Editorials
Plasma MicroRNA-100 as a Biomarker of Coronary Plaque Vulnerability
– A New Generation of Biomarker for Developing Acute Coronary Syndrome –
2015 年 79 巻 2 号 p. 303-304


詳細
2015 年 79 巻 2 号 p. 303-304
MicroRNAs (miRNAs) are single-stranded and short noncoding RNAs, typically 19–23 nucleotides in length, generated from endogenous transcripts.1,2 MiRNAs hybridize to mRNAs, resulting in negative regulation of target mRNA stability or translational inhibition of targeted transcripts, and are therefore considered as a key regulator of gene expression.1 To date, more than 1,000 human miRNAs have been identified, and many are suggested to have important roles in a variety of physiological and pathological processes, such as development, differentiation, cell proliferation, apoptosis, and stress responses.2 A growing body of evidence over the past few years suggests the importance of miRNAs in the onset of various diseases such as cancer, neurological diseases, immune diseases and cardiovascular diseases.3 Several studies have begun focusing on miRNAs in the pathogenesis of cardiovascular disease. Recently, we identified a set of 5 miRNAs involved in the reduced catecholamine sensitivity of mildly symptomatic patients with congestive heart failure,4 which shed light on the potential of miRNAs to provide possible etiologic insights as well as therapeutic targets for congestive heart failure.
Article p 413
In addition to being new therapeutic targets, circulating miRNAs has shown great promise as novel biomarkers for cardiovascular disease. Previous reports5–7 indicate that plasma levels of specific miRNAs correlate with arteriosclerotic disease, including acute coronary syndrome (ACS) (Figure). The plasma levels of endothelial cell-related miRNA-17, miRNA-92a and miRNA-126, and inflammatory cell-related miRNA-155 are significantly decreased in patients with coronary artery disease (CAD) compared with healthy subjects.6 In addition, the smooth muscle-enriched miRNA-145 was significantly decreased, and cardiac muscle-enriched microRNAs (miR-133a, miR-208a) tended to be higher in patients with CAD.6 Likewise, myocardium-related miRNA-1, miRNA-208, miR-499, miR-663b and miR-1291, as well as smooth muscle-related miRNA-30 and miRNA-145 were evaluated as circulating biomarkers for acute myocardial infarction.7 However, little is known about the relationship between plasma miRNAs and vulnerable coronary plaque. There is only one report showing that the expression of miR-146a in peripheral blood mononuclear cells was significantly increased in patients with ACS.8
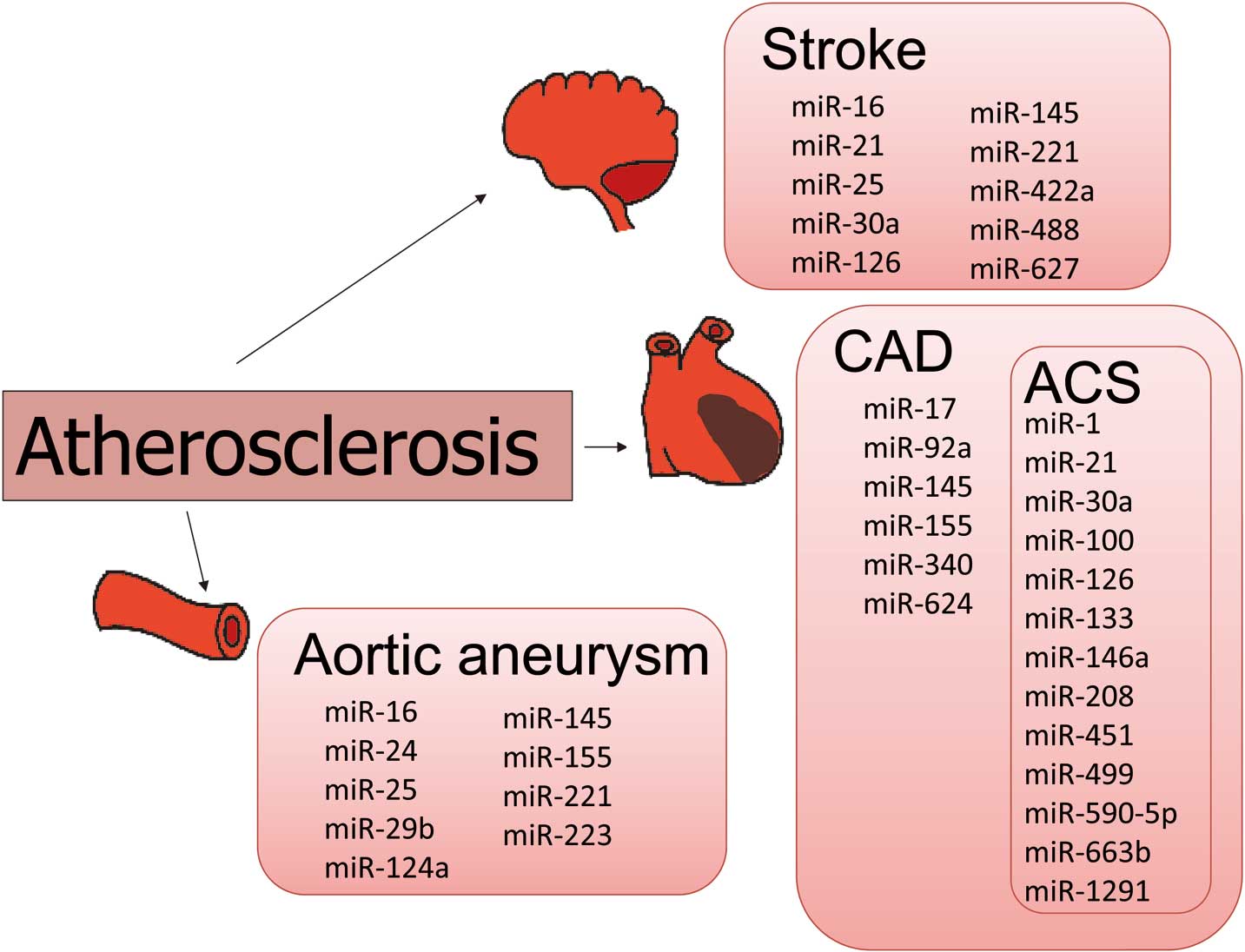
Circulating microRNAs as possible candidate biomarkers in various cardiovascular diseases. ACS, acute coronary syndrome; CAD, coronary artery disease.
In this issue of the Journal, Soeki et al report on the possibility of plasma miRNA-100 levels as a biomarker for coronary plaque vulnerability.9 Meanwhile, it has been reported that disruption or erosion of vulnerable plaque and the subsequent thrombosis are the most frequent causes of ACS. Furthermore, postmortem studies have identified several histologic characteristics of vulnerable plaques, such as greater plaque burden and greater lipid area.10,11 Intravascular ultrasound enables cross-sectional imaging of coronary arteries and provides a more comprehensive assessment of atherosclerotic plaque in vivo. Recently developed integrated backscatter intravascular ultrasound (IB-IVUS), which allows analysis of the tissue components of coronary plaque in vivo, has shown that vulnerable plaque causing ACS is related to an increase in plaque burden, including greater lipid pool12 There are other studies using IB-IVUS that also show an association between the clinical condition of a patient and plaque vulnerability.13,14 Few studies, however, have examined the relevance of biomarkers to coronary plaque, especially its tissue components.
In the study reported here in the Journal, mean plasma levels of miRNA-100 were higher in the coronary sinus than in the aorta in 32 patients with CAD, and the plasma miRNA-100 levels in the aorta positively correlated with the percentage lipid volume (%LV) and negatively correlated with the percentage fibrous volume (%FV) in coronary plaque as measured by IB-IVUS. In addition, transcoronary concentration gradients of circulating miRNA-100 were more strongly correlated with %LV and %FV than the plasma miRNA-100 levels in the aorta. Soeki et al suggest that miRNA-100 is released into the coronary circulation from lipid-rich plaques, thereby reflecting a compensatory reaction to stabilize the plaques by suppressing the mammalian target of rapamycin signaling pathway. These findings suggest that miRNA-100 could be useful as a new-generation biomarker of developing ACS.
There have been critical problems to resolve in applying plasma miRNAs levels in the clinical setting.15 The problem of how to normalize plasma miRNAs levels is important. Because the expression profile of circulating RNA may change according to the condition of the patient, a “housekeeping” miRNAs has not yet been established. Further studies in a large cohort of patients are needed to clarify whether circulating miRNAs could be useful as biomarkers in various clinical settings.