Critical Care
Sudden Death Phenomenon While Bathing in Japan ― Mortality Data ―
2017 年 81 巻 8 号 p. 1144-1149


詳細
2017 年 81 巻 8 号 p. 1144-1149
Background: Bath-related sudden cardiac arrest frequently occurs in Japan, but the mortality data have not been sufficiently reported.
Methods and Results: This prospective cross-sectional observational study was conducted in the Tokyo Metropolis, Saga Prefecture and Yamagata Prefecture between October 2012 and March 2013 (i.e., in winter). We investigated the data for all occurrences in these areas for which the emergency medical system needed to be activated because of an accident or acute illness related to bathing. Emergency personnel enrolled the event when activation of the emergency medical system was related to bathing. Of the 4,599 registered bath-related events, 1,527 (33%) were identified as bath-related cardiac arrest events. Crude mortality (no. deaths per 100,000) during the observational period was 10.0 in Tokyo, 11.6 in Yamagata and 8.5 in Saga. According to the mortality data for age and sex, the estimated number of bath-related deaths nationwide was 13,369 in winter, for the 6 months from October (95% CI: 10,862–16,887). Most cardiac arrest events occurred in tubs filled with water with the face submerged in the water. This suggests that drowning plays a crucial role in the etiology of such phenomena.
Conclusions: The estimated nationwide number of deaths was 13,369 (95% CI: 10,862–16,887) in winter, for the 6 months from October. Crude mortality during the winter season was 10.0 in Tokyo, 11.6 in Yamagata and 8.5 in Saga.
In an aging society, the burden of life-threatening conditions increases. Sudden death during bathing frequently occurs in Japan.1–12 Such bath-related deaths comprise >10% of all sudden deaths,8 and most victims are ≥65 years.1–7,9–12 This phenomenon is unique to Japan and is not seen in other developed countries, such as the USA, UK, Germany or France.9 According to Japanese Government Vital Statistics, in 2011 there were 7,536 unexpected deaths due to drowning (International Classification of Diseases [ICD]-10, W65–74).13 Of those, 5,033 deaths occurred in the bathtub (ICD-10, W65). Furthermore, approximately 90% of those who die in the tub are elderly. The actual number of deaths likely exceeds the official number because many deaths are judged as deaths from disease, such as ischemic heart disease, on the death certificate.10 Therefore, the actual status of this phenomenon has not yet been sufficiently clarified.
Editorial p 1096
To recognize and prevent such fatal events, the true situation and characteristics need to be understood. It was therefore necessary to collect complete data on bath-related deaths in a community-based manner. Few previous studies have reported the actual death toll.6,11 Previous broad surveillance performed in the Tokyo Metropolitan area in winter between October 1999 and March 2000 has estimated the annual nationwide number of sudden deaths during bathing at 14,000.6 Although this surveillance was relatively large scale and well-coordinated with the Tokyo Fire Department, there was no information from other areas. Another study reported that 17,000 events occurred in 2011, but that study had no information from the Tokyo area.11 Other medicolegal and hospital-based studies discussed mortality based on small sample sizes and limited information.1,4,5,7–10,12 Thus, no previous studies have reflected the national status. Furthermore, the sudden death phenomenon is rapidly increasing given that the elderly population (≥65 years) is now growing. A comprehensive investigation of the latest status on a multi-area basis in Japan could provide essential information on this subject.
In this study, we prospectively collected all victim information regarding disease or injury related to bathing, including cardiac arrest, from fire departments in 3 areas (Tokyo Metropolis, Saga Prefecture and Yamagata Prefecture). This study focused on demographic findings to elucidate and estimate the actual mortality of bath-related events.
This prospective cross-sectional observational study was approved by the Ethics Committee of Keio University. It was conducted in winter, between October 2012 and March 2013 in 3 areas, including Tokyo Metropolis, Saga Prefecture (Kyushu region) and Yamagata Prefecture (along the Sea of Japan in Tohoku region). We investigated data from all occurrences in these areas for which the emergency medical system needed to be activated because of an accident or acute illness related to bathing. Emergency personnel completed the surveillance card to enroll the event in this study (Table S1) when they recognized that the emergency medical system activation was related to bathing. The bath-related events were classified into 4 categories: (1) cardiac arrest; (2) survivor in need of help because of any difficulties; (3) any acute illness; (4) injuries.
For all the enrolled data, the events of cardiac arrest were extracted, and the number of victims with cardiac arrest was obtained. Using Japanese Governmental Vital Statistics,14 bath-related mortality by age and sex was calculated in the 3 areas. Crude mortality rate in this study was defined as the total number of bath-related deaths per 100,000 people in winter for the 6 months from October. We calculated 95% CI of the mortality rates using a β-distribution. To compare mortality between the 3 regions, a binomial distribution model was used for statistical testing, and the standardized mortality ratio (SMR) in Yamagata and Saga was calculated by applying mortality data from Tokyo.
To estimate the nationwide number of bath-related deaths between October 2012 and December 2013, we calculated the weighted average of mortality using data from the 3 areas. The number of cardiac arrest events was then estimated for the Japanese population.
During the study period, 4,599 bath-related events were enrolled in this study from the 3 areas. Of those, 1,527 (33%) were identified as bath-related cardiac arrest events (Table 1).
| Situation at the scene | 2012 | 2013 | Total (%) | ||||
|---|---|---|---|---|---|---|---|
| Oct | Nov | Dec | Jan | Feb | Mar | ||
| Tokyo Metropolis | |||||||
| Total | 391 | 587 | 877 | 827 | 631 | 419 | 3,732 (100) |
| Cardiac arrest | 106 | 180 | 319 | 314 | 241 | 165 | 1,325 (36) |
| Survivor in need of help | 56 | 123 | 195 | 192 | 124 | 97 | 787 (21) |
| Acute illness | 138 | 202 | 269 | 243 | 184 | 117 | 1,153 (31) |
| Injury | 88 | 82 | 94 | 78 | 82 | 40 | 464 (12) |
| Unknown | 3 | 0 | 0 | 0 | 0 | 0 | 3 (0) |
| Yamagata Prefecture | |||||||
| Total | 73 | 91 | 95 | 98 | 85 | 64 | 506 (100) |
| Cardiac arrest | 18 | 22 | 24 | 26 | 21 | 21 | 132 (26) |
| Survivor in need of help | 11 | 20 | 14 | 18 | 20 | 13 | 96 (19) |
| Acute illness | 35 | 40 | 47 | 47 | 35 | 22 | 226 (45) |
| Injury | 9 | 9 | 10 | 7 | 9 | 8 | 52 (10) |
| Unknown | 0 | 0 | 0 | 0 | 0 | 0 | 0 (0) |
| Saga Prefecture | |||||||
| Total | 33 | 54 | 80 | 72 | 69 | 53 | 361 (100) |
| Cardiac arrest | 7 | 13 | 20 | 10 | 13 | 7 | 70 (19) |
| Survivor in need of help | 6 | 2 | 11 | 17 | 9 | 7 | 52 (14) |
| Acute illness | 11 | 28 | 37 | 36 | 30 | 32 | 174 (48) |
| Injuries | 8 | 10 | 12 | 8 | 17 | 6 | 61 (17) |
| Unknown | 1 | 1 | 0 | 1 | 0 | 0 | 3 (1) |
| Sum of the 3 areas | |||||||
| Total | 497 | 732 | 1,052 | 997 | 785 | 536 | 4,599 (100) |
| Cardiac arrest | 131 | 215 | 363 | 350 | 275 | 193 | 1,527 (33) |
| Survivor in need of help | 73 | 145 | 220 | 227 | 153 | 117 | 935 (20) |
| Acute illness | 184 | 270 | 353 | 326 | 249 | 171 | 1,553 (34) |
| Injury | 105 | 101 | 116 | 93 | 108 | 54 | 577 (13) |
| Unknown | 4 | 1 | 0 | 1 | 0 | 0 | 6 (0) |
The bath-related crude mortality rates during the winter season from October 2012 to March 2013 in the Tokyo, Yamagata and Saga areas were 10.0 (95% CI: 9.4–10.5), 11.6 (95% CI: 9.7–13.7) and 8.5 (95% CI: 6.0–10.7) deaths per 100,000 people, respectively (Table 2). The crude mortality in Yamagata and Saga was similar to that in Tokyo (P=0.11, P=0.20, respectively). The mortality tended to increase with age in both sexes, and that for male subjects tended to be higher than in female subjects (Figure 1).
| Age (years) | Mortality per 100,000 persons (95% CI) | |||
|---|---|---|---|---|
| Tokyo Metropolis | Yamagata Prefecture | Saga Prefecture | Weighted average | |
| 0–4 | 0.2 (0.0–1.1) | 0.0 (0.0–8.6) | 2.6 (0.1–14.7) | 0.3 (0.0–1.2) |
| 5–9 | 0.0 (0.0–0.8) | 0.0 (0.0–7.8) | 0.0 (0.0–9.5) | 0.0 (0.0–0.6) |
| 10–14 | 0.0 (0.0–0.7) | 0.0 (0.0–7.1) | 0.0 (0.0–8.6) | 0.0 (0.0–0.6) |
| 15–19 | 0.2 (0.0–1.0) | 0.0 (0.0–6.7) | 4.5 (0.6–16.4) | 0.5 (0.1–1.4) |
| 20–24 | 0.3 (0.0–1.0) | 0.0 (0.0–8.6) | 0.0 (0.0–10.0) | 0.2 (0.0–0.9) |
| 25–29 | 0.4 (0.1–1.1) | 0.0 (0.0–7.1) | 0.0 (0.0–9.0) | 0.4 (0.1–1.0) |
| 30–34 | 0.7 (0.3–1.4) | 0.0 (0.0–6.0) | 0.0 (0.0–7.8) | 0.6 (0.3–1.3) |
| 35–39 | 0.7 (0.3–1.4) | 0.0 (0.0–5.3) | 0.0 (0.0–7.1) | 0.7 (0.3–1.3) |
| 40–44 | 0.6 (0.2–1.2) | 0.0 (0.0–5.3) | 0.0 (0.0–7.1) | 0.5 (0.2–1.1) |
| 45–49 | 1.2 (0.6–2.1) | 3.0 (0.4–10.9) | 0.0 (0.0–7.5) | 1.2 (0.7–2.1) |
| 50–54 | 1.5 (0.7–2.5) | 1.4 (0.0–7.6) | 0.0 (0.0–7.1) | 1.4 (0.7–2.3) |
| 55–59 | 2.8 (1.7–4.3) | 3.7 (0.8–10.8) | 3.4 (0.4–12.5) | 2.9 (1.9–4.3) |
| 60–64 | 6.6 (4.9–8.5) | 7.2 (2.9–14.9) | 1.4 (0.0–8.1) | 6.3 (4.8–8.0) |
| 65–69 | 10.5 (8.3–13.0) | 6.7 (2.2–15.6) | 11.3 (4.2–24.6) | 10.2 (8.3–12.5) |
| 70–74 | 21.7 (18.5–25.4) | 14.7 (7.1–27.0) | 25.5 (13.2–44.6) | 21.4 (18.3–24.7) |
| 75–79 | 40.4 (35.4–45.8) | 33.8 (21.4–50.7) | 27.9 (14.4–48.7) | 39.0 (34.5–43.9) |
| 80–84 | 71.1 (63.3–79.6) | 73.3 (53.3–98.4) | 40.5 (22.7–66.9) | 69.2 (62.3–76.7) |
| ≥85 | 100.8 (90.9–111.5) | 60.0 (42.0–83.1) | 51.3 (31.3–79.2) | 91.6 (83.2–100.6) |
| Crude mortality | 10.0 (9.4–10.5) | 11.6 (9.7–13.7) | 8.5 (6.6–10.7) | 9.8 (9.3–10.3) |

Bath-related mortality rate by age and sex in elderly people. Mortality increases with age in both sexes, but is higher in the male than in the female subjects (P<0.05). (●) Tokyo Metropolis; (◆) Yamagata prefecture; (×) Saga prefecture; (○) average. Error bars, 95% confidence interval.
The SMR in Yamagata and Saga was also obtained using mortality by age and sex for Tokyo (Table 3). The mortality in Saga was smaller than in Tokyo, whereas that in Yamagata was similar to that in Tokyo.
| Tokyo Metropolis | Yamagata Prefecture | Saga Prefecture | |||
|---|---|---|---|---|---|
| % (95% CI) | % (95% CI) | P value‡ | % (95% CI) | P value‡ | |
| Total | 100 (95–100) | 80 (68–93) | 0.06 | 70 (55–80) | 0.01 |
| Male | 100 (93–108) | 78 (62–97) | 0.18 | 75 (59–94) | 0.20 |
| Female | 100 (92–108) | 81 (65–99) | 0.25 | 60 (47–73) | 0.02 |
†Obtained using observed mortality in Tokyo as data of the standard population. ‡No. estimated deaths using SMR vs. actual deaths. SMR, standardized mortality ratio.
We calculated the weighted average of mortality using data from the 3 areas (Table 2). The nationwide number of cardiac arrest events was then estimated from the Japanese population. The estimated number of deaths was 13,369 (95% CI: 10,862–16,887) between October 2012 and March 2013 (Figure 2).
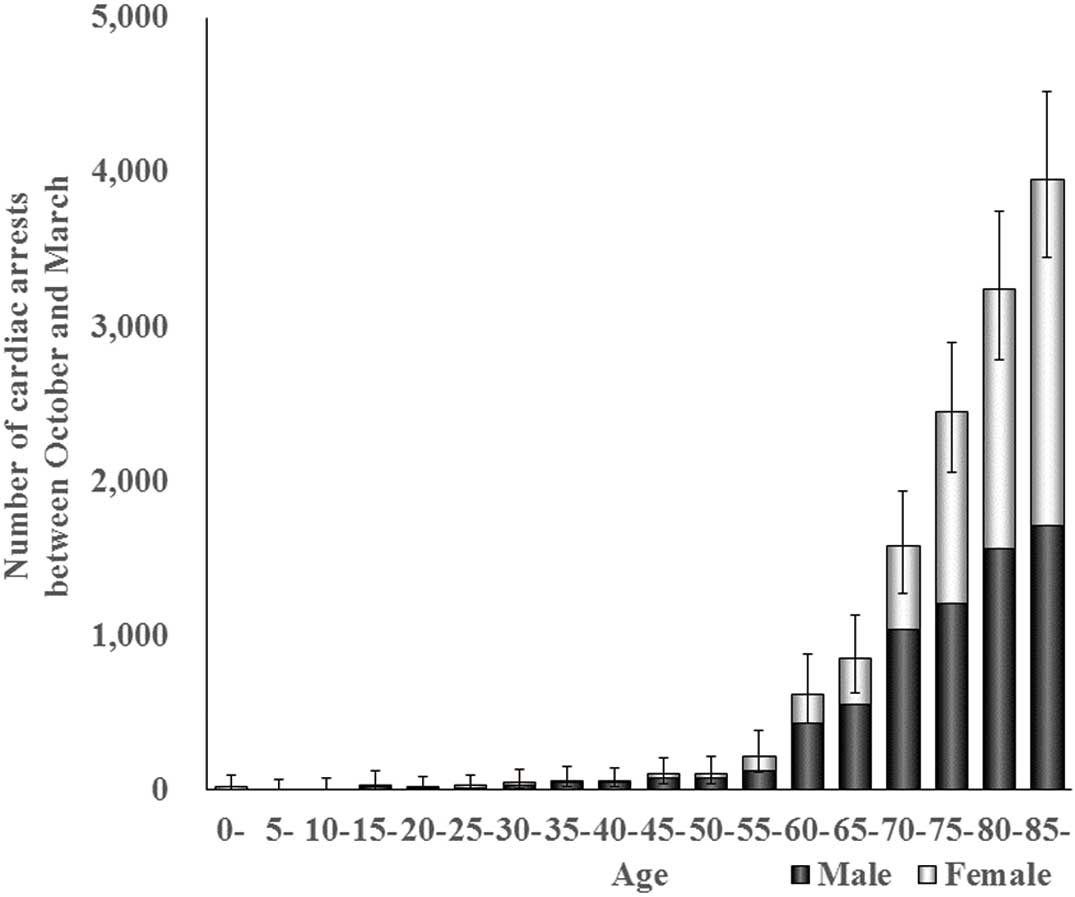
Estimated national number of bathing-related cardiac arrests according to age and sex. In winter, between October 2012 and March 2013, a total of 13,369 deaths (95% CI: 10,862–16,887) deaths was estimated. Error bars, 95% CI.
Most of the cardiac arrest events relating to bathing occurred while the victims bathed in a tub filled with hot water in a private bathroom. More than 90% of the cardiac arrests occurred in the home. Emergency personnel also recognized that >90% of the cardiac arrest events occurred in the bathtub. Furthermore, emergency personnel confirmed that the face was submerged in water at the scene in >80% of cases. Alcohol ingestion beforehand was infrequent (Table 4).
| Tokyo Metropolis, n (%) |
Yamagata Prefecture, n (%) |
Saga Prefecture, n (%) |
Total, n (%) |
|
|---|---|---|---|---|
| Cardiac arrest | 1,325 | 132 | 70 | 1,527 |
| Transported to medical facility (yes/no) |
738/574 (56/44) | 120/12 (91/9) | 68/2 (97/3) | 926/588 (61/39) |
| Setting of the bathroom (home/other) |
1,219/90 (93/7) | 114/18 (86/14) | 65/5 (93/7) | 1,398/113 (93/7) |
| Location of the event (in the tub/other) |
1,207/104 (92/8) | 122/10 (92/8) | 65/5 (93/7) | 1,394/119 (92/8) |
| Submersion of the face in tub water (yes/no) |
948/204 (82/18) | 94/19 (83/17) | 48/10 (83/17) | 1,090/233 (82/18) |
| Preceding alcohol ingestion (yes/no) |
67/433 (13/87) | 13/66 (17/83) | 5/27 (16/84) | 85/526 (14/86) |
In >40% of cardiac arrest events in Tokyo the person was not transported to medical facilities (Table 4). There was no indication for transportation to medical facilities because emergency personnel identified signs of death, such as postmortem rigidity, lividity or decomposition. The number of these cases was high in Tokyo.
This study is the first report based on a prospective survey of all events related to bathing. Of the bath-related events, 33% were identified as cardiac arrest events. Crude mortality during the winter season was approximately 10 per 100,000 people in the 3 areas, whereas regional differences were observed on calculation of SMR. This study is also the first to clarify that most victims submerged their faces in tub water, and many victims were found with clear signs of death.
In this study, crude mortality in each of the 3 areas was similar to that in previous reports. Previous medicolegal studies reported that crude mortality was approximately 10 (deaths/100,000 population).5,10 In previous surveillance, which was performed in the Tokyo Metropolitan area between October 1999 and March 2000, the Tokyo Fire Department identified 578 sudden cardiac arrest events during bathing.6 Using mortality according to age and sex in Tokyo area in this study, we estimated 517 deaths (95% CI: 399–706) between October 1999 and March 2000. The mortality data are reliable. Further, the present mortality rates by age and sex might be similar to the previous situation.
This study observed regional differences by calculating SMR, although previous reports have not established a regional difference in mortality. This may explain why a difference was not elucidated in this study. Previous studies have shown that bathing-related deaths typically occur during winter. Although seasonal differences have not been investigated, the cold environment might influence this phenomenon. Climate, living environment or bathing customs in those areas might contribute to mortality.4 We conducted this study in Tokyo, and in northern and western regions in Japan. The regional fire departments in Tokyo, Yamagata and Saga cooperated in this study.
Considering the regional difference, we calculated the weighted average of mortality using data from the 3 areas. The estimated nationwide number of deaths was 13,369 (95% CI: 10,862–16,887) in winter, between October 2012 and March 2013. The observation was performed for 6 months from October. Accordingly, we changed the number of fatalities into an annual number. We used 1.4-fold the observed number for annual estimation because previous reports have stated that the death toll between April and September is around 0.4-fold higher than the number in the winter season between October and March (Table S2). The annual nationwide number of bath-related death events was estimated at 18,717 (95% CI: 15,207–23,642).
The obtained mortality information in this study might be valuable for other estimations. Using the present estimated nationwide mortality, future and past estimation was performed according to the National Social Security and the National Institute of Population dataset.15 Previously reported estimates of the annual number were 14,000 in 2000 and 17,000 in 2011.6,11 Using obtained mortality in this study, we estimated 11,992 deaths (95% CI: 9,442–15,950) in 2000 and 17,335 (95% CI: 14,006–22,083) in 2010 (Figure 2). Thus, the present estimated annual number seems to be similar to that in previous reports. There may be >20,000 annual deaths in the near future unless an effective prevention is established. Future estimation was performed using mortality and population data by age and sex. The number of future lethal events was estimated at 24,777 (95% CI: 20,506–30,426) in 2025 and 27,337 (95% CI: 22,685–32,897) in 2035 (Figure 3).

Estimated nationwide number of annual bathing-related cardiac arrests. Using mortality data, a total of 11,992 (95% CI: 9,442–15,950) was estimated for 2000 and 17,335 (95% CI: 14,006–22,083) in 2010. Annually, 27,337 individuals (95% CI: 22,802–33,172) are predicted to die in the bathtub in 2035. Error bars, 95% CI.
The characteristics of the events suggest that drowning plays a crucial role in the process of bath-related death, although this study could not elucidate the mechanism. Most of the deaths occurred while the victims bathed in a tub filled with hot water in a private bathroom. Emergency personnel reported that >90% of the events occurred while in the tub. Furthermore, they confirmed that the face was submerged in the tub water at the scene in >80% of cases (Table 4). In recent autopsy studies, water inhalation is observed in the majority of sudden death events.5,9,10,12 Therefore, it was suggested that drowning is strongly associated with the final process of death. In most studies it was suspected that the mechanism of the event was related to cardiovascular events,1,4,5,7,9–12 but these findings suggest that a preceding disturbance of consciousness is an important mechanism rather than sudden cardiac arrest. Early recognition of drowning could be one of the important preventive strategies. To establish a mechanism and strategy for prevention, there is an unavoidable limitation when researchers focus on only lethal events. Further studies that investigate rescued and living subjects are strongly recommended.
Solitary death should warrant special attention. More than 90% of the events in this study occurred in the home. An increasing number of 1-person household elderly persons might cause an increase in solitary deaths because these people may not be rescued during bathing. Tokyo has more 1-person elderly households than the other 2 areas (Table 5). This might be reflected in the number of deaths in this study. In this study, >40% of the subjects in Tokyo were not transported to medical facilities (Table 4). This could be a reason for why the mortality in Tokyo was higher than in other areas.
| Population | |||
|---|---|---|---|
| n×103 | Elderly (≥65 years) | ||
| n×103 (% of population) | One to person households×103 (% of elderly) |
||
| Nationwide | 128,057 | 29,236 (23) | 4,790 (16) |
| Tokyo Metropolis | 13,159 | 2,642 (20) | 622 (24) |
| Yamagata Prefecture | 1,168 | 322 (28) | 30 (9) |
| Saga Prefecture | 849 | 208 (25) | 26 (13) |
This study has several limitations. First, limited areas were analyzed. There is a difference in residential environment and bathing habit in Japan. It is well-known that the residential environment is warmer in the Hokkaido area than in other regions. People in Okinawa have different bathing customs than other areas. Therefore, the nationwide estimation in this study is a potential limitation. Second, the study period was between October and March. Given that these events are uncommon in the summer, our study concentrated on the winter season. This may have led to an inaccurate annual estimation. Although this study has several limitations, this is the first study to report bathing-related mortality by age and sex.
In conclusion, the crude mortality rates during the winter season from October 2012 to March 2013 in the Tokyo, Yamagata and Saga areas were 10.0 (95% CI: 9.4–10.5), 11.6 (95% CI: 9.7–13.7) and 8.5 (95% CI: 6.0–10.7) deaths per 100,000 people, respectively. The estimated nationwide number of deaths was 13,369 (95% CI: 10,862–16,887) for the 6 months from October.
This study was supported by a Health Labour Sciences Research Grant (2012–2013).
The authors declare no conflict of interest.
Supplementary File 1
Table S1. Emergency personnel surveillance card items
Table S2. Seasonal differences in bathing-related deaths
Please find supplementary file(s);
http://dx.doi.org/10.1253/circj.CJ-16-1066