Abstract
Background:
The validity of the Academic Research Consortium for High Bleeding Risk (ARC-HBR) definitions of early (<1 year), late (1–4 years), and very late (>4 years) bleeding events is unknown.
Methods and Results:
This study was performed on patients (n=3,453) implanted with second-generation drug-eluting stents (DES) between 2010 and 2013. Data on all criteria of the ARC-HBR definition were collected retrospectively. The primary endpoint was Bleeding Academic Research Consortium Type 3 or 5 bleeding events; the ischemic endpoint was a composite of cardiac death, myocardial infarction, and ischemic stroke. The mean follow-up period was 7.5 years. Compared with non-high bleeding risk (HBR) patients, HBR patients (n=1,840; 53.3%) had an increased risk of the primary endpoint (early events, 3.6% vs. 0.5% [P<0.0001]; late events, 5.3% vs. 2.5% [P<0.0001]; very late events, 5.5% vs. 2.1% [P<0.0001]) and of ischemic events during follow-up. The discrimination ability of the ARC-HBR definition for late and very late bleeding events was comparable to that of early bleeding events (C statistics 0.679, 0.621, and 0.620, respectively) with high negative predictive value (96.6%, 95.1%, and 93.1%, respectively). Multivariate analysis revealed the different effects of individual criteria on bleeding events in each follow-up period.
Conclusions:
The ARC-HBR definition consistently identified patients at risk of long-term bleeding and ischemic events after second-generation DES implantation.
Current advances in technologies related to percutaneous coronary intervention (PCI) have improved clinical outcomes and enabled a subset of patients with complex clinical conditions to be treated.1–3
In such cases, the benefit of coronary revascularization may be counterbalanced by adverse bleeding events arising from long-term antithrombotic therapy. Although prolonged dual antiplatelet therapy (DAPT) reduces the risk of thrombotic events, it is associated with a higher risk of bleeding events.4–6
The current guidelines call for the identification of patients with a high bleeding risk (HBR) to minimize bleeding complications and ensure appropriate antiplatelet therapy, which is a cornerstone of management after PCI.7–9
Several bleeding risk scores have been proposed and are recommended to assess individual bleeding risks.10–12
However, the discrimination ability of these risk scores is modest. Recently, the Academic Research Consortium (ARC) for HBR provided a consensus document with a new definition consisting of 17 major and minor criteria to standardize HBR.13
Although several studies have confirmed the clinical validity of the ARC-HBR definition in predicting bleeding events, most of these studies set the bleeding endpoint at 1 year;14–18
however, the long-term bleeding risk after PCI remains an important concern, especially in patients with complex clinical conditions. To validate the ARC-HBR definitions, we aimed to investigate long-term clinical events, including bleeding and ischemic events, in patients with a HBR after implantation of a second-generation drug-eluting stent (DES).
Editorial p ????
Methods
Study Population
This study was a retrospective single-center study involving 4,700 patients who underwent PCI using DES in Kurashiki Central Hospital between January 2010 and December 2013. Of these 4,700 patients, 3,580 underwent PCI for the first time during the study period. Excluding 127 patients who underwent PCI with a bare metal stent (n=17) or a first-generation DES (n=110) left 3,453 patients who had been exclusively treated with a second-generation DES (Endeavor [Medtronic Vascular, Santa Rosa, CA, USA], XIECE V [Abbott Vascular, Santa Clara, CA, USA], NOBORI [Terumo, Tokyo, Japan], PROMUS [Boston Scientific, Natick, MA, USA], or Resolute Integrity [Medtronic Vascular]) in the study.
All study procedures were performed in accordance with the Declaration of Helsinki, and informed consent was obtained from all patients for both the PCI procedure and subsequent data collection and analysis for research purposes. The study was approved by the appropriate institutional ethics committee.
Study Definitions and Outcomes
The primary bleeding endpoint was defined as Bleeding Academic Research Consortium (BARC) Type 3 or 5 bleeding events.19
The primary ischemic endpoint was defined as a composite of cardiac death, myocardial infarction (MI), and ischemic stroke. The endpoints in this study were all-cause mortality, cardiac mortality, MI, definite or probable stent thrombosis (ST), target lesion revascularization, and ischemic stroke. ST and MI were defined according to the relevant ARC definitions.20
Follow-up and Data Collection
Baseline data were collected from patients’ medical records. Clinical follow-up information was obtained at the time of office visits, by telephone survey, or by writing a letter of inquiry to the primary care physician or patient. Information regarding major and minor criteria of the ARC-HBR definition was collected retrospectively from patients’ medical records and inquiries to primary care physicians. The study population was divided into 2 groups according to the ARC-HBR definition: HBR and non-HBR groups.
Antiplatelet Therapy
All patients were pretreated with aspirin (100 mg daily) and ticlopidine (200 mg daily)/clopidogrel (75 mg daily). According to the available guidelines during the study period, DAPT was recommended for at least 8 months after the index procedure; however, the duration of antiplatelet therapy was left to the discretion of individual physicians. The status of antiplatelet therapy was evaluated throughout the follow-up period, and persistent discontinuation of DAPT was defined as the withdrawal of aspirin or thienopyridine for at least 2 office visits or telephone inquiries.
Statistical Analysis
Categorical variables were compared using Chi-squared tests. Continuous variables are expressed as the mean±SD and were compared using Student’s t-test or the Wilcoxon rank-sum test based on data distribution. Cumulative incidence was estimated using the Kaplan-Meier method, and the significance of differences was assessed using the log-rank test. All clinical events were accounted for the first occurring event.
To evaluate the effect of HBR on the primary endpoint at the early (<1 year), late (1–4 years), and very late (>4 years) time points, we used a landmark analysis at 1 and 4 years. The ARC-HBR scores were calculated by allocating 1 point for each major criterion and 0.5 points for each minor criterion. The discrimination ability of the scores was assessed using C statistics. A Cox proportional hazards model was used to estimate the effects of an HBR definition, as well as individual criteria, relative to non-HBR patients, as well as those without the individual criteria, for clinical events, expressed as hazard ratios (HRs) and 95% confidence intervals (CIs). Covariates included in the multivariate model were the ARC-HBR criteria that had a frequency >1% and reached statistical significance (P<0.1). Patients with ARC-HBR major criteria were divided into 2 groups based on the number of major criteria, regardless of the number of overlapping minor criteria: those with ≥2 major criteria and those with 1 major criterion. Patients with ≥2 minor criteria without a major criterion were allocated to a separate group.
In all cases, 2-tailed P<0.05 was considered significant. Statistical analyses were conducted using R (R Foundation for Statistical Computing, Vienna, Austria).
Results
Baseline Characteristics
Of the 3,453 patients included in the final analysis, 1,840 (53.3%) were considered to be at HBR based on the ARC-HBR definition (Figure 1). The baseline characteristics of all patients, and HBR and non-HBR patients separately, are presented in
Table 1. HBR patients were much older, more likely to be female, and had significantly higher rates of diabetes and peripheral artery disease than non-HBR patients. The duration of DAPT was not significantly different between the 2 groups (Supplementary Figure). The mean follow-up period was 2,755±595 days.

Table 1.
Baseline Characteristics
| |
Overall |
HBR |
Non-HBR |
P value |
| No. patients |
3,453 |
1,840 |
1,613 |
|
| Male sex |
2,573 (74.6) |
1,246 (67.7) |
1,327 (82.4) |
<0.001 |
| Age (years) |
70.1±11.1 |
74.9±9.9 |
64.7±9.7 |
<0.001 |
| BMI (kg/m2) |
24.1±3.6 |
23.4±3.6 |
24.9±3.5 |
<0.001 |
| Hypertension |
2,484 (71.9) |
1,404 (76.3) |
1,080 (67.0) |
<0.001 |
| Diabetes |
1,371 (39.7) |
782 (42.5) |
589 (36.5) |
<0.001 |
| Insulin therapy |
340 (9.8) |
229 (12.4) |
111 (6.9) |
<0.001 |
| Dyslipidemia |
2,095 (60.7) |
1,029 (55.9) |
1,066 (66.1) |
<0.001 |
| Current smoker |
525 (15.2) |
168 (9.1) |
357 (22.1) |
<0.001 |
| Multivessel disease |
1,678 (48.6) |
931 (50.6) |
747 (46.3) |
0.013 |
| eGFR (mL/min/1.73 m2) |
61.9±26.4 |
50.3±26.8 |
75.2±18.7 |
<0.001 |
| Hemoglobin (g/dL) |
12.9±2.8 |
11.9±3.2 |
14.1±1.3 |
<0.001 |
| Platelet count (u/μL ) |
20.3±6.6 |
19.9±7.7 |
20.8±5.1 |
<0.001 |
| Hemodialysis |
190 (5.5) |
190 (10.3) |
0 (0.0) |
<0.001 |
| Previous PCI |
1,256 (36.4) |
697 (37.9) |
559 (34.7) |
0.054 |
| Peripheral artery disease |
254 (7.4) |
189 (10.3) |
65 (4.0) |
<0.001 |
| Previous CABG |
152 (4.4) |
106 (5.8) |
46 (2.9) |
<0.001 |
| Previous MI |
1,152 (33.4) |
669 (36.4) |
483 (29.9) |
<0.001 |
| Previous stroke |
298 (8.6) |
246 (13.4) |
52 (3.2) |
<0.001 |
| Heart failure |
347 (10.0) |
271 (14.7) |
76 (4.7) |
<0.001 |
| Clinical diagnosis |
|
|
|
0.002 |
| NSTEMI |
214 (6.2) |
120 (6.5) |
94 (5.8) |
|
| SAP |
2,102 (60.9) |
1,164 (63.3) |
938 (58.2) |
|
| STEMI |
717 (20.8) |
362 (19.7) |
355 (22.0) |
|
| UAP |
420 (12.2) |
194 (10.5) |
226 (14.0) |
|
| Lesion location |
| Left main trunk |
530 (15.3) |
310 (16.8) |
220 (13.6) |
0.01 |
| Left anterior descending |
1,979 (57.3) |
1,041 (56.6) |
938 (58.2) |
0.368 |
| Left circumflex |
989 (28.6) |
532 (28.9) |
457 (28.3) |
0.735 |
| Right coronary artery |
1,534 (44.4) |
839 (45.6) |
695 (43.1) |
0.148 |
| Graft |
13 (0.4) |
10 (0.5) |
3 (0.2) |
0.152 |
| Bifurcation |
1,782 (51.6) |
931 (50.6) |
851 (52.8) |
0.217 |
| Ostial lesion |
668 (19.3) |
363 (19.7) |
305 (18.9) |
0.572 |
| In-stent restenosis |
445 (12.9) |
240 (13.0) |
205 (12.7) |
0.809 |
| Diffuse lesion |
1,487 (43.1) |
819 (44.5) |
668 (41.4) |
0.072 |
| Chronic total occlusion |
554 (16.0) |
288 (15.7) |
266 (16.5) |
0.533 |
| AHA/ACC B2/C |
2,785 (80.7) |
1,502 (81.6) |
1,283 (79.5) |
0.132 |
| Stent type |
| XIENCE |
2,155 (62.5) |
1,165 (63.5) |
990 (61.5) |
0.24 |
| ENDEAVOUR |
162 (4.7) |
85 (4.6) |
77 (4.8) |
0.899 |
| NOBORI |
1,150 (33.4) |
596 (32.5) |
554 (34.4) |
0.246 |
| PROMUS |
663 (19.2) |
365 (19.9) |
298 (18.5) |
0.325 |
| Resolute integrity |
135 (3.9) |
75 (4.1) |
60 (3.7) |
0.648 |
| Minimum stent diameter (mm) |
2.79 (0.4) |
2.77 (0.40) |
2.80 (0.4) |
0.045 |
| Total no. stents |
2.4±1.5 |
2.4±1.5 |
2.4±1.5 |
0.949 |
| Total stent length (mm) |
52.5±37.1 |
52.4±36.9 |
52.7±37.5 |
0.838 |
| IVUS use |
1,681 (48.7) |
947 (51.5) |
734 (45.5) |
0.001 |
| Rotational atherectomy |
150 (4.3) |
117 (6.4) |
33 (2.0) |
<0.001 |
| Approach site |
|
|
|
<0.001 |
| Brachial |
460 (13.3) |
279 (15.2) |
181 (11.2) |
|
| Femoral |
2,023 (58.7) |
1,105 (60.1) |
918 (57.0) |
|
| Radial |
966 (28.0) |
455 (24.7) |
511 (31.7) |
|
| Medication at discharge |
| Aspirin |
3,434 (99.4) |
1,828 (99.3) |
1,606 (99.6) |
0.526 |
| Thienopyridine |
3,439 (99.5) |
1,827 (99.3) |
1,612 (99.9) |
0.007 |
| Ticlopidine |
252 (7.3) |
148 (8.0) |
104 (6.5) |
|
| Clopidogrel |
3,187 (92.3) |
1,680 (91.3) |
1,507 (93.4) |
|
| Statin |
2,778 (80.5) |
1,357 (73.8) |
1,421 (88.1) |
<0.001 |
| β-blocker |
1,287 (37.3) |
728 (39.6) |
559 (34.7) |
0.003 |
| ACEI/ARB |
2,348 (68.0) |
1,219 (66.2) |
1,129 (70.0) |
0.021 |
| CCBs |
1,401 (40.6) |
774 (42.1) |
627 (38.9) |
0.061 |
| Oral anticoagulant |
416 (12.0) |
416 (22.6) |
0 (0.0) |
<0.001 |
| Apixaban |
5 (0.1) |
5 (0.3) |
0 (0) |
|
| Dabigatran |
17 (0.5) |
17 (0.9) |
0 (0) |
|
| Edoxaban |
1 (0.03) |
1 (0.05) |
0 (0) |
|
| Rivaroxaban |
7 (0.2) |
7 (0.4) |
0 (0) |
|
| Warfarin |
440 (12.7) |
440 (23.9) |
0 (0) |
<0.001 |
| Status of antithrombotic drugs |
|
|
|
<0.0001 |
| DAPT+OAC |
408 (11.8) |
408 (22.2) |
0 (0) |
|
| DAPT |
3,025 (87.6) |
1,418 (77.1) |
1,607 (99.6) |
|
| SAPT+OAC |
7 (0.2) |
7 (0.4) |
0 (0) |
|
| SAPT |
12 (0.4) |
6 (0.3) |
6 (0.4) |
|
| OAC |
1 (0.03) |
1 (0.1) |
0 (0) |
|
Unless indicated otherwise, values are the mean±SD or n (%). ACC, American College of Cardiology; ACEI, angiotensin-converting enzyme inhibitor; AHA, American Heart Association; ARB, angiotensin II receptor blockers; BMI, body mass index; CABG, coronary artery bypass graft; CCBs, calcium channel blockers; CKD, chronic kidney disease; DAPT, dual antiplatelet therapy; eGFR, estimated glomerular filtration rate; HBR, high bleeding risk; IVUS, intravascular ultrasound; MI, myocardial infarction; NSTEMI, non-ST-elevation myocardial infarction; OAC, oral anticoagulant; PCI, percutaneous coronary intervention; SAP, stable angina pectoris ; SAPT, single antiplatelet therapy; STEMI, ST-elevation myocardial infarction; UAP, unstable angina.
The prevalence of each major and minor risk criterion is shown in
Figure 2. Among the major criteria, severe anemia was the most commonly observed criterion. In contrast, the rates of patients with chronic bleeding diathesis, liver cirrhosis with portal hypertension, and major surgery on DAPT were each <1%. In the HBR group, the proportion of patients with ≥2 minor criteria without any major criteria, 1 major criterion and >1 major criterion were 19.5%, 22.1%, and 11.7%, respectively.
Clinical Outcomes During Follow-up
The cumulative incidence rate of the primary bleeding endpoint was much higher in the HBR than non-HBR group (13.7% vs. 5.0%, P<0.0001;
Figure 3;
Table 2). Bleeding events occurred at a relatively constant rate up to 7 years, and the annual rate of major bleeding during follow-up was approximately 2.0% in the HBR group, compared with 0.7% in the non-HBR group. The status of antiplatelet drugs at bleeding event is presented in the
Supplementary Table. The proportion of patients with DAPT at the time of primary bleeding events was 70%.

Table 2.
Cumulative Incidence of Clinical Events
| |
Total |
<1 year |
1–4 years |
>4 years |
| HBR |
Non-HBR |
P value |
HBR |
Non-HBR |
P value |
HBR |
Non-HBR |
P value |
HBR |
Non-HBR |
P value |
| Major bleeding |
199 (13.7) |
74 (5.0) |
<0.0001 |
64 (3.6) |
8 (0.5) |
<0.0001 |
78 (5.3) |
38 (2.5) |
<0.0001 |
57 (5.5) |
28 (2.1) |
<0.0001 |
| All-cause death |
706 (40.5) |
157 (10.3) |
<0.0001 |
177 (9.6) |
18 (1.1) |
<0.0001 |
282 (17.4) |
64 (4.1) |
<0.0001 |
247 (20.3) |
75 (5.4) |
<0.0001 |
| Cardiac death |
229 (15.1) |
50 (3.4) |
<0.0001 |
83 (4.6) |
13 (0.8) |
<0.0001 |
72 (4.8) |
14 (0.9) |
<0.0001 |
74 (6.6) |
23 (1.7) |
<0.0001 |
| MI |
64 (4.6) |
33 (2.3) |
<0.0001 |
22 (1.2) |
12 (0.7) |
0.16 |
20 (1.4) |
7 (0.5) |
0.009 |
22 (2.0) |
14 (1.1) |
0.02 |
| Definite/probable ST |
7 (0.5) |
8 (0.5) |
0.77 |
3 (0.2) |
5 (0.3) |
0.39 |
3 (0.2) |
2 (0.1) |
0.61 |
1 (0.1) |
1 (0.1) |
0.9 |
| Definite ST |
5 (0.3) |
8 (0.5) |
0.4 |
2 (0.1) |
5 (0.3) |
0.2 |
2 (0.1) |
2 (0.1) |
0.96 |
1 (0.1) |
1 (0.1) |
0.9 |
| Ischemic stroke |
103 (7.5) |
47 (3.3) |
<0.0001 |
35 (1.9) |
8 (0.5) |
<0.0001 |
34 (2.3) |
19 (1.2) |
0.03 |
34 (3.4) |
20 (1.6) |
0.002 |
| Cardiac death/MI/ischemic stroke |
368 (24.2) |
129 (8.9) |
<0.0001 |
136 (7.5) |
34 (2.1) |
<0.0001 |
116 (7.8) |
39 (2.6) |
<0.0001 |
116 (11.1) |
56 (4.5) |
<0.0001 |
| TLR |
221 (14.5) |
181 (11.9) |
0.045 |
131 (7.7) |
80 (5.0) |
0.002 |
61 (4.3) |
73 (4.9) |
0.44 |
29 (3.2) |
28 (2.4) |
0.6 |
Data show the number of patients with the event (cumulative incidence). Event rates were estimated using Kaplan-Meier analysis. ST, stent thrombosis; TLR, target lesion revascularization. Other abbreviations as in Table 1.
The cumulative incidence rates of the primary ischemic endpoint, all-cause death, and MI were also higher in the HBR group. In a landmark analysis, HBR patients had a consistently greater risk than non-HBR patients of the primary bleeding endpoint during the early, late, and very late periods (3.6% vs. 0.5% [P<0.0001], 5.3% vs. 2.5% [P<0.0001], and 5.5% vs. 2.1% [P<0.0001], respectively). The cumulative incidence of the primary ischemic endpoint was also higher in HBR than non-HBR patients in each follow-up period (early, 7.5% vs. 2.1% [P<0.0001]; late, 7.8% vs. 2.6% [P<0.0001]; and very late, 11.1% vs. 4.5% [P<0.0001]). The C statistics for the ARC-HBR score for a primary bleeding endpoint within 1 year, between 1 and 4 years, and between 4 and 7 years were 0.679, 0.621, and 0.620, respectively. The sensitivity, specificity, and positive and negative predictive values for the ARC-HBR scores in the early, late, and very late periods are shown in
Figure 4. Compared with the discrimination ability in the early period, there was no significant difference in discrimination ability in the late and very late periods (P=0.10 and P=0.09, respectively).
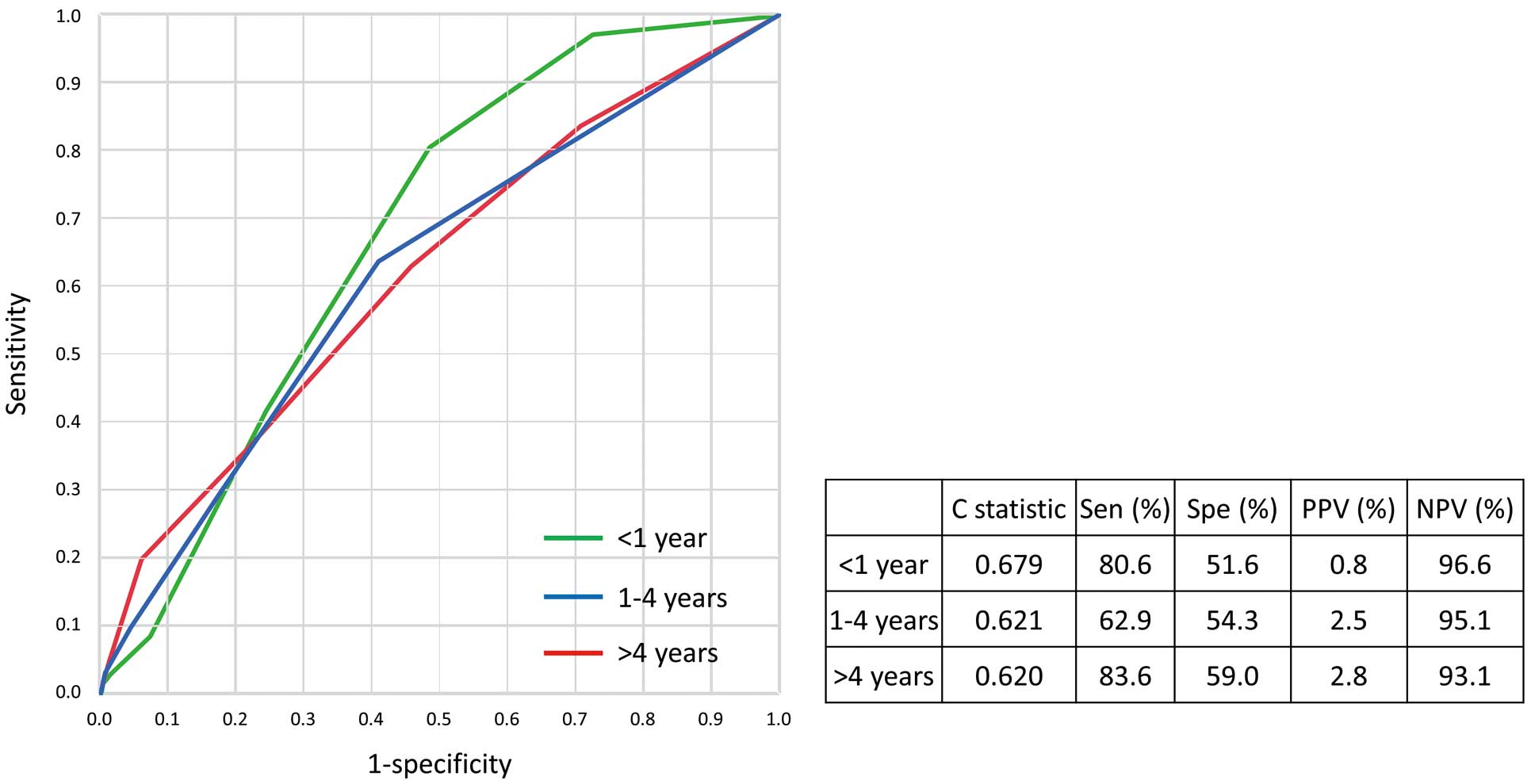
Table 3
presents the effects of individual ARC-HBR criteria on the primary bleeding endpoint during the early, late, and very late periods. In a multivariate analysis, chronic kidney disease as a major and minor criterion was associated with the primary bleeding endpoint in the early period, whereas the use of oral anticoagulants, chronic kidney disease as a major criterion, and anemia as a minor criterion were associated with late bleeding events and the use of oral anticoagulants, anemia as both a major and minor criterion, and age were associated with very late bleeding events.
Table 3.
Effect of Individual Academic Research Consortium for High Bleeding Risk (ARC-HBR) Criteria on Primary Bleeding Events Within 1 Year, Between 1 and 4 Years, and Between 4 and 7 Years
| |
<1 year |
1–4 years |
>4 years |
| HR (95% CI) |
P value |
HR (95% CI) |
P value |
HR (95% CI) |
P value |
| Major criteria |
| Oral anticoagulation |
1.57 (0.88–2.80) |
0.12 |
2.18 (1.41–3.37) |
<0.0001 |
1.90 (1.27–3.10) |
0.002 |
| Severe CKD |
2.92 (1.42–5.98) |
0.003 |
1.86 (1.10–3.16) |
0.02 |
1.18 (0.58–2.38) |
0.64 |
| Severe anemia |
1.74 (0.99–3.05) |
0.05 |
1.57 (0.91–2.68) |
0.1 |
2.24 (1.32–3.76) |
0.002 |
| Bleeding or transfusion |
3.10 (0.94–10.16) |
0.06 |
|
|
|
|
| Thrombocytopenia |
2.08 (0.82–5.25) |
0.12 |
2.18 (0.94–5.00) |
0.07 |
|
|
| Minor criteria |
| Age ≥75 years |
1.18 (0.72–1.91) |
0.51 |
1.31 (0.89–1.93) |
0.17 |
1.72 (1.18–2.53) |
0.005 |
| Moderate CKD |
2.27 (1.30–3.99) |
0.004 |
|
|
1.14 (0.77–1.68) |
0.5 |
| Moderate anemia |
|
|
1.60 (1.03–2.47) |
0.03 |
1.62 (1.06–2.48) |
0.03 |
| Stroke |
|
|
1.41 (0.83–2.43) |
0.2 |
|
|
Hazard ratios (HR) are relative to patients without each criterion; 95% confidence intervals (CIs) were estimated using the multivariate Cox proportional hazard model. Abbreviations as in Table 1.
The effects of the number of ARC-HBR criteria are shown in
Figure 5. The risk of bleeding events increased in a stepwise manner as the number of ARC-HBR criteria increased. This trend was observed in the early period, but was attenuated in late and very late periods, although the relative risk was higher for patients in the HBR than non-HBR group.
Discussion
The main findings of this study investigating the predictive value of the ARC-HBR definitions for long-term bleeding and ischemic events in patients implanted with second-generation DES can be summarized as follows:
1. The rate of the primary bleeding endpoint up to 7 years in HBR patients was nearly 3-fold higher than in non-HBR patients.
2. The ARC-HBR definition was associated with the primary bleeding endpoint not only within 1 year, but also beyond 1 year.
3. HBR patients more frequently experienced the primary ischemic endpoint throughout the 7 years of follow-up.
4. The discrimination ability of the ARC-HBR definition for the primary bleeding endpoint within 1, 1–4, and 4–7 years was comparable.
The frequency of HBR has been reported to range from 33% to 43% in all-comer registries in the US, Switzerland, China, India, and Japan if selected ARC-HBR criteria are investigated.16,21,22
In the present study, in which all ARC-HBR risk criteria were investigated, the frequency of HBR patients reached 53%, suggesting that the frequency of HBR patients may have been underestimated in previous reports using selected criteria, and that the rate of HBR patients is not low in daily practice.
Since the ARC-HBR proposal of the new definition of HBR, several studies have reported on the prevalence of the ARC-HBR criteria and their validity in predicting bleeding events.14,16–18
However, these studies assessed bleeding events mainly within 1 year. Natsuaki et al reported event rates beyond 30 days after an index PCI procedure to distinguish them from periprocedural events and found that the rate of bleeding events beyond 30 days was higher in the HBR than non-HBR group.16
In the present study we have validated the assessment of bleeding events between 1 and 4 years, as well as between 4 and 7 years, thus extending the generalizability of the ARC-HBR definition.
Interestingly, the ARC-HBR criteria were consistently associated with bleeding events during the 7-years follow-up, and their impact was not attenuated. In patients with HBR, bleeding events occurred constantly during the follow-up period. There are several possible explanations for this. First, DAPT was not discontinued as recommended in the current guideline. However, this is in line with the findings of a large multicenter trial in Japan, which found that approximately 70% of patients who experienced major bleeding were on DAPT at the time of the event.23
This low rate of persistent discontinuation of DAPT may have enhanced the difference in bleeding events between the HBR and non-HBR group. In addition, the rate of DAPT discontinuation did not differ between the HBR and non-HBR groups during the long follow-up period. The bleeding risk of patients meeting the ARC-HBR definition may not have been sufficiently taken into account during the study period. As reported previously, HBR patients are associated with traditional risk factors and ischemic events,16,18
and this was also observed in the present study. Therefore, a concern about recurrent ischemic events may have discouraged physicians from discontinuing DAPT in HBR patients. Determining the optimal duration of DAPT represents a considerable challenge, especially in patients with HBR.24–26
A recent trial that randomized patients to short- or long-term DAPT demonstrated that short-term DAPT was effective in preventing bleeding events in HBR patients.27
Further studies to investigate the long-term bleeding risk in HBR patients under current antithrombotic drug regimen are needed.
The bleeding risk in HBR patients has been reported to be 2.5- to 3.0-fold higher relative to non-HBR patients, and it has been also reported that the number of applicable ARC-HBR criteria has an additive effect on bleeding risk.17,18
These observations were confirmed in the present study. Although the discrimination ability of HBR for predicting bleeding events beyond 1 year was not statistically different from that within 1 year, the relative risk of HBR to non-HBR for bleeding events occurring beyond 1 year was numerically lower than that within 1 year. Taking this into consideration, there may be some limitations to predicting long-term bleeding events using factors collected at the index procedure because the condition of patients undergoing PCI may change during the long-term follow-up.
Study Limitations
This study has several limitations. First, the duration of DAPT in this study was different from that adopted in current practice. Second, ethnicity itself has been reported to be a risk factor for bleeding events,28,29
and the bleeding risk in the Japanese population is different from that in US and European populations. Therefore, some caution is required to extrapolate the results of this study outside Japan. Third, although we investigated all the ARC-HBR criteria using a retrospective method, the prevalence of each criterion may have been potentially underestimated. Fourth, the sample size of this study may be not large enough to accurately assess the effects of HBR and individual criteria on bleeding events beyond 1 year.
Conclusions
During long-term follow-up over a period of 7 years, the ARC-HBR definition successfully identified patients at risk of long-term bleeding. HBR was consistently associated with ischemic events throughout the 7 years.
Acknowledgments
The authors thank Miho Kobayashi, Makiko Kanaike, and Takako Yukiyoshi for their secretarial assistance.
Sources of Funding
This study did not receive any specific funding.
Disclosures
The authors have no financial associations or conflicts of interest to declare.
IRB Information
This study was approved by the Institutional Review Board of Kurashiki Central Hospital (Reference no. 3550).
Data Availability
The deidentified participant data and study protocol will be shared on reasonable request to the corresponding author. The data will become available 9 months after publication of this article, ending after 36 months.
Supplementary Files
Please find supplementary file(s);
http://dx.doi.org/10.1253/circj.CJ-21-0120
References
- 1.
Gada H, Kirtane AJ, Newman W, Sanz M, Hermiller JB, Mahaffey KW, et al. 5-year results of a randomized comparison of XIENCE V everolimus-eluting and TAXUS paclitaxel-eluting stents: Final results from the SPIRIT III trial (clinical evaluation of the XIENCE V everolimus eluting coronary stent system in the treatment of patients with de novo native coronary artery lesions). JACC Cardiovasc Interv 2013; 6: 1263–1266.
- 2.
Dangas GD, Serruys PW, Kereiakes DJ, Hermiller J, Rizvi A, Newman W, et al. Meta-analysis of everolimus-eluting versus paclitaxel-eluting stents in coronary artery disease: Final 3-year results of the SPIRIT clinical trials program (Clinical Evaluation of the Xience V Everolimus Eluting Coronary Stent System in the Treatment of Patients With De Novo Native Coronary Artery Lesions). JACC Cardiovasc Interv 2013; 6: 914–922.
- 3.
Saito Y, Kobayashi Y. Contemporary coronary drug-eluting and coated stents: A mini-review. Cardiovasc Interv Ther 2021; 36: 20–22.
- 4.
Yeh RW, Kereiakes DJ, Steg PG, Windecker S, Rinaldi MJ, Gershlick AH, et al. Benefits and risks of extended duration dual antiplatelet therapy after PCI in patients with and without acute myocardial infarction. J Am Coll Cardiol 2015; 65: 2211–2221.
- 5.
Sharma A, Agrawal S, Garg A, Vallakati A, Lavie CJ, Helft G. Duration of dual antiplatelet therapy following drug-eluting stent implantation: A systemic review and meta-analysis of randomized controlled trials with longer follow up. Catheter Cardiovasc Interv 2017; 90: 31–37.
- 6.
Mauri L, Hsieh WH, Massaro JM, Ho KK, D’Agostino R, Cutlip DE. Stent thrombosis in randomized clinical trials of drug-eluting stents. N Engl J Med 2007; 356: 1020–1029.
- 7.
Nakamura M, Kimura K, Kimura T, Ishihara M, Otsuka F, Kozuma K, et al. JCS 2020 guideline focused update on antithrombotic therapy in patients with coronary artery disease. Circ J 2020; 24: 831–865.
- 8.
Neumann FJ, Sousa-Uva M, Ahlsson A, Alfonso F, Banning AP, Benedetto U, et al. 2018 ESC/EACTS guidelines on myocardial revascularization. Eur Heart J 2019; 40: 87–165.
- 9.
Saito Y, Kobayashi Y, Tanabe K, Ikari Y. Antithrombotic therapy after percutaneous coronary intervention from the Japanese perspective. Cardiovasc Interv Ther 2020; 35: 19–29.
- 10.
Costa F, van Klaveren D, James S, Heg D, Raber L, Feres F, et al. Derivation and validation of the predicting bleeding complications in patients undergoing stent implantation and subsequent dual antiplatelet therapy (PRECISE-DAPT) score: A pooled analysis of individual-patient datasets from clinical trials. Lancet 2017; 389: 1025–1034.
- 11.
Kereiakes DJ, Yeh RW, Massaro JM, Cutlip DE, Steg PG, Wiviott SD, et al. DAPT score utility for risk prediction in patients with or without previous myocardial infarction. J Am Coll Cardiol 2016; 67: 2492–2502.
- 12.
Baber U, Mehran R, Giustino G, Cohen DJ, Henry TD, Sartori S, et al. Coronary thrombosis and major bleeding after PCI with drug-eluting stents: Risk scores from PARIS. J Am Coll Cardiol 2016; 67: 2224–2234.
- 13.
Urban P, Mehran R, Colleran R, Angiolillo DJ, Byrne RA, Capodanno D, et al. Defining high bleeding risk in patients undergoing percutaneous coronary intervention: A consensus document from the Academic Research Consortium for High Bleeding Risk. Eur Heart J 2019; 40: 2632–2653.
- 14.
Ueki Y, Bar S, Losdat S, Otsuka T, Zanchin C, Zanchin T, et al. Validation of bleeding risk criteria (ARC-HBR) in patients undergoing percutaneous coronary intervention and comparison with contemporary bleeding risk scores. EuroIntervention 2020; 28: 371–379.
- 15.
Sorrentino S, Claessen BE, Chandiramani R, Guedeney P, Vogel B, Baber U, et al. Long-term safety and efficacy of durable polymer cobalt-chromium everolimus-eluting stents in patients at high bleeding risk: A patient-level stratified analysis from four postapproval studies. Circulation 2020; 141: 891–901.
- 16.
Natsuaki M, Morimoto T, Shiomi H, Yamaji K, Watanabe H, Shizuta S, et al. Application of the Academic Research Consortium High Bleeding Risk Criteria in an all-comers registry of percutaneous coronary intervention. Circ Cardiovasc Interv 2019; 12: e008307.
- 17.
Cao D, Mehran R, Dangas G, Baber U, Sartori S, Chandiramani R, et al. Validation of the academic research consortium high bleeding risk definition in contemporary PCI patients. J Am Coll Cardiol 2020; 75: 2711–2722.
- 18.
Nakamura M, Kadota K, Nakao K, Nakagawa Y, Shite J, Yokoi H, et al. High bleeding risk and clinical outcomes in East Asian patients undergoing percutaneous coronary intervention: The PENDULUM Registry. EuroIntervention 2021; 16: 1154–1162.
- 19.
Mehran R, Rao SV, Bhatt DL, Gibson CM, Caixeta A, Eikelboom J, et al. Standardized bleeding definitions for cardiovascular clinical trials: A consensus report from the Bleeding Academic Research Consortium. Circulation 2011; 123: 2736–2747.
- 20.
Cutlip DE, Windecker S, Mehran R, Boam A, Cohen DJ, van Es GA, et al. Clinical end points in coronary stent trials: A case for standardized definitions. Circulation 2007; 115: 2344–2351.
- 21.
Sorrentino S, Claessen BE, Chandiramani R, Guedeney P, Vogel B, Baber U, et al. Long-term safety and efficacy of durable polymer cobalt-chromium everolimus-eluting stents in patients at high bleeding risk: A patient-level stratified analysis from four postapproval studies. Circulation 2020; 141: 891–901.
- 22.
Ueki Y, Bar S, Losdat S, Otsuka T, Zanchin C, Zanchin T, et al. Validation of bleeding risk criteria (ARC-HBR) in patients undergoing percutaneous coronary intervention and comparison with contemporary bleeding risk scores. EuroIntervention 2020; 28: 371–379.
- 23.
Shiomi H, Kozuma K, Morimoto T, Kadota K, Tanabe K, Morino Y, et al. 7-year outcomes of a randomized trial comparing the first-generation sirolimus-eluting stent versus the new-generation everolimus-eluting stent: The RESET Trial. JACC Cardiovasc Interv 2019; 12: 637–647.
- 24.
Sorrentino S, Baber U, Claessen BE, Camaj A, Vogel B, Sartori S, et al. Determinants of significant out-of-hospital bleeding in patients undergoing percutaneous coronary intervention. Thromb Haemost 2018; 118: 1997–2005.
- 25.
Capodanno D, Alfonso F, Levine GN, Valgimigli M, Angiolillo DJ. ACC/AHA versus ESC guidelines on dual antiplatelet therapy: JACC guideline comparison. J Am Coll Cardiol 2018; 72: 2915–2931.
- 26.
Watanabe H, Domei T, Morimoto T, Natsuaki M, Shiomi H, Toyota T, et al. Very short dual antiplatelet therapy after drug-eluting stent implantation in patients with high bleeding risk: Insight from the STOPDAPT-2 trial. Circulation 2019; 140: 1957–1959.
- 27.
Watanabe H, Domei T, Morimoto T, Natsuaki M, Shiomi H, Toyota T, et al. Details on the effect of very short dual antiplatelet therapy after drug-eluting stent implantation in patients with high bleeding risk: Insight from the STOPDAPT-2 trial. Cardiovasc Interv Ther 2021; 36: 91–103.
- 28.
Kang J, Park KW, Palmerini T, Stone GW, Lee MS, Colombo A, et al. Racial differences in ischaemia/bleeding risk trade-off during anti-platelet therapy: Individual patient level landmark meta-analysis from seven RCTs. Thromb Haemost 2019; 119: 149–162.
- 29.
Levine GN, Jeong YH, Goto S, Anderson JL, Huo Y, Mega JL, et al. Expert consensus document: World Heart Federation expert consensus statement on antiplatelet therapy in East Asian patients with ACS or undergoing PCI. Nat Rev Cardiol 2014; 11: 597–606.


