Abstract
Background:
The relationship between outcome of radiofrequency catheter ablation (RFCA) for atrial fibrillation (AF) and the severity of left ventricular (LV) diastolic dysfunction in patients with hypertrophic cardiomyopathy (HCM) remains unknown.
Methods and Results:
Twenty-two HCM patients (12 female, aged 65±11 years) with paroxysmal (n=5; 23%) or persistent (n=17; 77%) AF were enrolled. LV diastolic function was evaluated according to the ratio of the mitral inflow early filling velocity to the velocity of the early medial mitral annular ascent (E/e’) measured on pulsed wave and tissue Doppler assessments in all patients. Pulmonary vein isolation was performed in all patients. A second procedure was performed in 3 patients. During a follow-up of 21±12 months, sinus rhythm was maintained in 13 of 22 patients (59%). E/e’ was significantly higher in the patients with AF recurrence than in those without (18±7 vs. 11±3; P<0.01). On Kaplan-Meier analysis the prevalence of AF recurrence was significantly higher in patients with E/e’ ≥15 (n=6) than in those with E/e’ <15 (n=16; P<0.01). On multivariate Cox regression analysis the only significant and independent predictor for AF recurrence was E/e’ (hazard ratio, 1.16; 95% confidence interval: 1.01–1.37, P=0.03).
Conclusions:
LV diastolic dysfunction evaluated using E/e’ was associated with difficulty of rhythm control after RFCA in patients with HCM and AF. (Circ J 2015; 79: 419–424)
Atrial fibrillation (AF) is the most common tachyarrhythmia in patients with hypertrophic cardiomyopathy (HCM). AF is often poorly tolerated and is associated with significant clinical deterioration in these patients.1–3
Maintenance of sinus rhythm (SR) is desirable in patients with HCM. Several studies have shown that radiofrequency catheter ablation (RFCA) of severely symptomatic AF is both a feasible and safe approach in patients with HCM.4–7
The presence and severity of left ventricular (LV) diastolic dysfunction increase the risk of AF recurrence after RFCA in patients without structural heart disease.8
In patients with HCM, severe LV diastolic dysfunction is common due to the thickened and non-compliant ventricular chambers. The relationship between the outcome of RFCA for AF in patients with HCM and the severity of LV diastolic dysfunction, however, has not been fully investigated. The purpose of this study was to evaluate the impact of LV diastolic dysfunction, as measured on ultrasonography, on the outcome of RFCA for AF in patients with HCM.
Editorial p 305
Methods
Subjects
Twenty-four consecutive Japanese patients with HCM undergoing RFCA of paroxysmal or persistent AF at the National Cerebral and Cardiovascular Center from 2009 to 2012 were reviewed. The diagnosis of HCM was based on the presence of myocardial hypertrophy in the absence of local or systemic etiology. Paroxysmal and persistent AF were defined according to the 2012 HRS/EHRA/ECAS Expert Consensus Statement on Catheter and Surgical Ablation of Atrial Fibrillation.9
Two patients in whom LV diastolic dysfunction was not evaluated on ultrasonography were excluded. Consequently, 22 HCM patients were enrolled in this study. All patients provided informed consent. All patients were on oral anticoagulant therapy maintaining a target international normalized ratio of 2–3. Transesophageal echocardiography was performed to exclude any left atrial thrombi prior to the procedure in all patients.
Echocardiography
Comprehensive 2-D and Doppler echocardiography were performed in each patient using commercially available instruments before RFCA.10,11
SR was maintained at the time of echocardiography in 15 of 22 patients. When echocardiography was performed during AF, all echocardiographic parameters were measured with an average of 3 consecutive beats. LV outflow tract (LVOT) gradient was measured with continuous-wave Doppler in the apical 3-chamber view. LVOT obstruction (LVOTO) was defined as a gradient >30 mmHg.12
LV diastolic function was evaluated as the ratio of the mitral inflow early filling velocity to the velocity of the early medial mitral annular ascent (E/e’), measured on pulsed wave and tissue Doppler.13
RFCA
The RFCA was performed under sedation with i.v. propofol. All anti-arrhythmia medication, except for amiodarone, was discontinued for at least 5 half-lives before the procedure in all patients. Two standard catheters were positioned: a 6-F catheter (St. Jude Medical, Minnetonka, MN, USA) at the His bundle region via a femoral vein, and another 6-F catheter (Japan Lifeline, Tokyo, Japan) in the coronary sinus via the right cervical vein. The transseptal procedure was performed using fluoroscopic landmarks, and 2 SL0 sheaths (St. Jude Medical) and an 8.0-F Preface sheath (Biosense Webster, Irwindale, CA, USA) were advanced into the left atrium (LA). After the transseptal procedure, a single bolus of 4,000 U heparin was given. A continuous infusion with heparinized saline was performed to maintain an activated clotting time of 300–350 s. Two 7-F decapolar circular catheters (Lasso, Biosense-Webster, Diamond Bar, CA, USA) and a 3.5-mm open irrigated tip ablation catheter (Navistar Thermocool, Biosense Webster) were inserted into the LA. We performed 3-D electroanatomical mapping (CARTO system, Biosense Webster) of the LA. Mapping was complete when all regions of the LA had been systematically sampled and when a sufficient density of points had been acquired to determine the LA chamber. After reconstruction of the LA, the volume of the LA chamber was automatically analyzed with the CARTO system. Each pulmonary vein (PV) ostium was identified on PV venography and tagged on the 3-D electroanatomical map. Two decapolar circular mapping catheters were placed inside the ipsilateral superior and inferior PV. The circumferential ablation lines, using a 3.5-mm tip irrigated catheter targeting a maximum temperature of 43℃, maximum power of 25–30 W, and infusion rate of 17 ml/min, were created at a distance from the PV ostia. The endpoint of the PV isolation was defined as the establishment of bidirectional conduction block between the LA and PV at least 30 min after successful PV isolation. Cavo-tricuspid isthmus ablation was performed at the operator’s discretion.
Post-Procedure Care and Follow-up
After the first procedure, all patients received a follow-up every 1–3 months in the outpatient clinic. Follow-up included 12-lead electrocardiogram, 24-h Holter monitoring and assessment of the current condition. Anti-arrhythmic agents were resumed when there was evidence that AF recurred during the early unstable period after the procedure. AF recurrence was defined as sustained AF lasting >1 min. AF recurrence within a 2-month period after the procedure was considered transient, and a 2-month period was applied as a blanking period. Following the blanking period, repeat RFCA was carried out in the event of a recurrence of AF or atrial tachycardia. PV isolation was assessed and further ablation delivered as necessary.
Statistical Analysis
Data were analyzed using JMP 9.0e (SAS Institute, Cary, NC, USA). Numeric data are expressed as the mean±SD. Chi-squared test or Student’s t-test was used when appropriate to test for statistical difference. P<0.05 was considered statistically significant. Receiver operating characteristic (ROC) curve analysis was used to identify the value of E/e’ predictive of AF recurrence. Event rate curves were plotted according to the Kaplan-Meier method and were analyzed with the log-rank test. Univariate Cox regression analysis was performed to identify predictors of subsequent AF recurrence. The hazard ratio (HR) and 95% confidence interval (95% CI) were defined. To confirm their independent predictive value, variables with P<0.05 were tested in a multivariate model.
Results
Patient Characteristics
Patient clinical characteristics are listed in
Table 1. Persistent AF was found in 17 patients (77.3%). Longstanding persistent AF was not included in this study. The mean duration of AF was 80±53 months. The mean of the LA diameter was 48±6 mm and the mean LA volume measured on 3-D mapping was 98±38 ml.
Table 1.
Patient Characteristics
| Variable |
Total
(n=22) |
AF recurrence
(n=9) |
Without AF
recurrence (n=13) |
P-value |
| Age (years) |
65±11 |
67±8 |
64±12 |
0.52 |
| Female |
12 (54.5) |
6 (66.7) |
6 (46.2) |
0.90 |
| Paroxysmal AF |
5 (22.7) |
2 (22.2) |
3 (23.1) |
0.96 |
| Persistent AF |
17 (77.3) |
7 (77.8) |
10 (76.9) |
0.96 |
| Duration of AF (months) |
80±53 |
107±56 |
62±45 |
0.052 |
| Family history of HCM |
4 (18.2) |
2 (22.2) |
2 (15.4) |
0.68 |
| Use of AAD |
15 (68.2) |
5 (55.6) |
10 (76.9) |
0.29 |
| Echocardiography |
| Middle LV thickness (mm) |
13±4 |
12±4 |
14±5 |
0.28 |
| LVDd (mm) |
45±6 |
47±2 |
44±2 |
0.30 |
| LVDs (mm) |
30±7 |
32±2 |
28±2 |
0.26 |
| LVEF (%) |
57±14 |
54±13 |
59±14 |
0.48 |
| E |
65±18 |
60±14 |
68±20 |
0.31 |
| e’ |
5±2 |
4±1 |
7±2 |
0.0009 |
| E/e’ |
14±6 |
18±7 |
11±3 |
0.002 |
| MR (>moderate) |
5 (22.7) |
2 (22.2) |
3 (23.1) |
0.96 |
| LVOTO (>30 mmHg) |
3 (13.6) |
3 (33.3) |
0 (0.0) |
0.03 |
| LA diameter (mm) |
48±6 |
49±5 |
46±6 |
0.20 |
| LA volume (ml)† |
98±38 |
115±41 |
86±33 |
0.08 |
| RFCA |
| Pulmonary vein isolation |
22 (100) |
9 (100) |
13 (100) |
NS |
| CTIA |
10 (45.5) |
2 (22.2) |
8 (61.5) |
0.12 |
| Second procedure |
3 (13.6) |
1 (11.1) |
2 (15.4) |
0.22 |
| Follow-up period (months) |
21±12 |
22±14 |
20±11 |
0.72 |
Data given as mean±SD or n (%). †Measured on 3-D electrophysiologic mapping. AAD, anti-arrhythmic drug; AF, atrial fibrillation; CTIA, cavo-tricuspid isthmus ablation; E, mitral inflow early filling velocity; e’, velocity of early medial mitral annular ascent; HCM, hypertrophic cardiomyopathy; LA, left atrium; LV, left ventricle; LVDd, left ventricular dimension at end-diastole; LVDs, left ventricular dimension at end-systole; LVEF, left ventricular ejection fraction; LVOTO, left ventricular outflow tract obstruction; MR, mitral regurgitation; RFCA, radiofrequency catheter ablation.
All PV were successfully isolated in all patients. The mean procedure time was 244±60 min and the total duration of the RF applications was 39±12 min. Cavo-tricuspid isthmus ablation was performed in 10 patients (45.5%). No patients received linear lesions in the LA or a complex fractionated atrial electrogram ablation. In 3 patients, a second procedure was performed for recurrence of AF. Recovered PV conduction was found and successfully eliminated with RFCA.
Effect of Recurrence
From 21±12 months after the last procedure, maintenance of SR was observed in 13 of 22 patients (59%;
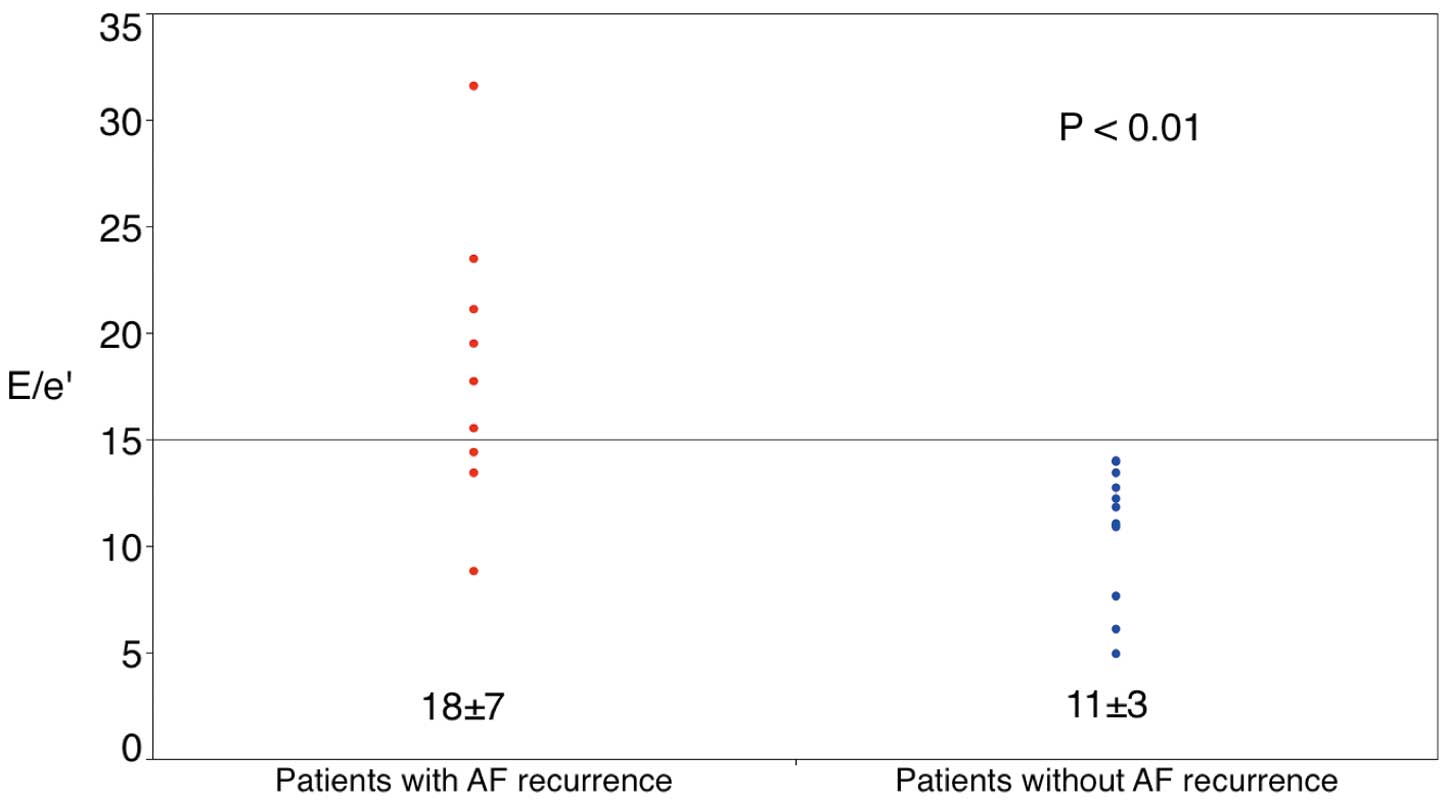
Table 1). There were no significant differences between patients with and without AF recurrence with respect to age, gender, type of AF, family history of HCM, use of anti-arrhythmic drugs, or follow-up period (Table 1). The duration of AF tended to be longer in the patients with AF recurrence than in those without (P=0.052). There were also no significant differences on echocardiography between patients with and without AF recurrence except for E/e’, e’ and number of patients with LVOTO (>30 mmHg). Compared with the patients without AF recurrence, E/e’ and number of patients with LVOTO (>30 mmHg) were significantly higher in those with an AF recurrence (18±7 vs. 11±3; P=0.002 and 3 vs. 0; P=0.03, respectively). E’ was significantly lower in those with AF recurrence (3.6±1.2 vs. 6.5±2.0; P=0.0009).
There was no significant difference in the number of cavo-tricuspid isthmus ablations during the initial RFCA and the second procedure between the patients with and without AF recurrence. LA volume measured on 3-D electroanatomical mapping tended to be larger in the patients with AF recurrence than in those without (115±41 vs. 86±33; P=0.08).
LV Diastolic Dysfunction and Outcome of RFCA
Comparison of E/e’ between the patients with and without AF recurrence is shown in
Figure 1. E/e’ was significantly higher in the patients with AF recurrence than in those without. In all 13 patients without AF recurrence, E/e’ was <15. In contrast, in 6 of 9 patents (67%) with AF recurrence, E/e’ was >15. On ROC curve analysis, the optimal threshold of E/e’ for predicting AF recurrence was 15 (sensitivity, 67%; specificity, 100%). The area under the ROC curve was 0.88.
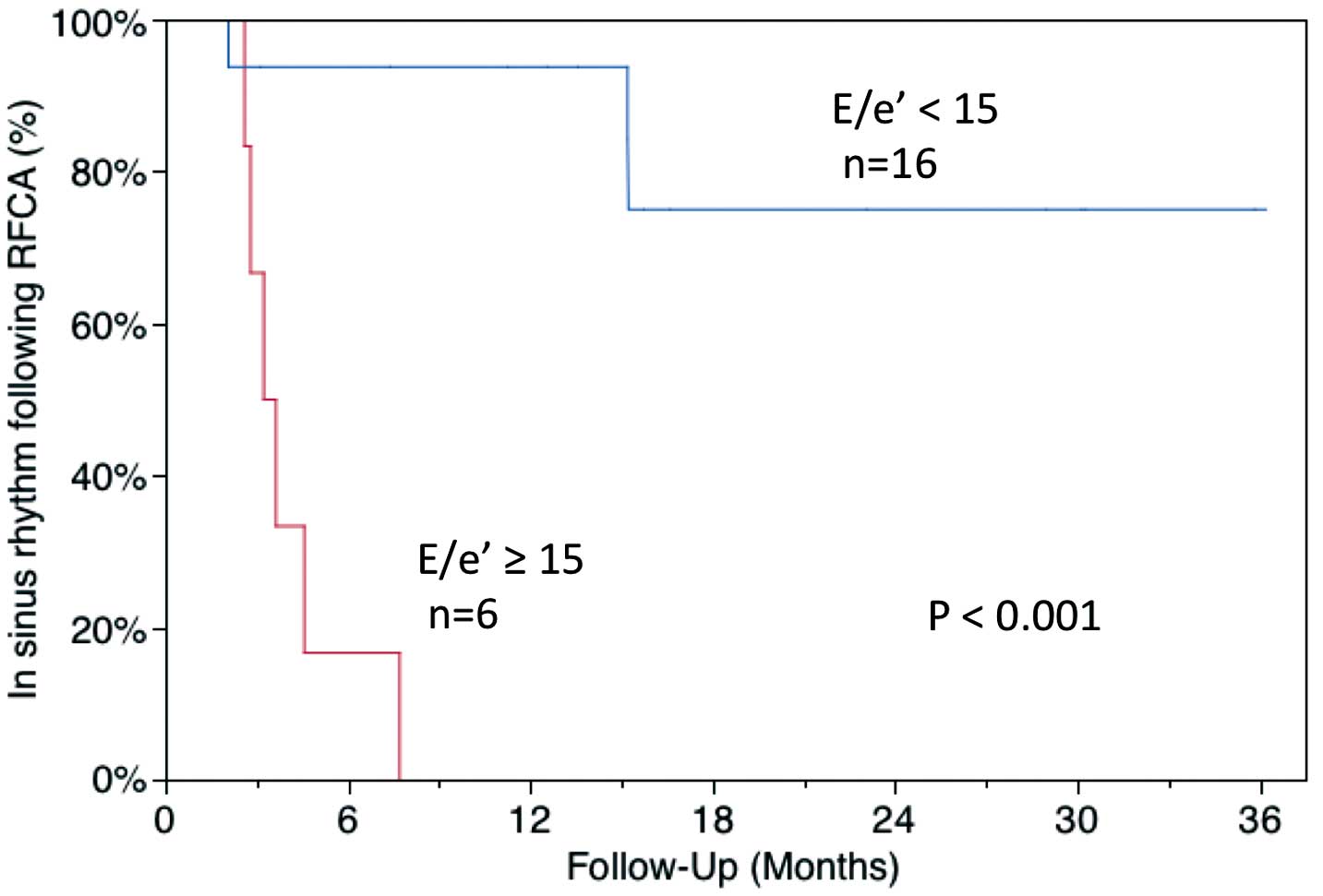
Figure 2
shows the results of Kaplan-Meier analysis of the maintenance of SR following RFCA. Patients with E/e’ ≥15 had a significantly higher risk of AF recurrence than those with E/e’ <15 (log-rank, P<0.001).
Predictors of Long-Term Outcome
The results of Cox regression analysis are shown in
Table 2. On univariate Cox regression analysis, E/e’, duration of AF and LA volume measured on 3-D electroanatomical mapping were significant predictors of AF recurrence. On multivariate Cox regression analysis E/e’ was the only predictor of AF recurrence following RFCA (HR, 1.16; 95% CI: 1.01–1.37, P=0.03).
Table 2.
Predictors of AF Recurrence
| |
Univariate |
Multivariate |
| HR (95% CI) |
P-value |
HR (95% CI) |
P-value |
| E/e’ |
1.19 (1.07–1.33) |
0.002 |
1.16 (1.01–1.37) |
0.03 |
| Duration of AF (months) |
1.02 (1.00–1.03) |
0.02 |
1.01 (0.99–1.03) |
0.40 |
| LA volume (ml)† |
1.02 (1.00–1.03) |
0.04 |
1.00 (0.98–1.02) |
0.28 |
| LA diameter (mm) |
1.14 (1.00–1.33) |
0.05 |
|
|
| LVOTO (>30 mmHg) |
3.99 (0.83–15.1) |
0.08 |
|
|
| CTIA |
0.50 (0.11–1.92) |
0.32 |
|
|
| Second procedure |
0.77 (0.04–4.28) |
0.80 |
|
|
†Measured on 3-D electrophysiologic mapping. Abbreviations as in Table 1.
Discussion
Main Findings
The major findings of the present study are as follows: (1) E/e’ was significantly higher in patients with AF recurrence than in those without; (2) patients with E/e’ ≥15 had a significantly higher risk of AF recurrence than those with E/e’ <15; and (3) E/e’ was the only predictor of AF recurrence following RFCA in the patients with HCM. To the best of our knowledge, this is the first report to describe the relationship between LV diastolic dysfunction and outcome of RFCA for AF in patients with HCM.
LV Diastolic Dysfunction and AF Recurrence
In the present study, we examined the correlation between LV diastolic dysfunction, estimated as E/e’, and outcome for AF in HCM patients. In patients with HCM, the mitral variables of E/A ratio and deceleration time of early filling velocity have weak to no correlations with LV filling pressures.14,15
But E/e’ correlated reasonably well with LV pre-A pressure during SR,15
which mean that E/e’ is a good parameter of LV diastolic function even in patients with HCM. E/e’ was significantly higher and e’ was significantly lower in patients with AF recurrence. The lower e’ reflects impaired myocardial relaxation. Severely impaired myocardial relaxation should elevate LA pressure, manifested as higher E/e’.16,17
Elevated LA pressure might result in continuous atrial remodeling after RFCA, which might explain why a higher recurrence was noted. Patients with LV diastolic dysfunction and AF have a lower LA voltage and higher recurrence rate of AF after RFCA.8,18,19
In contrast, SR was maintained in 13 of 16 patients (82%) with mild or moderate LV diastolic dysfunction (E/e’ <15). In those patients, the LA pressure might not be so high and the LA remodeling might not progress very much after RFCA for AF. The present results are in accordance with the previous reports showing that the presence and severity of LV diastolic dysfunction increased the risk of AF in patients with preserved LV systolic function.20–22
Several studies have demonstrated that RFCA of severely symptomatic AF is both a feasible and safe approach in patients with HCM.4–7
Di Donna et al found that the most important independent predictors of AF recurrence following RFCA consisted of age, functional status and LA volume.4
In that study, however, the relationship between the outcome of RFCA for AF and the severity of the LV diastolic dysfunction was not examined. Bunch et al showed that AF control following RFCA was less likely in patients with more advanced LV diastolic dysfunction.7
In the present study, LV diastolic dysfunction was graded as normal (grade 0), abnormal relaxation (grade I), pseudonormalization (grade II), restrictive (grade III), or irreversible advanced restrictive (grade IV). Although the grade of diastolic dysfunction was inversely related to the rate of AF control, this relationship did not reach statistical significance. Also, echocardiographic variables utilized to assess LV diastolic function were not associated with a reduced likelihood of AF control. The severity of LV diastolic dysfunction was not assessed in some patients due to AF during echocardiography, which might result in exclusion of the patients with severe LV diastolic dysfunction and weakening of the inverse relationship between the severity of LV diastolic dysfunction and the rate of AF control.
Clinical Implication
According to the ESC guidelines for the management of AF, RFCA for symptomatic AF refractory to pharmacological control in patients with HCM is a class IIa indication.23
At the same time, the ESC guidelines note that severe LV diastolic dysfunction is at high risk for recurrence. The appropriate candidates for RFCA in patients with HCM and AF have not been defined. We showed that outcome after RFCA was favorable in patients with mild or moderate LV diastolic dysfunction (E/e’ <15). This suggests that HCM patients with mild or moderate LV diastolic dysfunction (E/e’ <15) and AF might be good candidates for RFCA.
Study Limitations
This study had several limitations. First, this study was a retrospective study. Second, we could have underestimated the recurrence rate after RFCA for AF because asymptomatic AF recurrence could have been missed. Third, echocardiography was performed during AF in 7 of 22 patients. Although echocardiography during AF can be inaccurate, E/e’ is useful in the estimation of LV filling pressure even in patients with AF.24,25
There were no changes in LV diastolic parameters on tissue Doppler imaging following electrical cardioversion in patients with persistent AF,26
which means that these parameters were used equally in the patients with SR and AF. Fourth, this was an analysis of a small number of patients and a small number of events. Further examination is required with a larger number of patients to confirm the present results.
Conclusions
LV diastolic dysfunction evaluated on E/e’ was linked to the possibility of rhythm control after RFCA in the patients with HCM and AF. Patients with mild or moderate LV diastolic dysfunction (E/e’ <15) might be good candidates for RFCA in those with HCM and AF.
Acknowledgments
We thank Mr John Martin for the linguistic revision.
Disclosures
Funding: Nothing to disclose.
References
- 1.
Robinson K, Frenneaux MP, Stockins B, Karatasakis G, Poloniecki JD, McKenna WJ. Atrial fibrillation in hypertrophic cardiomyopathy: A longitudinal study. J Am Coll Cardiol 1990; 15: 1279–1285.
- 2.
Olivotto I, Cecchi F, Casey SA, Dolara A, Traverse JH, Maron BJ. Impact of atrial fibrillation on the clinical course of hypertrophic cardiomyopathy. Circulation 2001; 104: 2517–2524.
- 3.
Maron BJ, Olivotto I, Spirito P, Casey SA, Bellone P, Gohman TE, et al. Epidemiology of hypertrophic cardiomyopathy-related death: Revisited in a large non-referral-based patient population. Circulation 2000; 102: 858–864.
- 4.
Di Donna P, Olivotto I, Delcrè SDL, Caponi D, Scaglione M, Nault I, et al. Efficacy of catheter ablation for atrial fibrillation in hypertrophic cardiomyopathy: Impact of age, atrial remodelling, and disease progression. Europace 2010; 12: 347–355.
- 5.
Kilicaslan F, Verma A, Saad E, Themistoclakis S, Bonso A, Raviele A, et al. Efficacy of catheter ablation of atrial fibrillation in patients with hypertrophic obstructive cardiomyopathy. Heart Rhythm 2006; 3: 275–280.
- 6.
Gaita F, Di Donna P, Olivotto I, Scaglione M, Ferrero I, Montefusco A, et al. Usefulness and safety of transcatheter ablation of atrial fibrillation in patients with hypertrophic cardiomyopathy. Am J Cardiol 2007; 99: 1575–1581.
- 7.
Bunch TJ, Munger TM, Friedman PA, Asirvatham SJ, Brady PA, Cha YM, et al. Substrate and procedural predictors of outcomes after catheter ablation for atrial fibrillation in patients with hypertrophic cardiomyopathy. J Cardiovasc Electrophysiol 2008; 19: 1009–1014.
- 8.
Hu YF, Hsu TL, Yu WC, Huang SH, Tsao HM, Tai CT, et al. The impact of diastolic dysfunction on the atrial substrate properties and outcome of catheter ablation in patients with paroxysmal atrial fibrillation. Circ J 2010; 74: 2074–2078.
- 9.
Calkins H, Kuck KH, Cappato R, Brugada J, Camm AJ, Chen SA, et al. 2012 HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation: Recommendations for patient selection, procedural techniques, patient management and follow-up, definitions, endpoints, and research trial design: A report of the HRS Task Force on Catheter and Surgical Ablation of Atrial Fibrillation. Developed in partnership with the EHRA, a registered branch of the ESC and the ECAS; and in collaboration with the ACC, the AHA, the APHRS, and the STS. Endorsed by the governing bodies of the ACCF, the AHA, the ECAS, the EHRA, the STS, the APHRS, and the HRS. Heart Rhythm 2012; 9: 632–696.
- 10.
Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, et al. Recommendations for chamber quantification: A report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr 2005; 18: 1440–1463.
- 11.
Nagueh SF, Appleton CP, Gillebert TC, Marino PN, Oh JK, Smiseth OA, et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography. Eur J Echocardiogr 2009; 10: 165–193.
- 12.
Gersh BJ, Maron BJ, Bonow RO, Dearani JA, Fifer MA, Link MS, et al. 2011 ACCF/AHA guideline for the diagnosis and treatment of hypertrophic cardiomyopathy: A report of the ACCF/AHA Task Force on Practice Guidelines. Circulation 2011; 124: e783–e831, doi:10.1161/CIR.0b013e318223e2bd.
- 13.
Nagueh SF, Appleton CP, Gillebert TC, Marino PN, Oh JK, Smiseth OA, et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography. Eur J Echocardiogr 2009; 10: 165–193.
- 14.
Nishimura RA, Appleton CP, Redfield MM, Ilstrup DM, Holmes DR, Tajik AJ. Noninvasive Doppler echocardiographic evaluation of left ventricular filling pressures in patients with cardiomyopathies: A simultaneous Doppler echocardiographic and cardiac catheterization study. J Am Coll Cardiol 1996; 28: 1226–1233.
- 15.
Nagueh SF, Lakkis NM, Middleton KJ, Spencer WH, Zoghbi WA, Quiñones MA. Doppler estimation of left ventricular filling pressures in patients with hypertrophic cardiomyopathy. Circulation 1999; 99: 254–261.
- 16.
Ommen SR, Nishimura RA, Appleton CP, Miller FA, Oh JK, Redfield MM, et al. Clinical utility of Doppler echocardiography and tissue Doppler imaging in the estimation of left ventricular filling pressures: A comparative simultaneous Doppler-catheterization study. Circulation 2000; 102: 1788–1794.
- 17.
Nagueh SF, Middleton KJ, Kopelen HA, Zoghbi WA, Quiñones MA. Doppler tissue imaging: A noninvasive technique for evaluation of left ventricular relaxation and estimation of filling pressures. J Am Coll Cardiol 1997; 30: 1527–1533.
- 18.
Cha YM, Wokhlu A, Asirvatham SJ, Shen WK, Friedman PA, Munger TM, et al. Success of ablation for atrial fibrillation in isolated left ventricular diastolic dysfunction: A comparison to systolic dysfunction and normal ventricular function. Circ Arrhythm Electrophysiol 2011; 4: 724–732.
- 19.
Lee JS, Shim CY, Wi J, Joung B, Ha JW, Lee MH, et al. Left ventricular diastolic function is closely associated with mechanical function of the left atrium in patients with paroxysmal atrial fibrillation. Circ J 2013; 77: 697–704.
- 20.
Jaïs P, Peng JT, Shah DC, Garrigue S, Hocini M, Yamane T, et al. Left ventricular diastolic dysfunction in patients with so-called lone atrial fibrillation. J Cardiovasc Electrophysiol 2000; 11: 623–625.
- 21.
Tsang TSM, Gersh BJ, Appleton CP, Tajik AJ, Barnes ME, Bailey KR, et al. Left ventricular diastolic dysfunction as a predictor of the first diagnosed nonvalvular atrial fibrillation in 840 elderly men and women. J Am Coll Cardiol 2002; 40: 1636–1644.
- 22.
Tsang TSM, Barnes ME, Gersh BJ, Bailey KR, Seward JB. Risks for atrial fibrillation and congestive heart failure in patients >/=65 years of age with abnormal left ventricular diastolic relaxation. Am J Cardiol 2004; 93: 54–58.
- 23.
Camm AJ, Kirchhof P, Lip GYH, Schotten U, Savelieva I, Ernst S, et al. Guidelines for the management of atrial fibrillation: The Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC). Eur Heart J 2010; 31: 2369–2429.
- 24.
Sohn DW, Song JM, Zo JH, Chai IH, Kim HS, Chun HG, et al. Mitral annulus velocity in the evaluation of left ventricular diastolic function in atrial fibrillation. J Am Soc Echocardiogr 1999; 12: 927–931.
- 25.
Wada Y, Murata K, Tanaka T, Nose Y, Kihara C, Uchida K, et al. Simultaneous Doppler tracing of transmitral inflow and mitral annular velocity as an estimate of elevated left ventricular filling pressure in patients with atrial fibrillation. Circ J 2012; 76: 675–681.
- 26.
Melek M, Birdane A, Goktekin O, Ata N, Celik A, Kilit C, et al. The effect of successful electrical cardioversion on left ventricular diastolic function in patients with persistent atrial fibrillation: A tissue Doppler study. Echocardiography 2007; 24: 34–39.