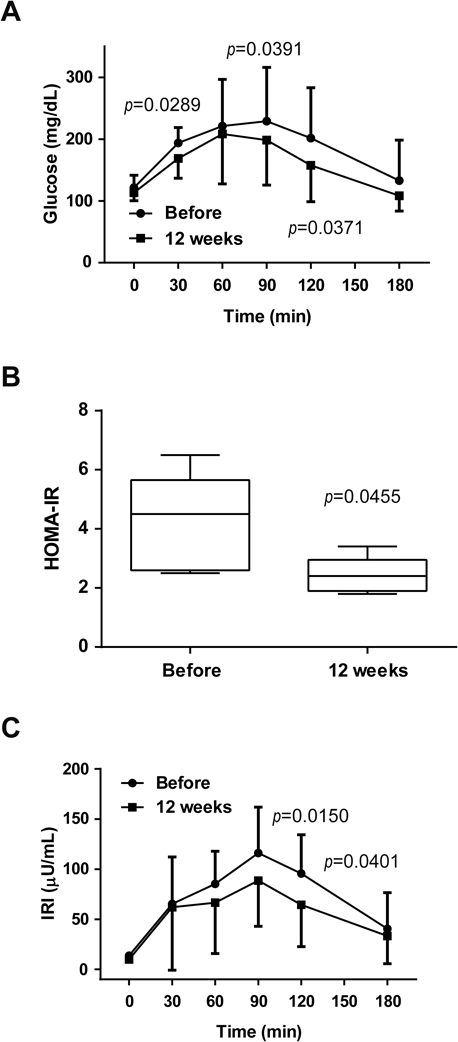
Obesity is a risk factor for type 2 diabetes. Fasting glucose and serum insulin levels were unaltered after 12 weeks of kosen-cha administration (Figs. 1A, C). However, postprandial glucose levels at 30, 90, and 120 min were significantly decreased after kosen-cha administration (30 min: p = 0.0289, 60 min: p = 0.0391, 120 min: p = 0.0371; Fig. 1A). In addition, postprandial insulin levels at 90 and 120 min decreased significantly (90 min; p = 0.0150, 120 min; p = 0.0401; Fig. 1C). Conversely, the levels of HOMA-IR, an indicator of insulin resistance, were significantly decreased (p = 0.0455; Fig. 1B). These data suggest that kosen-cha improved glucose tolerance in the evaluated subjects.
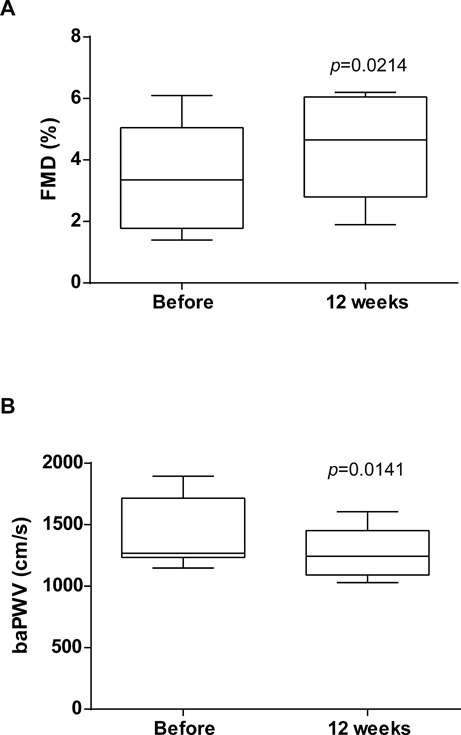
Vascular FunctionObesity is a risk factor for cardiovascular diseases such as arteriosclerosis and myocardial infarction. We examined the effects of kosen-cha on FMD and baPWV, indicators of endothelial function and vascular stiffness, respectively, in obese patients. FMD and baPWV are reportedly associated with atherosclerosis. Although the blood pressure was unchanged, the values of FMD (Fig. 2A, 3.5 ± 1.8 vs. 4.2 ± 1.7%; p = 0.0214) and baPWV (Fig. 2B, 1416 ± 292 vs. 1103 ± 562 cm/s; p = 0.0141) were significantly improved after 12-weeks of kosen-cha administration.
Cardiac HypertrophyThe effects of kosen-cha on cardiac functions were measured using echocardiography. No subject showed LV dysfunction (data not shown). LV mass index (Fig. 3A, 118.9 ± 22.1 vs. 105.6 ± 19.6 g/m2; p = 0.0120) and plasma BNP levels (Fig. 3B, 33.9 ± 13.6 vs. 11.5 ± 5.6 pg/mL; p = 0.0144), which are indicators of cardiac hypertrophy, were significantly improved after 12-weeks of kosen-cha administration.
DISCUSSION
In this study, we demonstrated the potential of kosen-cha to reduce obesity. After consuming kosen-cha for 12 weeks, plasma TG levels were decreased, and glucose tolerance, vascular endothelial functions, and cardiac hypertrophy were improved with no significant influence on biomarkers of liver and kidney functions.
Several studies in humans and animals have reported the favorable effects of green tea or GTC-rich beverages on body weight and body composition, under free-living conditions.2,5,10–14) A meta-analysis of 11 clinical trials reported that the body weight of subjects administered green tea decreased by an average of 1.31 kg compared to that of subjects in the control group, with most intervention periods being performed for approximately 12 weeks.15) In our pilot study, a 12-week kosen-cha consumption decreased body weight by an average of 2.2 kg, consistent with findings in a previous report.15) Although this study is an open-label pilot study with a small sample size, our results suggest that kosen-cha could prevent/manage obesity as efficiently as regular green tea.
Furthermore, as shown in Table 1, kosen-cha was richer in polymerized GTCs then regular green tea. Specifically, EGC and EGCG were lower in kosen-cha than regular green tea, suggesting that the polymerized catechin observed in kosen-cha results from EGC and EGCG polymerization. Given that EGC and EGCG are indicated as the main compounds responsible for the anti-obesity effect of green tea,16) the effects of kosen-cha on obesity may be dependent on both polymerized GTCs and simple GTCs. Larger polymerized catechins have a higher molecular weight and a complex structure. This complicated active compound analyses in kosen-cha. Hence, this was a limitation to this study. Advanced analytical methods for investigating the detailed mechanisms are therefore required. Previously, the high molecular weight polymerized polyphenols in oolong tea have inhibited pancreatic lipase more effectively than the oolong tea extract,17) suggesting that GTC polymerization enhanced its anti-obesity effect. The mechanism by which simple GTC exerts its anti-obesity effects is actively being researched. Notably, in humans, the sympathetic nervous system is thought to mediate the enhancement of energy expenditure.18,19) Our results and those previous reports suggest that the anti-obesity effect of kosen-cha depends on the suppression of lipid and sugar absorption from the intestines by polymerized GTCs, and the enhanced energy expenditure by simple GTCs in blood and tissues.
In our pilot study, the results suggested that kosen-cha improved serum TG levels and insulin resistance, but LDL-C, HDL-C and fasting blood glucose levels were unaltered. The weight loss and maintenance improved the parameters associated with metabolic syndrome,20,21) indicating that the effects of kosen-cha on these factors are partially dependent on decreased obesity. Green tea consumption has been shown to reduce TG levels in some clinical trials.4,22–24) Furthermore, Ikeda et al. reported that the green tea extract inhibits pancreatic lipase and TG absorption in the intestines.25) Hence, it could be postulated that pancreatic lipase and TG absorption were equally suppressed by polymerized and/or simple GTCs in kosen-cha. A network meta-analysis has reported that green tea consumption may decrease fasting blood glucose and showed its limited effects on 2 h postprandial glucose levels in 75 g OGTT and HOMA-IR.26) Bogdanski et al. reported that green tea extracts improved the parameters associated with insulin resistance, including HOMA-IR in obese and hypertensive patients.27) Although the mechanisms of action of polymerized GTCs have not been elucidated, polymerized polyphenols reportedly suppressed intestinal sugar absorption. Increased polymerization of polyphenols seems to increase the effect on sugar and lipid absorption in the intestine; owing to the higher molecular weight, it is not absorbed. Notably, some studies have elucidated the mechanism by which GTCs improve insulin resistance and sensitivity. Ortsäter et al. indicated that EGCG preserves the islet structure and enhances glucose tolerance in db/db mice.28) Additionally, Ueda et al. reported that EGCG promotes glucose transporter-4 translocation in the skeletal muscle.29) These reports suggest that simple GTCs may improve insulin resistance utilizing the above mechanisms.
Obesity and its related metabolic syndrome predispose patients to cardiovascular diseases.30) It has been shown that green tea consumption reduces cardiovascular disease-induced mortality.7) Previously, studies have indicated that green tea consumption decreases the risk of cardiovascular diseases in humans.7,10) In this study, we examined the effects of kosen-cha on vascular endothelial functions and LV hypertrophy, demonstrating a significant improvement in response to kosen-cha. Given that kosen-cha significantly decreased obesity, which is associated with vascular function and cardiac remodeling,31,32) an improvement in these parameters may be partially dependent on obesity and the related syndromes. Moreover, it is possible that GTCs in kosen-cha exhibit obesity-independent effects in cardiovascular diseases. Reportedly, GTCs have improved endothelial dysfunction and atherosclerosis via inhibiting vascular inflammation and reducing oxidative stress.33)
Several studies have demonstrated the mechanism of action of polyphenols in cardiac hypertrophy and heart failure including anti-inflammatory, antioxidant, and direct effects on cardiomyocytes. Notably, Yoshino et al. reported that the antioxidant activity of kosen-cha is similar to that observed with original green tea.34) Hence, the antioxidant effect could be postulated as the mechanism of action. However, as these processes and causes are complex, especially in humans, detailed mechanisms of action of polymerized and simple GTCs have not been elucidated. Further studies are necessary to investigate the mechanisms by which GTCs in kosen-cha improve cardiac hypertrophy.
Kosen-cha, which contains large quantities of polymerized GTCs, reduced obesity, improved insulin resistance, vascular functions, and cardiac hypertrophy in humans. These effects may be attributed to weight maintenance and/or the direct effects of the polymerized and simple GTCs on target organs. Like other green teas,4,7,26) the administration of kosen-cha showed no significant adverse effects. Although further studies (especially randomized controlled trials) are required to demonstrate the anti-obesity effects of kosen-cha and its polymerized catechins, and to clarify its detailed mechanisms of action, this pilot study, for the first time, indicates the beneficial effects of kosen-cha on obesity and metabolic syndrome. These findings suggest the possibility that drinking kosen-cha could prevent obesity and improve the QOL.
Acknowledgments
This study was supported by TEA CRAFT Co., Ltd., and a Grant for specially promoted research by the University of Shizuoka.
Conflict of Interest
Tatsuya Morimoto, Yasufumi Katanasaka and Yoichi Sunagawa received a research Grant from TEA CRAFT.
REFERENCES
- 1) Kenchaiah S, Evans JC, Levy D, Wilson PW, Benjamin EJ, Larson MG, Kannel WB, Vasan RS. Obesity and the risk of heart failure. N. Engl. J. Med., 347, 305–313 (2002).
- 2) Sae-tan S, Grove KA, Lambert JD. Weight control and prevention of metabolic syndrome by green tea. Pharmacol. Res., 64, 146–154 (2011).
- 3) Bray GA. Lifestyle and pharmacological approaches to weight loss: efficacy and safety. J. Clin. Endocrinol. Metab., 93 (Suppl. 1), S81–S88 (2008).
- 4) Maki KC, Reeves MS, Farmer M, Yasunaga K, Matsuo N, Katsuragi Y, Komikado M, Tokimitsu I, Wilder D, Jones F, Blumberg JB, Cartwright Y. Green tea catechin consumption enhances exercise-induced abdominal fat loss in overweight and obese adults. J. Nutr., 139, 264–270 (2009).
- 5) Wang H, Wen Y, Du Y, Yan X, Guo H, Rycroft JA, Boon N, Kovacs EM, Mela DJ. Effects of catechin enriched green tea on body composition. Obesity (Silver Spring), 18, 773–779 (2010).
- 6) Hursel R, Viechtbauer W, Dulloo AG, Tremblay A, Tappy L, Rumpler W, Westerterp-Plantenga MS. The effects of catechin rich teas and caffeine on energy expenditure and fat oxidation: a meta-analysis. Obes. Rev., 12, e573–e581 (2011).
- 7) Kuriyama S, Shimazu T, Ohmori K, Kikuchi N, Nakaya N, Nishino Y, Tsubono Y, Tsuji I. Green tea consumption and mortality due to cardiovascular disease, cancer, and all causes in Japan: the Ohsaki study. JAMA, 296, 1255–1265 (2006).
- 8) Yoshino K, Shimizu Y, Shimizu A. Kosencha, a novel processed tea. New Food Industry, 57, 1–10 (2015).
- 9) Toyoda-Ono Y, Yoshimura M, Nakai M, Fukui Y, Asami S, Shibata H, Kiso Y, Ikeda I. Suppression of postprandial hypertriglyceridemia in rats and mice by oolong tea polymerized polyphenols. Biosci. Biotechnol. Biochem., 71, 971–976 (2007).
- 10) Nagao T, Meguro S, Hase T, Otsuka K, Komikado M, Tokimitsu I, Yamamoto T, Yamamoto K. A catechin-rich beverage improves obesity and blood glucose control in patients with type 2 diabetes. Obesity (Silver Spring), 17, 310–317 (2009).
- 11) Nagao T, Komine Y, Soga S, Meguro S, Hase T, Tanaka Y, Tokimitsu I. Ingestion of a tea rich in catechins leads to a reduction in body fat and malondialdehyde-modified LDL in men. Am. J. Clin. Nutr., 81, 122–129 (2005).
- 12) Belza A, Frandsen E, Kondrup J. Body fat loss achieved by stimulation of thermogenesis by a combination of bioactive food ingredients: a placebo-controlled, double-blind 8-week intervention in obese subjects. Int. J. Obes. (Lond.), 31, 121–130 (2007).
- 13) Nagao T, Hase T, Tokimitsu I. A green tea extract high in catechins reduces body fat and cardiovascular risks in humans. Obesity (Silver Spring), 15, 1473–1483 (2007).
- 14) Auvichayapat P, Prapochanung M, Tunkamnerdthai O, Sripanidkulchai BO, Auvichayapat N, Thinkhamrop B, Kunhasura S, Wongpratoom S, Sinawat S, Hongprapas P. Effectiveness of green tea on weight reduction in obese Thais: a randomized, controlled trial. Physiol. Behav., 93, 486–491 (2008).
- 15) Hursel R, Viechtbauer W, Westerterp-Plantenga MS. The effects of green tea on weight loss and weight maintenance: a meta-analysis. Int. J. Obes. (Lond.), 33, 956–961 (2009).
- 16) Meydani M, Hasan ST. Dietary polyphenols and obesity. Nutrients, 2, 737–751 (2010).
- 17) Nakai M, Fukui Y, Asami S, Toyoda-Ono Y, Iwashita T, Shibata H, Mitsunaga T, Hashimoto F, Kiso Y. Inhibitory effects of oolong tea polyphenols on pancreatic lipase in vitro. J. Agric. Food Chem., 53, 4593–4598 (2005).
- 18) Rains TM, Agarwal S, Maki KC. Antiobesity effects of green tea catechins: a mechanistic review. J. Nutr. Biochem., 22, 1–7 (2011).
- 19) Wang S, Moustaid-Moussa N, Chen L, Mo H, Shastri A, Su R, Bapat P, Kwun I, Shen CL. Novel insights of dietary polyphenols and obesity. J. Nutr. Biochem., 25, 1–18 (2014).
- 20) Shibata R, Ouchi N, Ito M, Kihara S, Shiojima I, Pimentel DR, Kumada M, Sato K, Schiekofer S, Ohashi K, Funahashi T, Colucci WS, Walsh K. Adiponectin-mediated modulation of hypertrophic signals in the heart. Nat. Med., 10, 1384–1389 (2004).
- 21) Ouchi N, Parker JL, Lugus JJ, Walsh K. Adipokines in inflammation and metabolic disease. Nat. Rev. Immunol., 11, 85–97 (2011).
- 22) Chu SL, Fu H, Yang JX, Liu GX, Dou P, Zhang L, Tu PF, Wang XM. A randomized double-blind placebo-controlled study of Pu’er tea extract on the regulation of metabolic syndrome. Chin. J. Integr. Med., 17, 492–498 (2011).
- 23) Suliburska J, Bogdanski P, Szulinska M, Stepien M, Pupek-Musialik D, Jablecka A. Effects of green tea supplementation on elements, total antioxidants, lipids, and glucose values in the serum of obese patients. Biol. Trace Elem. Res., 149, 315–322 (2012).
- 24) Belcaro G, Ledda A, Hu S, Cesarone MR, Feragalli B, Dugall M. Greenselect phytosome for borderline metabolic syndrome. Evid. Based Complement. Alternat. Med., 2013, 869061 (2013).
- 25) Ikeda I, Tsuda K, Suzuki Y, Kobayashi M, Unno T, Tomoyori H, Goto H, Kawata Y, Imaizumi K, Nozawa A, Kakuda T. Tea catechins with a galloyl moiety suppress postprandial hypertriacylglycerolemia by delaying lymphatic transport of dietary fat in rats. J. Nutr., 135, 155–159 (2005).
- 26) Kondo Y, Goto A, Noma H, Iso H, Hayashi K, Noda M. Effects of coffee and tea consumption on glucose metabolism: a systematic review and network meta-analysis. Nutrients, 11, 48 (2018).
- 27) Bogdanski P, Suliburska J, Szulinska M, Stepien M, Pupek-Musialik D, Jablecka A. Green tea extract reduces blood pressure, inflammatory biomarkers, and oxidative stress and improves parameters associated with insulin resistance in obese, hypertensive patients. Nutr. Res., 32, 421–427 (2012).
- 28) Ortsäter H, Grankvist N, Wolfram S, Kuehn N, Sjoholm A. Diet supplementation with green tea extract epigallocatechin gallate prevents progression to glucose intolerance in db/db mice. Nutr. Metab. (Lond.), 9, 11 (2012).
- 29) Ueda M, Nishiumi S, Nagayasu H, Fukuda I, Yoshida K, Ashida H. Epigallocatechin gallate promotes GLUT4 translocation in skeletal muscle. Biochem. Biophys. Res. Commun., 377, 286–290 (2008).
- 30) Bozkurt B, Aguilar D, Deswal A, Dunbar SB, Francis GS, Horwich T, Jessup M, Kosiborod M, Pritchett AM, Ramasubbu K, Rosendorff C, Yancy C. Contributory risk and management of comorbidities of hypertension, obesity, diabetes mellitus, hyperlipidemia, and metabolic syndrome in chronic heart failure: a scientific statement from the American Heart Association. Circulation, 134, e535–e578 (2016).
- 31) Hannukainen JC, Lautamaki R, Parkka J, Strandberg M, Saunavaara V, Hurme S, Soinio M, Dadson P, Virtanen KA, Gronroos T, Forsback S, Salminen P, Iozzo P, Nuutila P. Reversibility of myocardial metabolism and remodelling in morbidly obese patients 6 months after bariatric surgery. Diabetes Obes. Metab., 20, 963–973 (2018).
- 32) Wycherley TP, Brinkworth GD, Keogh JB, Noakes M, Buckley JD, Clifton PM. Long-term effects of weight loss with a very low carbohydrate and low fat diet on vascular function in overweight and obese patients. J. Intern. Med., 267, 452–461 (2010).
- 33) Oyama J, Maeda T, Kouzuma K, Ochiai R, Tokimitsu I, Higuchi Y, Sugano M, Makino N. Green tea catechins improve human forearm endothelial dysfunction and have antiatherosclerotic effects in smokers. Circ. J., 74, 578–588 (2010).
- 34) Yoshino K, Sugimoto N, Shiokawa A, Yoshino H, Goto K, Shimizu A. Antioxidant activity of polyphenolic components in Kosencha. J Technology and Education, 25, 37–45 (2018).