Abstract
Background: In the setting of acute myocardial infarction (AMI), there are no data regarding the benefits of intravascular ultrasound (IVUS) for chronic kidney disease (CKD) patients.
Methods and Results: This study used data from the Korea Acute Myocardial Infarction Registry, a large, multicenter prospective cohort. We evaluated 1,759 patients with AMI and CKD, defined as estimated glomerular filtration rate (eGFR) <60 mL/min/1.73 m2, and patients were classified into 2 groups: with and without IVUS. The primary outcome was target lesion failure (TLF) at 3 years. The hazard ratio (HR) of TLF according to eGFR was also analyzed. A total of 1,759 patients with AMI and CKD who underwent IVUS-guided PCI (19.2%) had a significantly lower risk of TLF at 3 years (8.9% vs. 15.3%; HR 0.55; 95% confidence interval [CI]: 0.38 to 0.81; P=0.002) than those who underwent angiography-guided PCI, regardless of their eGFR and the presence of end-stage renal disease (ESRD). The results were consistent after confounder adjustment and inversed probability weighting.
Conclusions: In patients with CKD and AMI who underwent PCI with 2nd-generation DES implantation, the use of IVUS guidance was associated with a significant reduction in 3-year TLF and showed consistently favorable outcomes regardless of eGFR and ESRD.
The most common cause of death in people with chronic kidney disease (CKD) is cardiovascular disease.1 Compared with patients without CKD, those with CKD present more complex, calcified, and extensive coronary artery disease.2 Intravascular ultrasound (IVUS)-guided percutaneous coronary intervention (PCI) is a known technique that provides more accurate lesion morphological analysis and helps stent optimization, which leads to better clinical outcomes compared with angiography-guided PCI in the drug-eluting stent (DES) area.3,4 In subgroup analyses of previous randomized clinical trials, the rate of target vessel failure in patients with CKD was significantly decreased using IVUS-guided PCI compared with angiographic guidance.5 Recently, IVUS-guided PCI with DES implantation showed better long-term clinical outcomes even in patients with acute myocardial infarction (AMI).6,7 In a subgroup analysis, the beneficial effect of IVUS-guided PCI was also observed in patients with AMI and CKD.7 However, there are few subgroup analyses regarding the benefit of IVUS for patients with CKD, and none in the setting of AMI. Therefore, this study aimed to evaluate the long-term clinical impact of IVUS guidance for 2nd-generation DES implantation in patients with both AMI and CKD.
Methods
Design and Study Population
We analyzed the data from the nationwide, multicenter prospective Korea Acute Myocardial Infarction Registry-National Institutes of Health (KAMIR-NIH) registry. Patients with AMI were enrolled in 20 major cardiovascular centers between November 2011 and December 2015. The all-clinical parameters of patients in the KAMIR-NIH registry have been described previously.8 Trained study coordinators at each center saved the data using a web-based report form on the Internet-based Clinical Research and Trial Management System. The clinical outcomes were followed up to 36 months by the attending physicians with trained coordinators using web-based standardized case report forms. It has been supported by a grant from the Korea Centers for Disease Control and Prevention since November 2011 with the Internet-Based Clinical Research and Trial Management System (iCReaT study No. C110016; cris.nih.go.kr identifier KCT0000863). The study protocols were approved by the ethics committees of each participating cardiovascular center, following the principles of the revised Declaration of Helsinki. Informed consent was gathered from all participated patients in the KAMIR-NIH.
In this study, CKD was defined as estimated glomerular filtration rate (eGFR) <60 mL/min/1.73 m2
calculated using the Modification of Diet in Renal Disease (MDRD) equation. End-stage renal disease (ESRD) was defined as eGFR <15 mL/min/1.73 m2.9 Among the 13,104 patients with AMI enrolled in the KAMIR-NIH registry, we selected 1,759 patients with CKD who underwent PCI with 2nd-generation DES implantation. The exclusion criteria were patients with cardiogenic shock, thrombolysis, no PCI or PCI without stenting, PCI with a bare-metal stent or 1st-generation DES, fractional flow reserve use or optical coherence tomography-guided PCI, and missing data, patients without CKD, and patients lost to follow-up (i.e., when the patient was safely discharged but did not visit the hospital again and unable to be contacted by telephone) (Supplementary Figure 1). Patients with AMI who underwent 2nd-generation DES implantation were managed according to the most up-to-date AMI guidelines.10,11 The choice of the preballoon size or stent size and type, interventional strategy (e.g., use of thrombus aspiration), and therapeutics (e.g., use of glycoprotein IIb/IIIa inhibitors, heparin dose) were left to each operator.
Study Outcome
The primary outcome was target lesion failure (TLF) at 3 years after PCI, defined as a composite of cardiac death, target vessel myocardial infarction (TV-MI), and ischemia-driven target lesion revascularization (ID-TLR). Death was considered as cardiac death unless the exact non-cardiac cause of death could be identified. TV-MI was considered as an MI with evidence of myocardial necrosis in the territory of the treated target vessel according to the 3rd Universal Definition of MI.12 ID-TLR was regarded as any PCI of the target lesion due to the presence of ≥50% angiographic diameter stenosis associated with symptoms of angina or a positive functional study, or a ≥70% angiographic diameter stenosis without symptoms of angina or a positive functional study. Secondary outcomes included the individual components of TLF, which was defined according to the Academic Research Consortium definition, and major adverse cardiovascular events (MACE) such as all-cause death, any MI, definite or probable stent thrombosis, and any revascularization.13
Statistical Analysis
Categorical variables are expressed as frequencies and percentages. Depending on the number of each variable, the chi-square or Fisher’s exact test was performed. Continuous variables were analyzed with descriptive methods depending on their distribution, and variables with a normal distribution are presented as means and standard deviations. Cumulative incidences of clinical events at 3 years were calculated based on a Kaplan-Meier curve, and comparisons of clinical outcomes between the IVUS- and angiography-guided PCI groups were analyzed by log-rank test. A Cox regression model with a restricted cubic spline was used to graphically display a plot of the hazard ratio (HR) across the range of eGFRs for the interaction effect of TLF between the type of guided PCI and eGFR. As differences in baseline characteristics could affect clinical outcomes, sensitivity analyses were performed to adjust for confounding factors as much as possible. First, a multivariable Cox regression model was used to assess clinical outcomes. Variables that were significant on univariate analysis (P<0.1) or important variables were included in the multivariate analysis with the following covariates: age, sex, body mass index, Killip class III as acute pulmonary edema, ST-elevation MI (STEMI), hypertension, diabetes mellitus, prior PCI, history of cerebrovascular accident, left ventricular ejection fraction ≤50%, CKD stage, statin use, multivessel disease, left main PCI, glycoprotein IIb/IIIa inhibitors, and procedural factors (transradial approach, stent diameter, stent length >60 mm, and stent number ≥3). Second, we performed inverse probability weighting (IPW) between the groups to quantitatively assess the difference between PCI strategies. The IPW of all variables was assessed using the proportional hazard regression model. The values after IPW adjustment were within ±10% across all matched covariates, demonstrating successful balance between the comparative groups (Supplementary Figure 2). All statistical analyses were performed using the survival, MatchIt, and WeightIt packages of R, version 3.6.3 software (R Foundation for Statistical Computing, Vienna, Austria).
Results
The selection of the enrolled patients is shown in Supplementary Figure 1. In total, 1,759 CKD patients with AMI underwent PCI with 2nd-generation DES implantation; 337 (19.2%) underwent IVUS-guided PCI and 1,422 (80.8%) underwent angiography-guided PCI.
Baseline Characteristics of Patients
The patients’ mean age was 70.4±10.8 years, and 1,109 (63.0%) were male. Their baseline clinical, lesion, and procedural characteristics are summarized in Table 1. The IVUS-guided PCI group had lower prevalence of Killip class III, STEMI and ejection fraction (<50%) than the angiography-guided group. For the procedural characteristics, the IVUS-guided PCI group had higher rates of left main disease, left anterior descending artery disease, glycoprotein IIb/IIIa inhibitor use than the angiography-guided PCI group. A significantly larger stent diameter and total stent number were observed in the IVUS-guided PCI group than in the angiography-guided PCI group. The rate of successful PCI was similar between groups.
Table 1. Baseline, Lesion, and Procedural Characteristics of Study Population With Chronic Kidney Disease
| |
Crude population |
IVUS-guided
PCI (n=337) |
Angiography-guided
PCI (n=1,422) |
P value |
| Demographics |
| Age, years |
69.8±11.0 |
70.7±10.9 |
0.19 |
| Male |
225 (66.8%) |
884 (62.2%) |
0.13 |
| Body mass index |
24.1±3.5 |
23.6±3.3 |
0.04 |
| Killip class III |
48 (14.2%) |
307 (21.6%) |
0.003 |
| Clinical presentation |
| STEMI |
131 (38.9%) |
658 (46.3%) |
0.02 |
| NSTEMI |
206 (61.1%) |
764 (53.7%) |
|
| Cardiovascular risk factors |
| Hypertension |
233 (69.1%) |
1,012 (71.2%) |
0.50 |
| Diabetes mellitus |
164 (48.7%) |
667 (46.9%) |
0.60 |
| Dyslipidemia |
49 (14.5%) |
155 (10.9%) |
0.08 |
| Current smoker |
75 (22.3%) |
353 (24.8%) |
0.36 |
| Previous history of MI |
35 (10.4%) |
136 (9.6%) |
0.72 |
| Previous history of PCI |
22 (6.5%) |
94 (6.6%) |
0.99 |
| Previous history of CVA |
30 (8.9%) |
170 (12.0%) |
0.14 |
| Familial history |
23 (6.8%) |
59 (4.1%) |
0.15 |
| LVEF ≤50% |
135 (40.1%) |
685 (48.2%) |
0.009 |
| eGFR, mL/min/1.73 m2 |
42.5±15.5 |
41.5±15.6 |
0.30 |
| CKD stage III |
270 (80.1%) |
1,104 (77.6%) |
0.58 |
| stage IV |
35 (10.4%) |
174 (12.2%) |
|
| stage V |
32 (9.5%) |
144 (10.1%) |
|
| Hemoglobin level |
12.5±2.2 |
12.2±2.2 |
0.12 |
| Medication at discharge |
| DAPT |
| Aspirin |
337 (100.0%) |
1,420 (99.9%) |
0.93 |
| P2Y12 inhibitor |
336 (99.7%) |
1,417 (99.6%) |
0.89 |
| Clopidogrel |
282 (83.7%) |
1,229 (86.4%) |
0.22 |
| Prasugrel |
20 (5.9%) |
103 (7.2%) |
0.47 |
| Ticagrelor |
73 (21.7%) |
256 (18.0%) |
0.14 |
| RAAS inhibitor |
271 (80.4%) |
1,107 (77.8%) |
0.34 |
| β-blocker |
273 (81.0%) |
1,176 (82.7%) |
0.51 |
| Statin |
315 (93.5%) |
1,279 (89.9%) |
0.06 |
| Lesion characteristics |
| Vessel disease |
|
|
0.09 |
| 1 |
110 (32.6%) |
551 (38.7%) |
|
| 2 |
141 (41.8%) |
519 (36.5%) |
|
| 3 |
86 (25.5%) |
352 (24.8%) |
|
| Culprit vessel |
|
|
<0.001 |
| LM |
43 (12.8%) |
55 (3.9%) |
|
| LAD |
149 (44.2%) |
601 (42.3%) |
|
| LCX |
43 (12.8%) |
222 (15.6%) |
|
| RCA |
102 (30.3%) |
544 (38.3%) |
|
| ACC/AHA B2/C lesion |
280 (83.1%) |
1,200 (84.4%) |
0.61 |
| 3 vessels treated |
16 (4.7%) |
45 (3.2%) |
0.21 |
| Procedural characteristics |
| Transradial approach |
105 (31.2%) |
397 (27.9%) |
0.90 |
| Glycoprotein IIb/IIIa inhibitor |
55 (16.3%) |
129 (9.1%) |
<0.001 |
| Thrombus aspiration |
63 (18.7%) |
294 (20.7%) |
0.46 |
| Stent type |
|
|
0.52 |
| Biolimus |
52 (15.4%) |
208 (14.6%) |
|
| Everolimus |
186 (55.2%) |
806 (56.7%) |
|
| Zotrarolimus |
81 (24.0%) |
360 (25.3%) |
|
| Sirolimus |
15 (4.5%) |
39 (2.7%) |
|
| Novolimus |
3 (0.9%) |
9 (0.6%) |
|
| Stent diameter |
3.2±0.5 |
3.1±0.4 |
<0.001 |
| Total stent length, mm |
33.0±17.3 |
31.2±15.6 |
0.08 |
| >60 |
35 (10.4%) |
108 (7.6%) |
0.12 |
| Total no. of stents |
1.7±0.9 |
1.5±0.8 |
0.002 |
| ≥3 |
58 (17.2%) |
166 (11.7%) |
0.008 |
| Successful PCI |
335 (99.4%) |
1,410 (99.2%) |
0.95 |
Values are presented as mean±SD or n (%). ACC, American College of Cardiology; AHA, American Heart Association; CVA, cerebrovascular accident; DAPT, dual antiplatelet therapy; DES, drug-eluting stent; eGFR, estimated glomerular filtration rate; LAD, left anterior descending artery; LCX, left circumflex artery; LM, left main; MI, myocardial infarction; NSTEMI, non-STEMI; LVEF, left ventricular ejection fraction; PCI, percutaneous coronary intervention; PS, propensity score; RAAS, renin-angiotensin-aldosterone system; RCA, right coronary artery; SMD, standard mean difference; STEMI, ST-elevation myocardial infarction; TIMI, Thrombolysis in Myocardial Infarction.
The median follow-up duration was 3 years (interquartile range: 2.85–3.06 years). Figure 1, Supplementary Figure 3, and Table 2 present a comparison of clinical outcomes between the IVUS- and angiography-guided PCI groups of patients with AMI and CKD. The risk of 3-year TLF was significantly lower in the IVUS-guided group (8.9%) than in the angiography-guided group (15.3%) (HR: 0.55; 95% confidence interval (CI): 0.38–0.81; P=0.002) (Figure 1A, Table 2). The results were consistent after multivariable Cox regression analysis (multivariable-adjusted HR: 0.61; 95% CI: 0.42–0.90; P=0.012) and IPW adjustment (IPW-adjusted HR: 0.58; 95% CI: 0.38–0.88; P=0.010) (Table 2). IVUS-guided PCI was significantly associated with a reduction in MACE, and all-cause death, after multiple adjustments for various confounding factors and IPW adjustment (Figure 1B, Table 2).
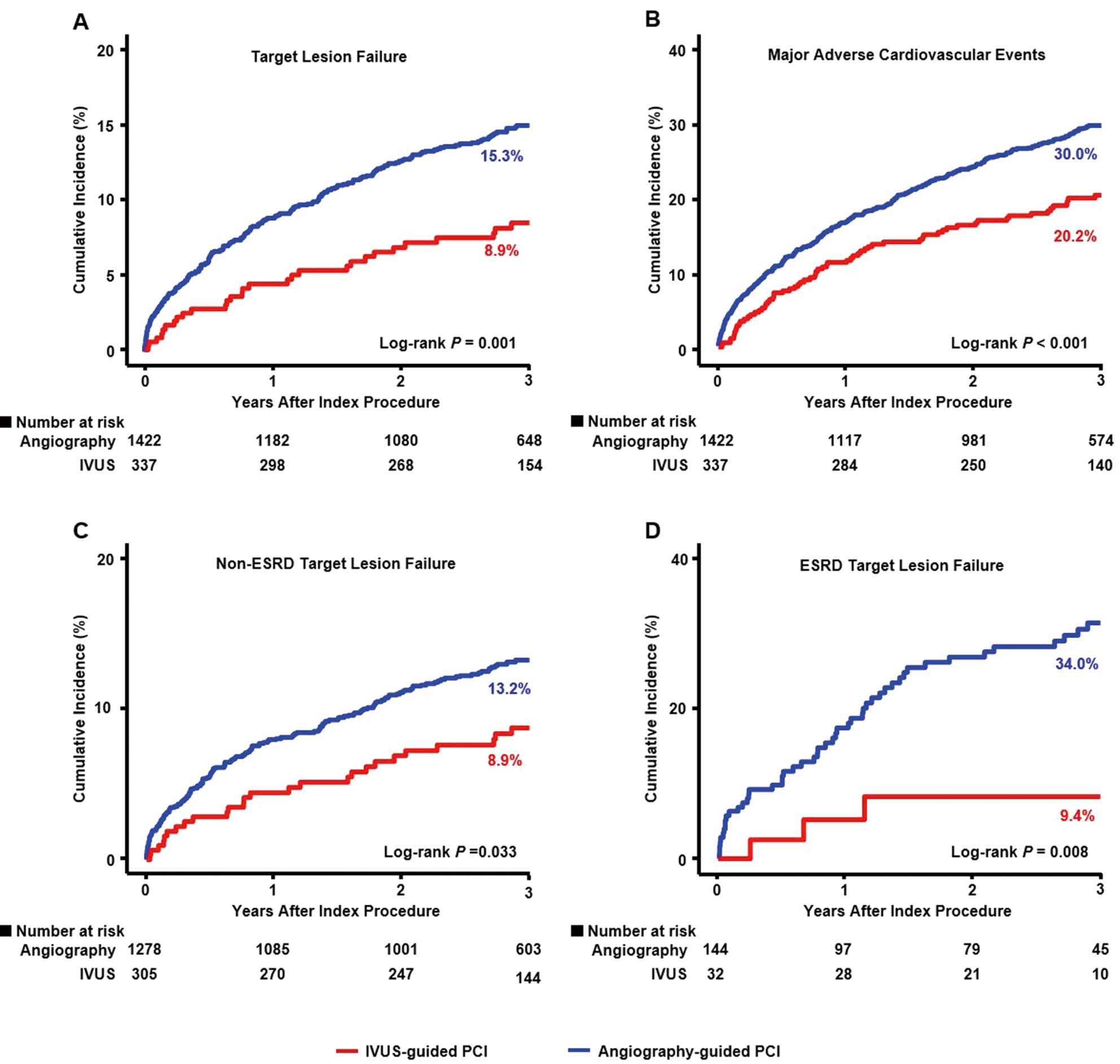
Table 2. Comparison of 3-Year Clinical Outcomes in Patients With Chronic Kidney Disease
| 3-year outcomes |
IVUS-guided PCI
(n=337) |
Angiography-guided
PCI (n=1,422) |
Unadjusted |
Multivariable-Adjusted* |
IPW-Adjusted |
| HR (95% CI) |
P value |
HR (95% CI) |
P value |
HR (95% CI) |
P value |
| Target lesion failure+ |
30 (8.9%) |
218 (15.3%) |
0.55 (0.38–0.81) |
0.002 |
0.61 (0.42–0.90) |
0.01 |
0.58 (0.38–0.88) |
0.01 |
| Cardiac death |
23 (6.8%) |
160 (11.3%) |
0.59 (0.38–0.91) |
0.02 |
0.68 (0.44–1.05) |
0.08 |
0.66 (0.42–1.09) |
0.08 |
| TV-MI |
3 (0.9%) |
32 (2.3%) |
0.38 (0.12–1.24) |
0.11 |
0.40 (0.12–1.31) |
0.13 |
0.40 (0.12–1.27) |
0.12 |
| ID-TLR |
7 (2.1%) |
55 (3.9%) |
0.51 (0.23–1.12) |
0.09 |
0.50 (0.23–1.11) |
0.09 |
0.41 (0.15–1.08) |
0.07 |
| MACE++ |
68 (20.2%) |
426 (30.0%) |
0.63 (0.49–0.82) |
<0.001 |
0.68 (0.53–0.88) |
0.004 |
0.66 (0.49–0.88) |
0.005 |
| All-cause death |
37 (11.0%) |
259 (18.2%) |
0.58 (0.41–0.82) |
0.002 |
0.65 (0.46–0.92) |
0.01 |
0.65 (0.45–0.94) |
0.02 |
| Any MI |
10 (3.0%) |
73 (5.1%) |
0.54 (0.28–1.05) |
0.07 |
0.58 (0.30–1.12) |
0.11 |
0.57 (0.30–1.12) |
0.10 |
| Any revascularization |
25 (7.4%) |
140 (9.8%) |
0.72 (0.47–1.10) |
0.12 |
0.73 (0.45–1.12) |
0.33 |
0.67 (0.43–1.05) |
0.08 |
| Definite/probable ST |
2 (0.6%) |
8 (0.6%) |
1.02 (0.22–4.79) |
0.98 |
1.11 (0.23–5.34) |
0.90 |
0.97 (0.19–5.09) |
0.97 |
Values are presented as n (%) unless otherwise indicated. +Target lesion failure: composite of cardiac death, target vessel MI, ischemic driven TLR. ++MACE: a composite of all-cause death, MI, any revascularization. *Adjusted variable: age, sex, body mass index, Killip class 3, STEMI, hypertension, diabetes, history of PCI, CVA, LVEF ≤50%, CKD stage, statin use, multivessel disease, LM PCI, glycoprotein IIb/IIIa inhibitors, and procedural factors (transradial approach, stent diameter, stent length >60 mm, stent number ≥3). CI, confidence interval; HR, hazard ratio; IPW, inverse probability weighting; MACE, major adverse cardiovascular event; MI, myocardial infarction; ST, stent thrombosis; TLR, target lesion revascularization; TV-MI, target vessel myocardial infarction.
When TLF were compared between non-ESRD and ESRD patients, the IVUS-guided PCI group showed significantly better outcomes in both non-ESRD and ESRD groups (Figure 1C,D). The restricted cubic spline curve showed the benefit of IVUS-guided PCI on the 3-year TLF across a range of eGFRs (Figure 2). However, there was no statistical difference in the HR of IVUS-guided PCI vs. angiography-guided PCI according to eGFR (P interaction=0.613).
Discussion
In this study, we compared the 3-year clinical outcomes between IVUS- and angiography-guided PCI with 2nd-generation DES implantation in patients with AMI and CKD using data from a nationwide, multicenter prospective dedicated AMI registry. The main findings of the current study were: (1) IVUS guidance was significantly associated with a lower risk of TLF and MACE at 3 years compared with angiography-guided PCI, (2) IVUS guidance was consistently associated with a reduction in the 3-year TLF in patients with AMI and CKD including ESRD regardless of eGFR (Figure 3).
Recently, nonrandomized clinical trials and subgroup analyses of AMI registry data have shown benefits of IVUS-guided PCI with DES implantation for patients with AMI and CKD.7 Furthermore, the benefits of IVUS guidance were also proven in patients with high ischemic risk, including CKD of AMI, and were more dominant among patients with CKD than among those without CKD.14
When compared with patients without renal impairment, patients with CKD are more likely to have a higher ischemic burden, including long and calcified lesions with multivessel disease, associated with periprocedural and long-term higher mortality rates.15–18 The only data on the effect of IVUS in patients with CKD are from a subgroup study5 of a randomized trial regarding IVUS vs. angiography guidance, and IVUS-guided PCI demonstrated significantly better clinical outcomes in patients with CKD in terms of ischemic events, but not in the non-CKD group. In patients with CKD, the number of stents was higher, and the stent length was longer with smaller stent diameter than in patients without CKD.5 These PCI characteristics of patients with CKD are a possible explanation for why stent optimization of IVUS is more important in patients with CKD and that the benefits of IVUS in patients with CKD are shown to be better than on those in patients without CKD. In our study using dedicated AMI registry data, when compared with angiographic guidance, the stent diameter was bigger and stent number was higher in the IVUS group, which could affect the favorable clinical outcomes in IVUS-guided PCI. Possibly the operators have to make more effort to optimize PCI using IVUS guidance for the diffuse and tight lesions of CKD even though the AMI settings. In addition, although the study did not include data on periprocedural myocardial injury, a combination of approaches, such as the use of IVUS together with optimal stenting and pretreatment with specific medications such as statins and nicorandil, may potentially contribute to improved clinical outcomes in this patient population by addressing these concerns.19–21
Our study also showed the benefits of IVUS guidance, depending on the eGFR, including ESRD state. Our analysis demonstrated the consistent effect of IVUS-guided PCI in patients with CKD and AMI, regardless of eGFR. Therefore, we suggest that the use of IVUS for patients with AMI and renal impairment, including ESRD, should be considered to achieve PCI optimization, although further randomized studies are needed to fully determine the benefits of IVUS-guided PCI in patients with AMI and CKD.
Study Limitations
First, this study had the inherent limitations of observational registry data with selection biases, because IVUS use was decided at the operator’s discretion and the exact reason for IVUS use was unknown in this registry. Second, IVUS guidance might not guarantee stent optimization, because the details of IVUS parameters such as minimal stent area or stent expansion rate or post dilatation with non-compliant balloon after stenting were not provided in the registry. Third, the present registry data did not collect the amount of contrast media used during PCI, which might affect clinical outcomes; therefore, the results should be interpreted with caution. Fourth, we did not have information on MI size assessed by cardiac magnetic resonance imaging, which is an important factor in evaluating the prognosis of AMI patients. However, we attempted to overcome this limitation by including as many factors as possible that could potentially affect infarct size in our multivariable-adjusted model to compare clinical outcomes. Fifth, our study lacked proteinuria and albuminuria data, which are crucial components in the definition of CKD. Instead, we focused on eGFR, calculated using the MDRD equation, to classify CKD stages. Despite this constraint, we believe our study still provides valuable insights into the relationship between CKD stages and clinical outcomes in patients with AMI. Sixth, calcification is a limitation of the procedure or the use of IVUS in CKD patients, but unfortunately the degree of calcification or the use of rotational atherectomy are not investigated in this registry, so we conducted this study only for patients who were successfully implanted with a 2nd-generation DES.
In this nationwide multicenter registry, IVUS guidance for patients with AMI and CKD undergoing second-generation DES implantation was associated with a lower risk of TLF at 3 years and showed consistently favorable outcomes regardless of eGFR level, including ESRD.
Acknowledgments
The authors thank the clinical investigators of the Korea Acute Myocardial Infarction Registry.
Sources of Funding
This work was funded by the Research of Korea Centers for Disease Control and Prevention (2016-ER6304-02).
IRB Information
The present study was approved by the Institutional Review Board of Chonnam National University Hospital (Reference number: CNUH-2011-172).
Supplementary Files
Please find supplementary file(s);
https://doi.org/10.1253/circj.CJ-23-0189
References
- 1.
Jankowski J, Floege J, Fliser D, Böhm M, Marx N. Cardiovascular disease in chronic kidney disease. Circulation 2021; 143: 1157–1172, doi:10.1161/CIRCULATIONAHA.120.050686.
- 2.
Madhavan MV, Tarigopula M, Mintz GS, Maehara A, Stone GW, Généreux P. Coronary artery calcification: Pathogenesis and prognostic implications. J Am Coll Cardiol 2014; 63: 1703–1714.
- 3.
Hong SJ, Kim BK, Shin DH, Nam CM, Kim JS, Ko YG, et al. Intravascular ultrasound versus angiography-guided drug-eluting stent implantation: The ultimate trial. J Am Coll Cardiol 2018; 72: 3126–3137, doi:10.1016/j.jacc.2014.01.017.
- 4.
Hong SJ, Kim BK, Shin DH, Nam CM, Kim JS, Ko YG, et al. Effect of intravascular ultrasound-guided vs. angiography-guided everolimus-eluting stent implantation: The IVUS-XPL randomized clinical trial. JAMA 2015; 314: 2155–2163, doi:10.1001/jama.2015.15454.
- 5.
Zhang J, Gao X, Ge Z, Han L, Lu S, Qian X, et al. Impact of intravascular ultrasound-guided drug-eluting stent implantation on patients with chronic kidney disease: Results from ULTIMATE trial. Catheter Cardiovasc Interv 2019; 93: 1184–1193, doi:10.1002/ccd.28308.
- 6.
Kim Y, Bae S, Johnson TW, Son NH, Sim DS, Hong YJ, et al. Role of intravascular ultrasound-guided percutaneous coronary intervention in optimizing outcomes in acute myocardial infarction. J Am Heart Assoc 2022; 11: e023481, doi:10.1161/JAHA.121.023481.
- 7.
Choi IJ, Lim S, Choo EH, Hwang BH, Kim CJ, Park MW, et al. Impact of intravascular ultrasound on long-term clinical outcomes in patients with acute myocardial infarction. JACC Cardiovasc Interv 2021; 14: 2431–2443, doi:10.1016/j.jcin.2021.08.021.
- 8.
Kim JH, Chae SC, Oh DJ, Kim HS, Kim YJ, Ahn Y, et al. Multicenter cohort study of acute myocardial infarction in Korea: Interim analysis of the Korea Acute Myocardial Infarction Registry-National Institutes of Health Registry. Circ J 2016; 80: 1427–1436, doi:10.1253/circj.CJ-16-0061.
- 9.
Stevens LA, Coresh J, Feldman HI, Greene T, Lash JP, Nelson RG, et al. Evaluation of the modification of diet in renal disease study equation in a large diverse population. J Am Soc Nephrol 2007; 18: 2749–2757, doi:10.1681/ASN.2007020199.
- 10.
Steg PG, James SK, Atar D, Badano LP, Blömstrom-Lundqvist C, Borger MA, et al. ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur Heart J 2012; 33: 2569–2619, doi:10.1093/eurheartj/ehs215.
- 11.
O’Gara PT, Kushner FG, Ascheim DD, Casey DE Jr, Chung MK, de Lemos JA, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation 2013; 127: e362–e425, doi:10.1161/CIR.0b013e3182742cf6.
- 12.
Thygesen K, Alpert JS, Jaffe AS, Simoons ML, Chaitman BR, White HD. Third universal definition of myocardial infarction. J Am Coll Cardiol 2012; 60: 1581–1598.
- 13.
Cutlip DE, Windecker S, Mehran R, Boam A, Cohen DJ, van Es GA, et al. Clinical end points in coronary stent trials: A case for standardized definitions. Circulation 2007; 115: 2344–2351, doi:10.1016/j.jacc.2012.08.001.
- 14.
Roh JW, Bae S, Johnson TW, Kim Y, Cho DK, Kim JS, et al. Impact of intravascular ultrasound in acute myocardial infarction patients at high ischemic risk. Rev Esp Cardiol (Engl Ed) 2022, doi:10.1016/j.rec.2022.10.006.
- 15.
Sarnak MJ, Amann K, Bangalore S, Cavalcante JL, Charytan DM, Craig JC, et al. Chronic kidney disease and coronary artery disease: JACC state-of-the-art review. J Am Coll Cardiol 2019; 74: 1823–1838, doi:10.1016/j.jacc.2019.08.
- 16.
Baber U, Stone GW, Weisz G, Moreno P, Dangas G, Maehara A, et al. Coronary plaque composition, morphology, and outcomes in patients with and without chronic kidney disease presenting with acute coronary syndromes. JACC cardiovasc imaging 2012; 5(Suppl): S53–S61, doi:10.1016/j.jcmg.2011.12.008.
- 17.
Moriyama T, Fukami K. Management of patients with advanced chronic kidney disease and preexisting acute myocardial infarction. Circ J 2021; 85: 1719–1721, doi:10.1253/circj.CJ-21-0394.
- 18.
Hashimoto Y, Ozaki Y, Kan S, Nakao K, Kimura K, Ako J, et al. Impact of chronic kidney disease on in-hospital and 3-year clinical outcomes in patients with acute myocardial infarction treated by contemporary percutaneous coronary intervention and optimal medical therapy: Insights from the J-MINUET study. Circ J 2021; 85: 1710–1718, doi:10.1253/circj.CJ-20-1115.
- 19.
Miyagi M, Ishii H, Murakami R, Isobe S, Hayashi M, Amano T, et al. Impact of renal function on coronary plaque composition. Nephrol Dial Transplant 2010; 25: 175–181, doi:10.1093/ndt/gfp423.
- 20.
Kono K, Fujii H, Nakai K, Goto S, Shite J, Hirata K, et al. Composition and plaque patterns of coronary culprit lesions and clinical characteristics of patients with chronic kidney disease. Kidney Int 2012; 82: 344–351, doi:10.1038/ki.2012.118.
- 21.
Ozaki Y, Hara H, Onuma Y, Katagiri Y, Amano T, Kobayashi Y, et al; Task Force on Primary Percutaneous Coronary Intervention (PCI) of the Japanese Cardiovascular Interventional Therapeutics (CVIT). CVIT expert consensus document on primary percutaneous coronary intervention (PCI) for acute myocardial infarction (AMI) update 2022. Cardiovasc Interv Ther 2022; 37: 1–34, doi:10.1007/s12928-021-00829-9.


