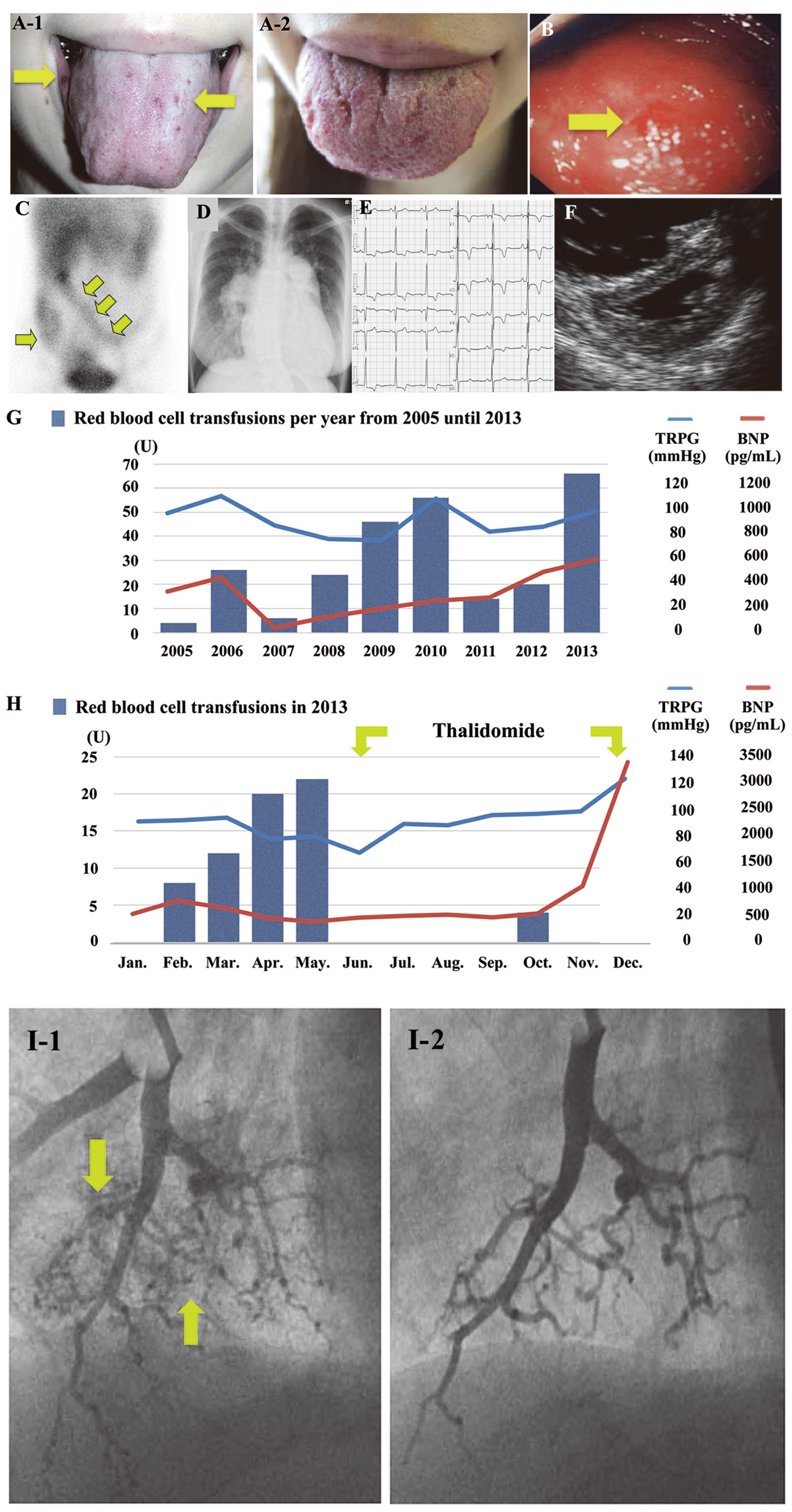
A 37-year-old woman with a known diagnosis of pulmonary arterial hypertension (PAH;
Table; January 1993) associated with hereditary hemorrhagic telangiectasia (HHT) and activin A receptor type II-like 1 (ACVRL1) mutation at the age of 17 years presented for repeated blood transfusions for the progressive anemia derived from recurrent epistaxis, hematemesis, tarry stool and melena. Telangiectasias were noted in the oral cavity (Figure A-1,B, arrows). Gastrointestinal scintigraphy (99mTc-human serum albumin diethylene-triamine-penta-acetic acid) showed extensive hemorrhage throughout the small and large intestines (Figure C, arrows). Chest X-ray showed hilar widening and cardiomegaly (Figure D). Electrocardiography and echocardiography indicated significant right ventricular overload (Figure E,F). Because beraprost 60 µg daily or bosentan 125 mg daily or ambrisentan 10 mg daily worsened the anemia, the patient was treated with 5 mg ambrisentan for PAH thereafter. The requirement for blood transfusion, however, increased year by year (Figure G). In 2013, the patient was urgently hospitalized for progressive anemia due to uncontrollable lower gastrointestinal oozing bleeding documented on video capsule endoscopy. Cardiac catheterization in February 2013 showed severe PAH with mean pulmonary arterial wedge pressure 10 mmHg, pulmonary arterial pressure (PAP), 97/40 mmHg (mean, 60 mmHg); and cardiac index 2.43 L/min/m2
(Table). Her condition deteriorated even after repeated blood transfusions. Therefore, we decided to initiate thalidomide, which increases platelet-derived growth factor-B expression and downregulates vascular endothelial growth factor in endothelial cells, stimulating mural cell coverage and leading to normal vascular maturation.1,2
After the initiation of thalidomide (50 mg daily), the anemia was dramatically improved without blood transfusion (Figure H) and telangiectatic lesions in the tongue were no longer notable (Figure A-2). Although intensive therapy with pulmonary vasodilators might induce bleeding, we were able to add tadalafil 10 mg daily and increase ambrisentan to 7.5 mg daily without any bleeding side-effects. Twelve months after thalidomide treatment, right heart failure developed with deteriorating pulmonary hemodynamics (mean PAP, 90 mmHg; cardiac index, 1.88 L/min/m2;
Table, January 2014). Wedged distal pulmonary angiography showed markedly decreased peripheral vessels (Figure I-2) as compared with that before thalidomide therapy (Figure I-1). After the discontinuation of thalidomide, the bleeding recurred and PAH did not improve, as reflected by serial changes in B-type natriuretic peptide and tricuspid regurgitation pressure gradient (Figure G,H). Finally, the patient died due to right heart failure. Thalidomide was beneficial against mucocutaneous bleeding,1–7
but careful consideration is required with regard to its initiation in HHT patients with PAH.
Table.
Hemodynamic Parameters
| |
PAP (mmHg) |
PVR (Wood units) |
CI (L/min/m2) |
| 1993 January |
76/36 (mean=52) |
7.2 |
3.6 |
| 2013 February |
97/40 (mean=60) |
13.4 |
2.43 |
| 2014 January |
139/70 (mean=90) |
27.7 |
1.88 |
CI, cardiac index; PAP, pulmonary arterial pressure; PVR, pulmonary vascular resistance.
Disclosures
The authors declare no conflicts of interest.
References
- 1.
Lebrin F, Srun S, Raymond K, Martin S, van den Brink S, Freitas C, et al. Thalidomide stimulates vessel maturation and reduces epistaxis in individuals with hereditary hemorrhagic telangiectasia. Nat Med 2010; 16: 420–428.
- 2.
Lacout A, Marcy PY, Hajjam M, Lacombe P. Pulmonary arteriovenous malformations etiologies in HHT patients and potential utility of thalidomide. Med Hypotheses 2013; 80: 587–588.
- 3.
Kersemaekers MAH, Westermann CJJ, Mager JJ, De Weerdt O, Disch FJM, Snijder RJ. Thalidomide for the treatment of epistaxis in hereditary hemorrhagic telangiectasia. Hematol Meet Rep 2007; 1: 22–23.
- 4.
Gossage JR, Chamberlain SM, Sridhar S, Kumar A. An interim report of thalidomide for treatment of recurrent angioectasia related gastrointestinal bleeding. Hematol Meet Rep 2009; 3: 21.
- 5.
Ha M, Kim YJ, Kwon KA, Hahm KB, Kim MJ, Kim DK, et al. Gastric angiodysplasia in a hereditary hemorrhagic telangiectasia type 2 patient. World J Gastroenterol 2012; 18: 1840–1844.
- 6.
Wang XY, Chen Y, Du Q. Successful treatment of thalidomide for recurrent bleeding due to gastric angiodysplasia in hereditary hemorrhagic telangiectasia. Eur Rev Med Pharmacol Sci 2013; 17: 1114–1116.
- 7.
Invernizzi R, Quaglia F, Klersy C, Pagella F, Ornati F, Chu F, et al. Efficacy and safety of thalidomide for the treatment of severe recurrent epistaxis in hereditary haemorrhagic telangiectasia: Results of a non-randomised, single-centre, phase 2 study. Lancet Haematol 2015; 2: e465–e473.