Images in Cardiovascular Medicine
Inferior Vena Cava Thrombi Caused by Enlarged, Solitary Hepatic Cyst
2018 年 82 巻 2 号 p. 604-605

詳細
2018 年 82 巻 2 号 p. 604-605
An 80-year-old woman was referred to hospital due to worsening bilateral pedal edema and mild exertional dyspnea. Physical examination indicated pallor, bilateral pedal edema and a distended abdomen. A non-tender, firm, immobile mass was palpable in the right hypochondrium. Laboratory data indicated hypoalbuminemia (2.5 g/dL; normal, >4.1 g/dL), mildly elevated creatinine (0.95 mg/dL; normal, <0.8 mg/dL), markedly elevated D-dimer (6.3 μg/mL; normal, <1.0 μg/mL), elevated fibrinogen, and fibrin degradation products (FDP; 17.1 μg/mL; normal, <5 μg/mL). Enhanced computed tomography (CT) showed a large hepatic cyst causing compression of the inferior vena cava (IVC). A large IVC thrombus was observed below the level of the compression. No pulmonary embolism was observed (Figure A). Abdominal ultrasonography showed a large hepatic cyst, IVC compression (Figure C), moderate hepatomegaly and a large, free-floating thrombus in the IVC (Figure B). After 1 month of treatment with direct oral anticoagulants (DOAC), follow-up enhanced CT and abdominal ultrasonography with color Doppler showed complete resolution of the thrombus. The patient was in good health with normal vital signs, and physical examination was unremarkable. DOAC were continued to prevent thrombus recurrence. Follow-up ultrasonography showed spontaneous regression of the hepatic cyst with no IVC compression (Figure D). To our surprise, recent follow-up plain abdominal CT (14 months after admission) indicated complete disappearance of the cyst (Figure E).
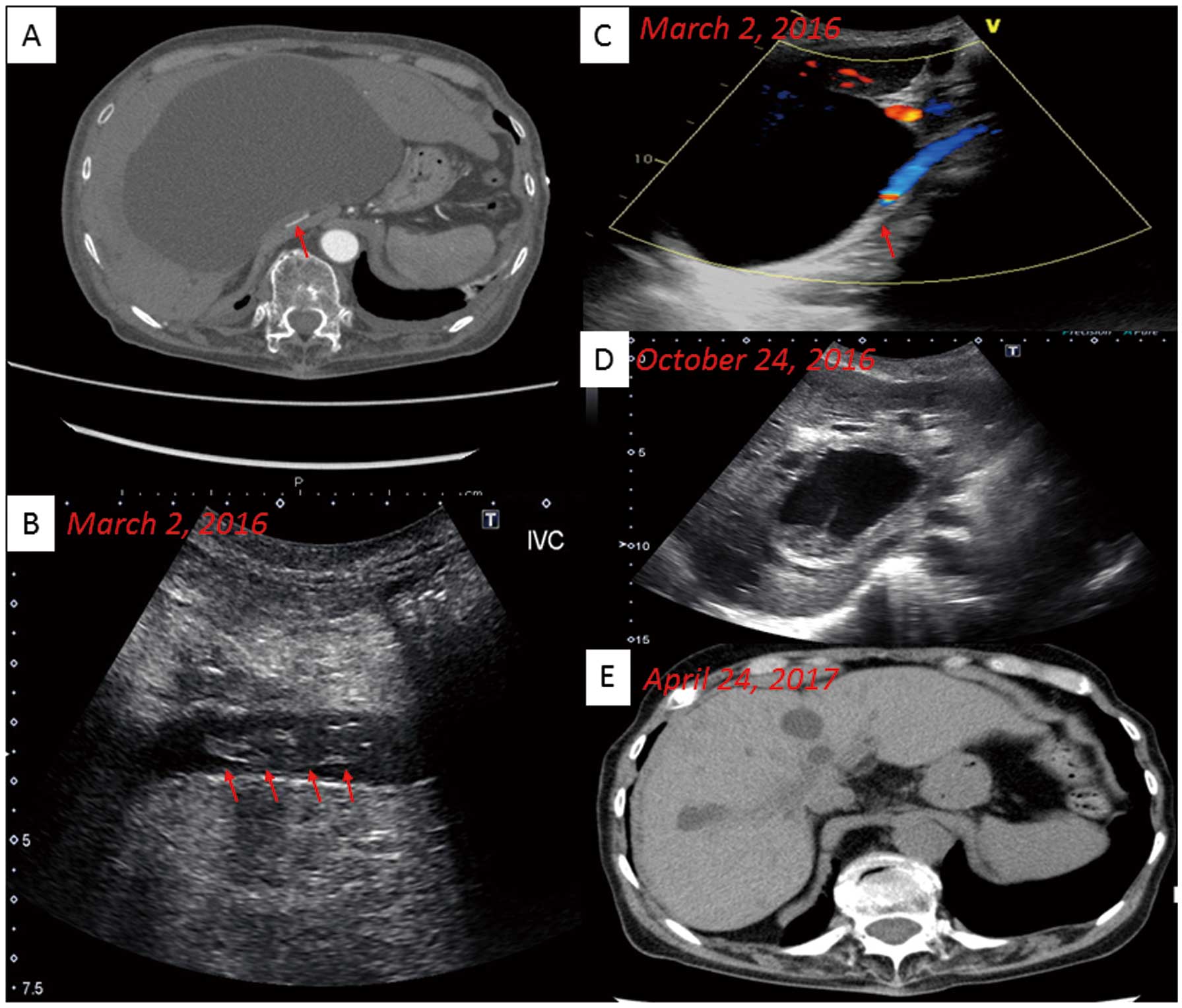
(A) Compression of the inferior vena cava (IVC) by a large liver cyst. Computed tomography (CT) of the abdomen with i.v. contrast showing progressive compression of the IVC (red arrow). (B) Abdominal ultrasonography showing a large, free-floating thrombus in the IVC (red arrows). (C) Abdominal ultrasonography with color Doppler showing a large hepatic cyst and compressed IVC (red arrow). (D) Follow-up ultrasonography in October 2016 showing spontaneous regression of the hepatic cyst including both the capsule and contents. (E) Follow-up CT in April 2017 showing complete disappearance of the large hepatic cyst and no compression of the IVC.
Large IVC thrombi are a rare sequela of IVC syndrome (IVCS). Several conditions can result in IVCS, including autosomal dominant polycystic kidney disease, renal cell carcinoma, post-traumatic hematoma and liver abscess.1–3
Congenital liver cysts detected incidentally on ultrasonography or CT are usually asymptomatic and do not require treatment. Cysts can be single or multiple, with sizes ranging from millimeters to 20 cm.4 Symptomatic cysts are rare but can be due to intracystic bleeding, rupture or secondary bacterial infection. Large hepatic cysts can compress the IVC, resulting in bilateral lower extremity edema and blood flow limitation. Treatment of symptomatic hepatic cysts can include aspiration, injection of a sclerosing agent into the cyst cavity, total cystectomy, hepatic resection or orthotopic transplantation.5,6 Treatment of the IVC thrombus generally includes surgical removal of the blood clot, insertion of an IVC filter and anticoagulation therapy.7,8 IVC thrombi caused by enlarged, solitary hepatic cysts are very rare. In the present case there was no previous imaging (echo or CT) before admission, therefore, we could not evaluate the time course of growth of the hepatic cyst. We speculate, however, that the growth was relatively acute. Conservative anticoagulation therapy with DOAC may be a feasible treatment for IVC thrombi in elderly patients with IVC compression due to large hepatic cysts. If the present patient had been younger, we would have treated her with aspiration and injection of a sclerosing agent into the cyst cavity. Because of the patient’s age, however, conservative therapy with DOAC was chosen for the huge hepatic cyst. Surprisingly, however, the large cyst gradually decreased and had completely disappeared on recent follow-up CT. We were able to identify the time course of the spontaneous regression of the hepatic cyst.
To our knowledge, this is the first report of a large, free-floating IVC thrombus caused by an enlarged, solitary hepatic cyst. Furthermore, both the thrombus and cyst completely vanished during follow-up.
The authors declare no conflict of interest.