Abstract
Background: The relationships between preoperative fractional flow reserve (FFR) values of the left anterior descending artery (LAD), FFRLAD, and intraoperative transit time flow measurement (TTFM) variables in coronary artery bypass grafting (CABG) remain unclear.
Methods and Results: We retrospectively collected data for 74 in situ left internal thoracic artery (LITA) grafts and 27 saphenous vein grafts (SVGs) to the LAD that were shown to be patent on postoperative angiography. Spearman correlation coefficients were determined between FFRLAD
and TTFM parameters of the LITA graft, as follows: maximum flow (Qmax), −0.22 (P=0.077); minimum flow (Qmin), −0.40 (P=0.014); mean flow (Qm), −0.35 (P=0.039); pulsatility index (PI), 0.33 (P=0.008); diastolic filling (DF): 0.01 (P=0.83); and systolic reverse flow (SRF), 0.37 (P=0.002). Spearman correlation coefficients between FFRLAD
and TTFM parameters of the SVG to LAD were: Qmax, −0.65 (P=0.004); Qmin, −0.43 (P=0.044); Qm, −0.75 (P=0.001); PI, 0.53 (P=0.033); DF, 0.14 (P=0.48); and SRF, 0.61 (P=0.009).
Conclusions: Both LITA grafts and SVGs to the LAD show negative correlations for FFRLAD
with Qmin
and Qm, but positive correlations for FFRLAD
with PI and SFR. These relationships between FFRLAD
and TTFM variables of CABG grafts to the LAD should be recognized.
Fractional flow reserve (FFR), an index calculated by dividing the distal coronary pressure by the proximal pressure measured under conditions of maximum hyperemia, has been well validated as a determinant of lesion-specific myocardial ischemia from epicardial coronary artery disease.1,2 An FFR threshold ranging from 0.75 to 0.80 is used to distinguish functionally significant coronary artery stenosis.3 The FFR Versus Angiography for Multivessel Evaluation (FAME) study demonstrated the superiority of FFR-guided percutaneous coronary intervention (PCI) to conventional angiography-guided PCI.2 Furthermore, the subsequent FAME-2 trial showed that FFR-guided PCI surpasses medical therapy alone,4 primarily by prudently deferring treatment for lesions that may appear stenotic but do not result in lesion-specific ischemia according to FFR measurements. Therefore, current guidelines recommend the use of FFR to complement coronary angiography.5,6 Under these circumstances, the strategy of coronary artery bypass grafting (CABG) is also shifting to FFR guidance, although its advantage over angiography-guided CABG remains undetermined.3
To validate the roles of FFR in CABG, our investigation aimed to assess the impact of preoperative FFR values of the target left anterior descending artery (LAD), referred to as FFRLAD,
on the intraoperative transit time flow measurement (TTFM) of both in situ left internal thoracic artery (LITA) grafts and aortocoronary saphenous vein grafts (SVGs). The aim of this study was to gain a better understanding of TTFM analysis of CABG graft flow, which is recommended in the European guidelines,7,8 as a less invasive, more highly reproducible, and less time-consuming method.
Methods
This retrospective study, using clinical data from routine medical practice for CABG patients, was approved by the Fujita Health University Ethics Committee (HM19-323, October 15, 2019), including a waiver for the need for informed consent for the retrospective use of patient data. The study was conducted according to the ethical guidelines for clinical studies published by the Ministry of Health9 and in accordance with the Declaration of Helsinki.
Study Patients
This study enrolled 101 patients who received CABG grafts to the LAD (74 in situ LITA grants and 27 SVGs; 12.1% of all patients undergoing CABG between 2014 and 2022). Patients were included if they fulfilled the following requirements (Figure 1): preoperative measurements were made of the FFRLAD
to determine the indication for CABG; intraoperative TTFM data were obtained; postoperative patency of the graft was confirmed by multislice computed tomography angiography (MSCTA); and no ischemia in the LAD area was identified on postoperative stress myocardial perfusion scintigraphy.
Our first choice of a graft to the LAD is an in situ LITA, as recommended by many guidelines. However, we used an SVG to the LAD when competitive flow due to less severe stenosis of the LAD may lead to the occurrence of the “string phenomenon” of a LITA graft to the LAD. In addition, we used an SVG to the LAD when the concomitant surgical procedures were complex, such as aortic arch replacement.
Preoperative FFR Measurement
Measurements of FFR were made only in patients with moderate coronary luminal stenosis on coronary angiography to decide the indication for CABG. Intracoronary pressure was measured using a 0.014-inch pressure guide wire (PressureWire Aeris; St Jude Medical, Inc., St Paul, MN, USA). The proximal and distal coronary pressures were recorded by the guiding catheter. The FFR was calculated as the mean distal coronary pressure divided by the mean aortic pressure during maximum hyperemia induced by intravenous continuous infusion of adenosine at a rate of 150–180 mg/kg/min. An FFR ≤0.80 indicates an ischemia-producing stenosis that needs revascularization.10
Intraoperative TTFM
Isolated or concomitant CABG procedures were performed with or without cardiopulmonary bypass. An in situ LITA graft or aortocoronary SVG was used as a bypass graft to the LAD area. Neither Y nor sequential grafting was used for the graft to the LAD.
A flow probe of 3 or 4 mm was placed around the graft for measurement of intraoperative TTFM (Medi-Stim, Oslo, Norway). We routinely obtain the flow profile with TTFM twice: (1) just after graft anastomosis during off-pump CABG or on-pump beating-heart CABG, or just after the aortic declamp during on-pump cardioplegic arrest CABG, to judge the need for graft revision; and (2) when the hemodynamic condition becomes stable before chest closure, with a mean blood pressure of 70–90 mmHg and a heart rate of 80–100 beats/min.
The following TTFM variables were calculated: maximum flow (Qmax; mL/min); minimum flow (Qmin; mL/min); mean flow (Qm; mL/min); pulsatility index (PI), where PI = (Qmax − Qmin) / Qm; diastolic filling (DF), where DF = 100 × ∫diastolic flow (Qd) / (∫systolic flow (Qs) + ∫Qd) systolic reverse flow (SRF), where SRF=volume of backward flow/volume of forward flow; and the fast Fourier transformation (FFT) ratio.11 The FFT ratio is calculated as F0/H1, where F0
is a power of the fundamental frequency and H1
is a power of the first harmonic on the FFT analysis of the blood flow curve.12 FFT analysis is based upon the principal that all periodic waveforms can be broken down into a series of pure sine waves or harmonics. Harmonics exist at frequencies that are multiplies of the fundamental frequency and are described in terms of an amplitude and phase.13,14
Postoperative Evaluation
For postoperative graft evaluation, every patient underwent cardiac imaging with MSCTA approximately 2 months after CABG as a routine checkup, using a β-blocker and isosorbide mononitrate to ensure the adequacy of images. In addition, every patient routinely underwent adenosine stress and rest myocardial perfusion scintigraphy approximately 2 months after CABG, using adenosine infused at a rate of 0.14 mg/kg/min for 6 min and 111–148 MBq of Thallium-201 administered 3 min before the end of the adenosine infusion. Single photon emission computed tomography images were then acquired 5 min later. Rest-redistribution scans were obtained after 4 h. Six segments, including the anteroseptal area perfused by the LITA graft or SVG to the LAD, were analyzed in the left ventricular short-axis image at the papillary muscle level.
Statistical Analysis
Categorical data are presented as either a number or a percentage; continuous data are presented as the mean±SD. Mann-Whitney tests were used to compare 2 continuous variables. Fisher’s exact tests were used to compare 2 categorical variables. A correlation analysis was performed between the intraoperative TTFM parameters and preoperative FFRLAD
using Pearson correlation coefficients, based on the linearity of the relationship between quantitative variables. One-tailed P<0.05 was considered statistically significant. All statistical analyses were performed using SPSS 18 (IBM Corporation, Armonk, NY, USA).
Results
Patient Characteristics
As indicated in the Table, there were no significances in patient characteristics between those receiving LITA grafts and SVGs, except for the following 4 characteristics: diabetes was more prevalent in the LITA-LAD group, peripheral artery disease was more prevalent in the SVG-LAD group, left ventricular end-diastolic dimension was larger in the SVG-LAD group, and isolated CABG was more frequently performed in the LITA-LAD group while concomitant procedures were more frequently performed, especially total arch replacement, in the SVG-LAD group.
Table.
Patient Characteristics
| |
LITA graft to LAD
(n=74) |
SVG to LAD
(n=27) |
P value |
| Age (years) |
68±9 |
71±10 |
0.06 |
| Male sex |
52 (70) |
21 (78) |
0.32 |
| Hypertension |
65 (88) |
23 (85) |
0.47 |
| Hypercholesterolemia |
55 (74) |
15 (56) |
0.06 |
| Diabetes |
46 (62) |
6 (22) |
0.0004 |
| Smoking habit |
38 (51) |
18 (67) |
0.13 |
| Pulmonary disease |
14 (19) |
7 (26) |
0.31 |
| Previous MI |
13 (18) |
3 (11) |
0.33 |
| Chronic kidney disease |
35 (47) |
12 (44) |
0.49 |
| Previous stroke |
10 (14) |
3 (11) |
0.52 |
| Peripheral artery disease |
18 (24) |
12 (44) |
0.045 |
| Left ventricular |
| End-diastolic dimension (mm) |
49.6±7.7 |
53.6±9.6 |
0.029 |
| End-systolic dimension (mm) |
36.1±9.8 |
39.3±12.9 |
0.12 |
| Ejection fraction |
0.52±0.12 |
0.51±0.13 |
0.38 |
| Isolated CABG |
51 (69) |
3 (11) |
0.0001 |
| Off-pump |
12 (16) |
0 |
|
| On-pump |
39 (53) |
3 (11) |
|
| Concomitant CABG with |
23 (31) |
24 (89) |
0.0001 |
| Mitral valve repair |
6 (8.1) |
4 (15) |
|
| AVR |
11 (15) |
8 (30) |
|
| AVR+hemiarch replacement |
3 (4.1) |
|
|
| MVR |
1 (1.4) |
|
|
| AVR+MVR |
1 (1.4) |
2 (7.4) |
|
| Aortic root surgery |
1 (1.4) |
2 (7.4) |
|
| Total arch replacement |
|
7 (26) |
|
| Cardiac tumor resection |
|
1 (3.7) |
|
Unless indicated otherwise, data are given as the mean±SD or n (%). AVR, aortic valve replacement; CABG, coronary artery bypass grafting; LAD, left anterior descending artery; LITA, in situ left internal thoracic artery; MI, myocardial infarction; MVR, mitral valve replacement; SVG, saphenous vein graft.
All patients were free from perioperative myocardial infarction, based on electrocardiographic changes and serum biomarkers. The postoperative course for all patients was uneventful, with a median hospital stay of 14 days. Postoperative MSCTAs demonstrated patent in situ LITA-LAD and SVG-LAD in all study patients. Postoperative myocardial perfusion scintigraphy also demonstrated no ischemia in the LAD area for all study patients.
FFR and TTFM Variables
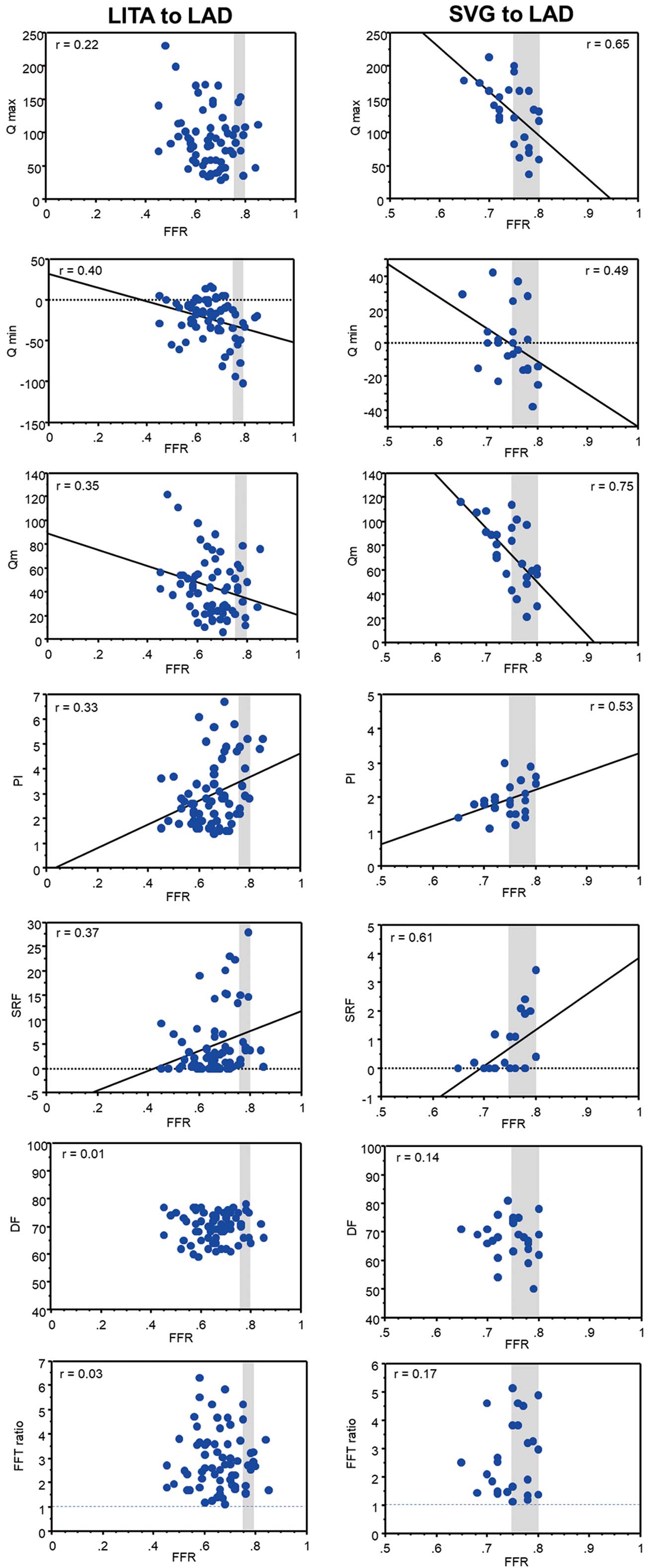
As shown in Figure 2, the FFRLAD
for the LITA graft to the LAD was significantly negatively correlated with Qmin
(r=−0.40; P=0.014) and Qm
(r=−0.35; P=0.039), but significantly positively correlated with PI (r=0.33; P=0.008) and SRF (r=0.37; P=0.002). The FFRLAD
for the LITA graft to the LAD was not correlated with Qmax, DF, or the FFT ratio.
As also shown in Figure 2, the FFRLAD
for the SVG to LAD was significantly negatively correlated with Qmax
(r=−0.65, P=0.004), Qmin
(r=−0.43, P=0.044), and Qm
(r=−0.75, P=0.001), but significantly positively correlated with PI (r=0.53; P=0.033) and SRF (r=0.61; P=0.009). The FFRLAD
for the SVG to LAD was not correlated with DF and the FFT ratio.
In summary, both LITA grafts and SVGs to the LAD showed negative correlations of FFRLAD
with Qmin
and Qm, but positive correlations of FFRLAD
with PI and SFR.
Representative Cases
Figure 3 shows the intraoperative TTFM of the LITA graft to the LAD with an FFRLAD
of 0.72 in a 58-year-old male patient undergoing isolated CABG. All TTFM parameters showed good values and the FFT analysis also showed a gradually attenuating waveform with an FFT ratio of 3.6. Postoperative MSCTA showed the patent LITA, and no ischemia was found at the LAD area on stress myocardial scintigraphy.
Figure 3 also shows the TTFM of the LITA graft to the LAD with a higher FFRLAD
of 0.79, in a 78-year-old male patient undergoing isolated CABG. The Qmin
and Qm
are as low as −28 and 13 mL/min, respectively, whereas the PI and SFR are as high as 4.5 and 15%, respectively. However, the FFT analysis provided a gradually attenuating waveform with an FFT ratio of 3.2. Although the postoperative MSCTA showed a patent LITA graft with a narrow diameter, no ischemia was found in the LAD area on stress myocardial scintigraphy.
Figure 4 shows the intraoperative TTFM of an SVG to the LAD with an FFRLAD
of 0.72 in a 78-year-old male patient undergoing total arch replacement and CABG. All TTFM parameters showed acceptable values and a gradually attenuating waveform on FFT analysis, with an FFT ratio of 1.8. Postoperative MSCTA showed a patent SVG, and no ischemia was found at the LAD area on stress myocardial scintigraphy.
Figure 4 also shows the TTFM of an SVG to the LAD with a gray-zone FFRLAD
of 0.78 in a 79-year-old male patient undergoing aortic valve replacement and CABG. Although reversal flow is larger, because Qmin
was −25 mL/min and SFR was 3.4%, the FFT analysis showed a gradually attenuating waveform with an FFT ratio of 1.1.
Discussion
The main findings of our analysis of the in situ LITA graft and SVG to the LAD are as follows:
1. Most of the TTFM variables of both the LITA graft and SVG are strongly affected by preoperative FFRLAD
values, including Qmin, Qm, PI, and SFR, which have been used as good indicators to evaluate the quality of the CABG anastomosis.
2. For both LITA grafts and SVGs, the FFT ratio is an independent TTFM variable that is not influenced by FFRLAD.
FFR-Guided CABG
Our main findings may be important in the current era, in which FFR-guided CABG is receiving growing attention, despite no evidence to support improved clinical outcomes.15–21 However, we should keep in mind that the relative benefits of CABG compared with PCI may be lost with the consequences of a shift towards FFR-guided CABG, which reduces the number of vessels grafted and increases the rate of anatomically defined incomplete revascularization.
FFR and TTFM Variables
In addition to morphological assessment using color Doppler, Qm
>15 mL/min, PI <5.0, DF >50%, SRF <4%, and an FFT ratio >1.0 are TTFM variables indicative of a patent graft during CABG.11,22 However, these variables vary with hemodynamic factors, as well as anastomotic quality. Honda et al23 reported significantly lower Qm
and higher PI of the LITA graft to the LAD with an FFR ≥0.75 compared with LITA grafts to the LAD with FFR <0.75. We have also reported that most TTFM variables of the LITA graft to the LAD are strongly affected by FFRLAD.24 In the present study, we have revealed similar correlations between FFRLAD
values and Qmin, Qm, PI, and SFR of the SVG to the LAD.
We observed no correlations of FFRLAD
with DF defined by the equation DF = 100 × ∫Qd / (∫Qs + ∫Qd), although DF may be an independent predictor of failed anastomosis.25 By identifying changes in the diastolic-delivered blood volume vs. total delivered blood volume, DF can quantify the gradual shift from diastolic to systolic dominance with increasing occlusion observed in the CABG flow rate waveform.26 However, when systolic reversal graft flow to the LAD with higher FFRLAD
occurs, ∫Qs
is negative, therefore leading to an inaccurate DF value on the TTFM machine. To obtain accurate DF values, the negative ∫Qs
should be substituted with its absolute value, ∫|Qs
|.
Unaffected TTFM Variables
It is noted that the FFT ratio11–14,24 is an independent TTFM index unaffected by FFRLAD. Mao et al14 demonstrated the application of FFT analysis in assessing CABG flow using multiscale models of a 3-dimensional LITA-LAD graft with varying degrees of stenosis in the LAD, resulting in different magnitudes of competitive flows. Their in vitro findings indicated that an FFT ratio >1.0 is maintained for patent LITA-LAD grafts regardless of the degree of stenosis, as shown in the present study. Therefore, FFT analysis of the TTFM flow curve may be recommended for grafts to the LAD with a higher FFRLAD
(>0.75). When the FFT ratio is ≥1.0, even if other TTFM variables are suboptimal, the graft anastomosis can be considered satisfactory, and the surgical indication for revascularization is not adequate. Conversely, an FFT ratio <1.0 suggests a potential issue with the anastomosis, necessitating consideration of graft revision.
Clinical Perspectives
The following perspectives are derived from the close relationships between FFRLAD
and TTFM variables of grafts to the LAD, as shown in the present study:
1. When judging the CABG anastomosis by intraoperative TTFM, as recommended in the guidelines,5 the influence of the preoperative FFR should be taken into account to avoid inadvertent re-anastomosis or revision of the grafts due to a poor TTFM variable.
2. As shown in Figure 2, SVGs show more beneficial TTFM variables, higher Qm, lower PI, and lower SFR, than LITA grafts to the LAD with the gray-zone FFRLAD. Although the long-term patency is limited, SVGs may be better as a conduit to the gray-zone LAD with 0.75<FFRLAD<0.80. As Sabik et al reported, grafting moderately stenosed coronary arteries with an SVG does not affect long-term mortality.27 In addition, we expect long-term patency of the SVG to the LAD with gray-zone FFR with the no-touch harvesting technique, as reported by Samano et al.28
Study Limitations
The present study has several limitations. First, we retrospectively collected the data of a small number of patients from a single center, meaning that the study was susceptible to potential sources of bias. Second, this study included a highly selected portion of CABG patients with patent grafts and the patients undergoing CABG using SVGs with concomitant aortic valve replacement. Although the effect of the turbulence of downstream prosthetic aortic valves on SVGs anastomosed to the ascending aorta has not been adequately studied, Hassanein et al reported that the flow in SVGs in patients with biological valves was higher than in those with the mechanical valve.29 Third, we used MSCTA for postoperative graft assessment, which cannot evaluate “to and fro” flow competition of the LITA graft when compared with coronary angiography. Intraoperative epicardial ultrasound or indocyanine green angiography may be an alternative to check the anastomosis site. Fourth, because graft flow is sensitive to many parameters, including hemodynamics, diabetes and female sex, endothelial dysfunction and altered resistance distal to the coronary lesions, efforts to control for these variables in a regression model rather than a simple linear correlation may help clarify the nature and strength of the relationship. Fifth, most TTFM variables analyzed showed a relatively low intensity of correlation with FFR, although the correlation was statistically significant.
Conclusions
Most TTFM variables of both in situ LITA grafts and SVGs to the LAD during CABG are strongly affected by preoperative FFRLAD
values, including Qmin, Qm, PI, and SFR, which have been used as good indicators to evaluate the quality of the anastomosis. Because the FFT ratio is not influenced by FFR, FFT analysis of the TTFM results may be recommend for both the in situ LITA graft and SVG to the LAD. It is imperative to recognize such relationships between FFRLAD
and TTFM variables of CABG grafts to the LAD.
Sources of Funding
The authors have received no financial support for the research, authorship, and publication of this article.
Disclosures
The authors have no conflicts of interest to disclose.
IRB Information
This study was approved by the Ethics Committee of Fujita Health University (No. HM19-323; date of approval, October 15, 2019).
References
- 1.
Spaan JA, Piek JJ, Hoffman JI, Siebes M. Physiological basis of clinically used coronary hemodynamic indices. Circulation 2006; 113: 446–455.
- 2.
Tonino PA, De Bruyne B, Pijls NH, Siebert U, Ikeno F, van’t Veer M, et al. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N Engl J Med 2009; 360: 213–224.
- 3.
Spadaccio C, Glineur D, Barbato E, Di Franco A, Oldroyd KG, Biondi-Zoccai G, et al. Fractional flow reserve-based coronary artery bypass surgery: Current evidence and future directions. JACC Cardiovasc Interv 2020; 13: 1086–1096.
- 4.
Xaplanteris P, Fournier S, Pijls NHJ, Fearon WF, Barbato E, Tonino PAL, et al; FAME 2 Investigators. Five-year outcomes with PCI guided by fractional flow reserve. N Engl J Med 2018; 379: 250–259.
- 5.
Neumann FJ, Sousa-Uva M, Ahlsson A, Alfonso F, Banning AP, Benedetto U, et al; ESC Scientific Document Group. 2018 ESC/EACTS guidelines on myocardial revascularization. Eur Heart J 2019; 40: 87–165.
- 6.
Lawton JS, Tamis-Holland JE, Bangalore S, Bates ER, Beckie TM, Bischoff JM, et al. 2021 ACC/AHA/SCAI guideline for coronary artery revascularization: Executive summary: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022; 145: e4–e17.
- 7.
Kolh P, Windecker S, Alfonso F, Collet JP, Cremer J, Falk V, et al. 2014 ESC/EACTS guidelines on myocardial revascularization: The Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur J Cardiothorac Surg 2014; 46: 517–592.
- 8.
National Institute for Heath and Care Excellence (NICE). MiraQ for assessing graft flow during coronary artery bypass graft surgery. Medical technologies guidance [MTG8]. 2022. https://www.nice.org.uk/guidance/mtg8 (accessed August 1, 2023).
- 9.
Guidelines for health, labour and welfare scientific research. Available at https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/hokabunya/kenkyujigyou/i-kenkyu/index.html (accessed August 1, 2023).
- 10.
Elgendy IY, Conti CR, Bavry AA. Fractional flow reserve: An updated review. Clin Cardiol 2014; 37: 371–380.
- 11.
Takami Y, Takagi Y. Roles of Transit-time flow measurement for coronary artery bypass surgery. Thorac Cardiovasc Surg 2018; 66: 426–433.
- 12.
Takami Y, Ina H. Relation of intraoperative flow measurement with postoperative quantitative angiographic assessment of coronary artery bypass grafting. Ann Thorac Surg 2001; 72: 1270–1274.
- 13.
Hatada A, Yoshimasu T, Kaneko M, Kawago M, Yuzaki M, Honda K, et al. Relation of waveform of transit-time flow measurement and graft patency in coronary artery bypass grafting. J Thorac Cardiovasc Surg 2007; 134: 789–791.
- 14.
Mao B, Wang W, Zhao Z, Zhao X, Li L, Zhang H, et al. On the relationship between competitive flow and FFT analysis of the flow waves in the left internal mammary artery graft in the process of CABG. Biomed Eng Online 2016; 15(Suppl 2): 129.
- 15.
Botman CJ, Schonberger J, Koolen S, Penn O, Botman H, Dib N, et al. Does stenosis severity of native vessels influence bypass graft patency?: A prospective fractional flow reserve-guided study. Ann Thorac Surg 2007; 83: 2093–2097.
- 16.
Toth G, De Bruyne B, Casselman F, De Vroey F, Pyxaras S, Di Serafino L, et al. Fractional flow reserve-guided versus angiography-guided coronary artery bypass graft surgery. Circulation 2013; 128: 1405–1411.
- 17.
Thuesen AL, Riber LP, Veien KT, Christiansen EH, Jensen SE, Modrau I, et al. Fractional flow reserve versus angiographically-guided coronary artery bypass grafting. J Am Coll Cardiol 2018; 72: 2732–2743.
- 18.
Toth GG, De Bruyne B, Kala P, Ribichini FL, Casselman F, Ramos R, et al. Graft patency after FFR-guided versus angiography-guided coronary artery bypass grafting: The GRAFFITI trial. EuroIntervention 2019; 15: e999–e1005.
- 19.
Glineur D, Grau JB, Etienne PY, Benedetto U, Fortier JH, Papadatos S, et al. Impact of preoperative fractional flow reserve on arterial bypass graft anastomotic function: The IMPAG trial. Eur Heart J 2019; 40: 2421–2428.
- 20.
Fournier S, Toth GG, De Bruyne B, Johnson NP, Ciccarelli G, Xaplanteris P, et al. Six-year follow-up of fractional flow reserve-guided versus angiography-guided coronary artery bypass graft surgery. Circ Cardiovasc Interv 2018; 11: e006368.
- 21.
Spadaccio C, Glineur D, Barbato E, Di Franco A, Oldroyd KG, Biondi-Zoccai G, et al. Fractional flow reserve-based coronary artery bypass surgery: Current evidence and future directions. JACC Cardiovasc Interv 2020; 13: 1086–1096.
- 22.
Gaudino M, Antoniades C, Benedetto U, Deb S, Di Franco A, Di Giammarco G, et al. Mechanisms, consequences, and prevention of coronary graft failure. Circulation 2017; 136: 1749–1764.
- 23.
Honda K, Okamura Y, Nishimura Y, Uchita S, Yuzaki M, Kaneko M, et al. Graft flow assessment using a transit time flow meter in fractional flow reserve-guided coronary artery bypass surgery. J Thorac Cardiovasc Surg 2015; 149: 1622–1628.
- 24.
Noda M, Takami Y, Amano K, Sakurai Y, Akita K, Maekawa A, et al. Relation of fractional flow reserve with transit time coronary artery bypass graft flow measurement. Ann Thorac Surg 2021; 111: 134–140.
- 25.
Niclauss L. Techniques and standards in intraoperative graft verification by transit time flow measurement after coronary artery bypass graft surgery: A critical review. Eur J Cardiothorac Surg 2017; 51: 26–33.
- 26.
Takahashi K, Morota T, Ishii Y. A novel transit-time flow metric, diastolic resistance index, detects subcritical anastomotic stenosis in coronary artery bypass grafting. JTCVS Tech 2022; 17: 94–103.
- 27.
Sabik JF, Olivares G, Raza S, Lytle BW, Houghtaling PL, Blackstone EH. Does grafting coronary arteries with only moderate stenosis affect long-term mortality? J Thorac Cardiovasc Surg 2016; 151: 806–811.e3.
- 28.
Samano N, Geijer H, Liden M, Fremes S, Bodin L, Souza D. The no-touch saphenous vein for coronary artery bypass grafting maintains a patency, after 16 years, comparable to the left internal thoracic artery: A randomized trial. J Thorac Cardiovasc Surg 2015; 150: 880–888.
- 29.
Hassanein W, Albert A, Florath I, Hegazy YY, Rosendahl U, Bauer S, et al. Concomitant aortic valve replacement and coronary bypass: The effect of valve type on the blood flow in bypass grafts. Eur J Cardiothorac Surg 2007; 31: 391–396.