Abstract
To prevent cognitive decline, non-pharmacological therapies such as reminiscence for mild cognitive impairment (MCI) are required, however, the use of nursing homes was limited due to coronavirus disease 2019 (COVID-19). Therefore, the demand for remote-care is increasing. We hypothesized that immersive virtual reality (iVR) could be used more effectively than conventional reminiscence for anxiety. We first examined the effectiveness and safety of reminiscence using iVR (iVR reminiscence session) in patients with MCI. After COVID-19 imposed restriction on visiting nursing homes, we conducted online iVR reminiscence session (remote iVR reminiscence session) and compared its effectiveness with that of interpersonal iVR reminiscence session (face-to-face iVR reminiscence session). The results of two elderly with MCI suggested that iVR reminiscence could reduce anxiety and the burden of care without serious side effects. The effects of remote iVR reminiscence might be almost as effective as those of face-to-face one.
INTRODUCTION
Dementia is a major global problem. Non-pharmacological therapies in the treatment of dementia are becoming increasingly important now and one of the most common of them is reminiscence.1,2) Sustained reminiscence in nursing homes has been shown to reduce cognitive decline, anxiety and depression.2) However, the coronavirus disease 2019 (COVID-19) has significantly decreased the opportunities for social interaction among the elderly, which has led to loneliness and, in turn, worsening psychiatric symptoms including cognitive decline, depression and anxiety.3) Therefore, there is an urgent need to develop new care methods useful even in the COVID-19 era.
A new non-pharmacological approach, digital therapeutics (DTx), which is a treatment using digital technologies such as the internet of things and virtual reality (VR), which has high affinity with remote medical care. Demand for DTx has skyrocketed worldwide as a means of preventing the spread of infection, while at the same time not compromising the quality of medical care.4,5) Recently, we found that various physical and mental symptoms such as pain, anxiety, and depression were improved in terminal cancer patients by reminiscing about memorable places using immersive VR (iVR).6) Therefore, we hypothesized that the three-dimensional (3D) environment of iVR, may provide a more realistic experience than the 2D environment provided by tablets or PCs, enabling more effective reminiscence. In this study, we first aimed to examine the effectiveness for anxiety, and safety of reminiscence using iVR (iVR reminiscence session) in patients with mild cognitive impairment (MCI) as a case study. After COVID-19 imposed restriction on visiting nursing homes, we conducted online iVR reminiscence session (remote iVR reminiscence session) and compared with that of interpersonal iVR reminiscence session (face-to-face iVR reminiscence session) to reveal the effectiveness for remote iVR reminiscence session.
MATERIALS AND METHODS
Subjects and Study DesignThis was a case series with two subjects and was conducted from February to April 2020. The eligible criteria for the subjects were those aged ≥65 years, using the day service of a nursing home, suspected to have MCI (Mini-Mental State Examination Japanese version (MMSE-J) scores ranging from 24 to 277)), and were able to obtain the cooperation of their families for the assessment using the questionnaire. The exclusion criteria were those who were <65 years, had an MMSE-J score ≤23 or ≥28, were visually impaired, were unable to move their upper extremities on their own volition because of severe paralysis or numbness, had severe cognitive decline and unable to answer the questionnaire, or were deemed unsuitable for participation in the study by the principal investigator.
EvaluationThe participants’ anxiety was assessed using the State-Trait Anxiety Inventory (STAI)8,9) Japanese version. The degree of side effects (nausea, dizziness, and headache) and satisfaction with the iVR reminiscence session were also assessed using the Numerical Rating Scale (NRS). The burden of care was assessed using the short and Japanese version of the Zarit Caregiver Burden Interview (J-ZBI_8)10) and Dementia Behavior Disturbance Scale (DBD13).11) The subjects’ motivation was also assessed using the apathy scale.12) The attitude toward participation in the study was assessed using the Tokyo University Style Observation Rating Scale (TORS)13) and Pittsburgh Rehabilitation Participation Scale (PRPS)14) from filmed of the subjects taken during the iVR reminiscence sessions. If subjects showed any unusual behavior, such as agitation, within 1 week of the date of iVR reminiscence session, the nursing home staff recorded the date, time, and condition and informed the principal investigator.
Implementation of Face-to-Face iVR Reminiscence SessionPrior to the implementation of this study, the VR operators were instructed by a researcher who had a lot of experience in using VR in the medical field6,15) and had sufficient rehearsal. After confirming that there was no problem in the VR operation technique, this study was started. At this time, the researchers involved in the intervention consisted of pharmacists, an occupational therapist, a clinical psychologist, a certified psychologist and a pharmacy student. Conducted in the presence of the researchers, the subjects experienced the iVR reminiscence session one by one. Two VR headsets (Oculus Go, Facebook Technologies, CA, U.S.A.) were used. First, using one headset (for the researcher), the researcher asked the subject to describe their memorable places, and then used an app that can view Google map street view (Wander, Parkline Interactive, LLC, Boston, MA, U.S.A.) to search for the place they wanted to visit. Next, to share the images in the VR headset and enable a smooth VR experience without the subject having to operate the app, we launched Wander on the second headset (for the subject) and synchronized the images in both headsets by running the multiplayer mode. The subjects’ headset images were mirrored to a tablet PC so that the researchers and nursing home staff could also share the images with them. The subjects then put on the VR headset and experienced a virtual trip for 10 min. The schedule of the iVR reminiscence sessions and various assessments performed in this study are shown in Fig. 1A.
Implementation of Remote iVR Reminiscence SessionFigures 1B and C show a framework of remote iVR reminiscence session and the practice of it, respectively. We used two headsets and the travel app Wander as well as the face-to-face iVR reminiscence session. We used a web conferencing service (Zoom, Zoom Video Communications, Inc., CA, U.S.A.) to connect a tablet PC set up in a nursing home with each of the three researchers to conduct real-time group conversations. To reduce the burden on nursing home staff, the tablet PCs at the nursing home were remotely controlled by researchers using a remote connection tool (TeamViewer, TeamViewer AG, Goeppingen, Germany) to connect to the zoom session and mirror the video in the VR headset to the tablet PC.
The iVR Reminiscence and Various Evaluation SchedulesBefore the start of the first iVR reminiscence session, the subjects were evaluated using the MMSE-J, apathy scale, J-ZBI_8, DBD13, the autonomic nervous system, and electroencephalography (EEG). MMSE-J and apathy scale were answered by the subject themselves, and the J-ZBI_8 and DBD13 were answered by the subjects’ families. Subjects then underwent weekly iVR reminiscence sessions, with anxiety assessed by the STAI before and after each session, and satisfaction and side effects (nausea, dizziness, and headache) assessed by the NRS after iVR reminiscence sessions. One month after the participating in this study, the subject responded to the apathy scale, and subjects’ family members responded to the J-ZBI_8 and DBD13. The occupational therapist also assessed the TORS and PRPS from the video of each session. Subjects 1 and 2 experienced 6- and 8-times face-to-face iVR reminiscence sessions, respectively, and after that, both experienced remote iVR reminiscence session once. The STAI sharply reflects the anxiety of the moment, it is possible that the degree of anxiety would be different day by day during the situation regarding the COVID-19 was dramatically changing. Therefore, we thought it would be appropriate to compare the effectiveness of remote iVR reminiscence session with last face-to-face iVR reminiscence session, which is considered to be the closest to the social situation.
Primary and Secondary EndpointsThe primary endpoint was the change in total STAI scores before and after the iVR reminiscence sessions. The secondary endpoints were the difference between the various evaluation tools at the time of the final face-to-face iVR reminiscence session and the remote iVR one, the change over time in the NRS score on satisfaction and side effects after each iVR reminiscence session, and the change over time in the J-ZBI, DBD13 and apathy scale before and 1 month after the first iVR reminiscence session.
Ethical ConsiderationsThis study was conducted in accordance with the Declaration of Helsinki and the Ethical Guidelines for Medical Research Involving Human Subjects, and approved by the Research Ethics Review Committee of the Osaka Center for Cancer and Cardiovascular Disease Prevention (Approval No. R1-RINRI-9). Written informed consent was obtained from the subjects and their families. This study was registered with the University Hospital Medical Information Network Clinical Trials Registry (Registration No. UMIN000040350).
RESULTS
The background of the two subjects is shown in Table 1. In addition, subject No. 1 used octotiamine, B2, B6, and B12 combination tablets, taltirelin hydrate tablets, levodopa and carbidopa hydrate tablets, ketoprofen tape, ambroxol hydrochloride extended-release capsules, and fexofenadine orally disintegrating (OD) tablets before the intervention, but did not use any medication for anxiety. After the intervention, ambroxol hydrochloride extended-release capsules and fexofenadine OD tablets were discontinued, but there was no change in other medications. Subject No. 2 stopped using the day care, so the information on medication was not available. Both subjects were engaged in rehabilitation and learning activities such as reading, writing and calculation, which are routinely conducted at the day care, and there was no change in these activities before and after the intervention.
Table 1. Baseline Characteristics of the Subject and Assessments Results after a Month
| Subject | 1 | 2 |
|---|
| Age (years) | 80 | 92 |
| Sex | Male | Female |
| Number of interventions | 7 | 9 |
| Assessments | Baseline | After a month | Baseline | After a month |
| MMSE-J | 25 | N/A | 24 | N/A |
| Apathy scale | 19 | 17 | 8 | 17 |
| J-ZBI_8 | 17 | 9 | 14 | 13 |
| DBD13 | 7 | 4 | 7 | 6 |
| TORS | 17 | 20 | 19 | 20 |
| PRPS | 6 | 6 | 6 | 6 |
| Electroencephalography | W.N.L. | N/A | W.N.L. | N/A |
Abbreviation: N/A, not applicable; MMSE-J, Mini Mental State Examination Japanese version; STAI, State-Trait Anxiety Inventory; J-ZBI_8, Short version of the Japanese version of the Zarit Caregiver Burden Interview; DBD, Dementia Behavior Disturbance Scale; TORS, Todai-shiki Observational Rating Scale; PRPS, Pittsburgh Rehabilitation Participation Scale; W.N.L, Within Normal Limits.
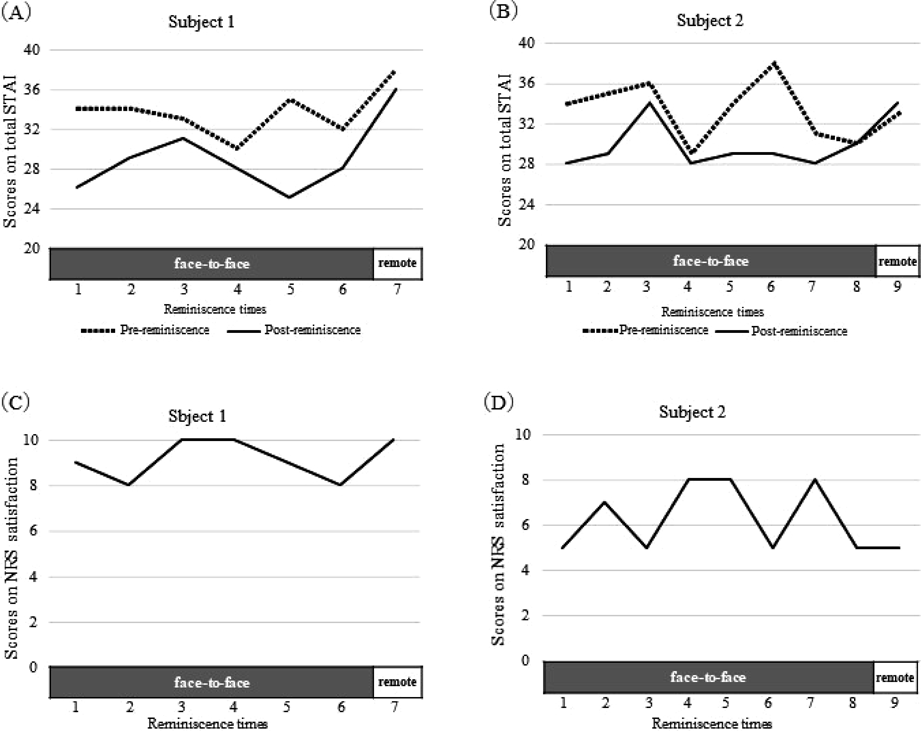
The progress of STAI scores, side effects, and satisfaction for both subjects are shown in Fig. 2. Focusing on the initial face-to-face iVR reminiscence session, the total STAI score was 34 for both subjects before the session, but, the total STAI score decreased to 26 and 28 for subjects 1 and 2, respectively after the session (Figs. 2A, B). Subsequently, subject 1 received face-to-face iVR reminiscence sessions six times, and in each case the total STAI score decreased after iVR reminiscence sessions. Subject 2 received the face-to-face iVR reminiscence sessions eight times, and in all but the eighth time, the STAI total score decreased after iVR reminiscence sessions.
Remote iVR reminiscence session was performed at the seventh intervention for subject 1 and at the ninth intervention for subject 2. The total STAI score of Subject 1 decreased by 4 points at the final face-to-face iVR reminiscence session (sixth intervention), whereas it decreased by 2 points in the remote iVR reminiscence session (Fig. 2A). For subject 2, the total STAI score did not change at the final face-to-face iVR reminiscence session (eighth intervention), whereas it increased by 1 point with remote iVR (Fig. 2B). Regarding satisfaction, subject 1 increased from 8 to 10 from the final face-to-face iVR reminiscence session (sixth intervention) to the remote iVR one, while subject 2 remained unchanged at 5 (Figs. 2C, D). The NRS scores for side effects in both subjects were 0 at all iVR reminiscence sessions regardless of being face-to-face or remote. Furthermore, there were no reports of unusual behavior within 1 week of each iVR reminiscence session. After a month, subject 1 showed a decrease in the apathy scale, J-ZBI_8 and DBD13, and an increase in TORS (Table 1). Subject 2 also showed a decrease in J-ZBI_8 and DBD13 and an increase in TORS, but an increase in the apathy scale (Table 1).
DISCUSSION
This study is the first to focus on the impact of iVR reminiscence session on anxiety in the elderly with MCI. Depression and anxiety are reported to occur more often during the MCI stage and to place a relatively large burden on caregivers.16) Before and after face-to-face iVR reminiscence session, there was a decrease in total STAI scores at many sessions: 6/6 for subject 1 and 7/8 for subject 2. The finding of a decrease in transient anxiety is consistent with the results of recent studies using iVR for cancer patients. Chirico et al.17) compared three groups of breast cancer patients: one group viewing nature images in iVR, one implementing music therapy, and a nonintervention group. They found that the total STAI score before and after each intervention decreased by 6.85 points in the iVR viewing group and by 3.33 points in the music therapy group, indicating that the iVR intervention was more effective than music therapy in reducing anxiety. Corsaletti et al.18) found that the minimal clinically important difference (MCID) for STAI was 10 points. In this study, the maximum STAI change observed in subject 1 was 10, the same as in MCID, and that in subject 2 was 9, which was greater than the STAI decrease observed in the study by Chirico et al.17) Therefore, we consider that iVR reminiscence session showed a transient anxiety-reducing effect on the elderly with MCI. Besides, there was little difference in transient anxiety reduction or satisfaction between remote and face-to-face iVR reminiscence session. In reminiscence, smooth communication is important for multiperson groups, but there was concern that the effectiveness of remote iVR reminiscence session may be diminished because of the difficulty of communication, especially in the elderly who are unfamiliar with digital devices. However, subject 1 showed a decrease in STAI scores after remote iVR reminiscence session, and his satisfaction level was higher than that of the final face-to-face iVR reminiscence session (sixth intervention). Subject 2 showed a slight increase in STAI scores after remote iVR reminiscence session, but the satisfaction level was the same as in the final face-to-face iVR reminiscence session (eighth intervention). Although the unfamiliarity of the elderly and caregivers in handling digital devises is a major obstacle to remote medical care, we enabled them to remotely control a tablet PC to increase the feasibility, thereby minimizing the burden on the nursing staff. There have been no reports on practical examples like our study, and we think that this may be a model case for future remote medical care.
In addition, iVR reminiscence session did not cause any side effects and no abnormalities. These results are consistent with recent studies examining the efficacy and safety of iVR in people aged ≥70 years.6,19)
There are some limitations. First, because it was a case series of only two cases, a well-designed study with a comparative control setting and an adequate sample size is needed. Second, the responses to the questionnaire were administered in the form of interviews with either the researcher or nursing home staff; therefore, the effect of interpersonal bias might not be avoided. Third, the number of times of face-to-face and remote iVR reminiscence sessions should have been determined in advance as part of the study design, but in this study, we could not do so because remote iVR reminiscence session was hurriedly implemented in order to provide uninterrupted care that could prevent cognitive decline while COVID-19 restricted various daily life and social activities. As for remote iVR reminiscence sessions, we had initially planned to conduct multiple sessions, but, were later forced to change the plan due to the suspension of the day care according to the declaration of a state of emergency, resulting in different number of times of iVR reminiscence sessions for each subject. However, since this is the first trial of its kind in the world, we believe that these preliminary results will contribute to the development of future researches. Fourth, the information on medication of subject No. 2 was not available.
This study suggests that iVR reminiscence session may transiently reduce anxiety in the late elderly with MCI without causing serious side effects, which may also reduce the burden of caregiving for their families. Furthermore, the results suggest that the effectiveness of remote iVR reminiscence may be comparable to that of face-to-face iVR reminiscence. Because there are barriers to the elderly’ mastery of new technology,20) future studies are required to establish useful remote treatments for the elderly and caregivers.
Acknowledgments
The authors thank all subjects and collaborators.
Conflict of Interest
The authors declare no conflict of interest.
REFERENCES
- 1) Huang HC, Chen YT, Chen PY, Hu SHL, Liu F, Kuo YL, Chiu HY. Reminiscence therapy improves cognitive functions and reduces depressive symptoms in elderly people with dementia: a meta-analysis of randomized controlled trials. J. Am. Med. Dir. Assoc., 16, 1087–1094 (2015).
- 2) Lök N, Bademli K, Selcuk-Tosun A. The effect of reminiscence therapy on cognitive functions, depression, and quality of life in Alzheimer patients: randomized controlled trial. Int. J. Geriatr. Psychiatry, 34, 47–53 (2019).
- 3) Steinman MA, Perry L, Perissinotto CM. Meeting the care needs of older adults isolated at home during the COVID-19 pandemic. JAMA Intern. Med., 180, 819–820 (2020).
- 4) Ohannessian R, Duong TA, Odone A. Global telemedicine implementation and integration within health systems to fight the COVID-19 pandemic: a call to action. JMIR Public Health Surveill., 6, e18810 (2020).
- 5) Wang SSY, Teo WZW, Teo WZY, Chai YW. Virtual reality as a bridge in palliative care during COVID-19. J. Palliat. Med., 23, 756 (2020).
- 6) Niki K, Okamoto Y, Maeda I, Mori I, Ishii R, Matsuda Y, Takagi T, Uejima E. A novel palliative care approach using virtual reality for improving various symptoms of terminal cancer patients: a preliminary prospective, multicenter study. J. Palliat. Med., 22, 702–707 (2019).
- 7) Saxton J, Morrow L, Eschman A, Archer G, Luther J, Zuccolotto A. Computer assessment of mild cognitive impairment. Postgrad. Med., 121, 177–185 (2009).
- 8) Iwata N, Mishima N, Shimizu T, Mizoue T, Fukuhara M, Hidano T, Spielberger CD. Positive and negative affect in the factor structure of the state-trait anxiety inventory for Japanese workers. Psychol. Rep., 82, 651–656 (1998).
- 9) Iwata N, Mishima N, Shimizu T, Mizoue T, Fukuhara M, Hidano T, Spielberger CD. The Japanese adaptation of the STAI form Y in Japanese working adults—the presence or absence of anxiety. Ind. Health, 36, 8–13 (1998).
- 10) Arai Y, Tamiya N, Yano E. The short version of the Japanese version of the Zarit Caregiver Burden Interview (J-ZBI_8): its reliability and validity. Nippon Ronen Igakkai Zasshi, 40, 497–503 (2003).
- 11) Machida A. Estimation of the reliability and validity of the short version of the 28-item dementia behavior disturbance scale. Nippon Ronen Igakkai Zasshi, 49, 463–467 (2012).
- 12) Okada K, Kobayashi S, Aoki K, Suyama N, Yamaguchi S. Assessment of motivational less in poststroke patients using the Japanese version of Starkstein’s apathy scale. Jpn. J. Stroke, 20, 318–323 (1998).
- 13) Matsuda O, Kurokawa Y, Saito M, Maruyama K, Miyamoto N. Interrater reliability of the Todai-shiki Observational Rating Scale (TORS) for group psychotherapy of elderly patients with dementia. Psychogeriatrics, 1, 133–138 (2001).
- 14) Lenze EJ, Munin MC, Quear T, Dew MA, Rogers JC, Begley AE, Reynolds CF 3rd. The Pittsburgh Rehabilitation Participation Scale: reliability and validity of a clinician-rated measure of participation in acute rehabilitation. Arch. Phys. Med. Rehabil., 85, 380–384 (2004).
- 15) Niki K, Yasui M, Iguchi M, Isono T, Kageyama H, Ueda M. A pilot study to develop a new method of assisting children in taking their medication by using immersive virtual reality. Biol. Pharm. Bull., 44, 279–282 (2021).
- 16) Black W, Almeida OP. A systematic review of the association between the behavioral and psychological symptoms of dementia and burden of care. Int. Psychogeriatr., 16, 295–315 (2004).
- 17) Chirico A, Maiorano P, Indovina P, Milanese C, Giordano GG, Alivernini F, Iodice G, Gallo L, De Pietro G, Lucidi F, Botti G, De Laurentiis M, Giordano A. Virtual reality and music therapy as distraction interventions to alleviate anxiety and improve mood states in breast cancer patients during chemotherapy. J. Cell. Physiol., 235, 5353–5362 (2020).
- 18) Corsaletti B, Proença M, Bisca G, Leite J, Bellinetti L, Pitta F. Minimal important difference for anxiety and depression surveys after intervention to increase daily physical activity in smokers. Fisioter. Pesqui., 21, 359–364 (2014). ‹http://www.scielo.br/j/fp/a/kVFcRJLNhb7j5Gzb6WFFj3q/abstract/?lang=en›
- 19) Ferguson C, Shade MY, Blaskewicz Boron J, Lyden E, Manley NA. Virtual reality for therapeutic recreation in dementia hospice care: A feasibility study. Am. J. Hosp. Palliat. Care, 37, 809–815 (2020).
- 20) van den Berg N, Schumann M, Kraft K, Hoffmann W. Telemedicine and telecare for older patients—a systematic review. Maturitas, 73, 94–114 (2012).