Thromboangiitis Obliterans ― A Disappearing Disease? ―
論文ID: CJ-23-0524
この記事には本公開記事があります。

詳細
論文ID: CJ-23-0524
Thromboangiitis obliterans (TAO) was one of the most important and common etiologies of peripheral arterial disease (PAD) in Japan in the 1970s.1 In 1972, the Japanese government established a law to provide treatment support, research support, and funding for epidemiological studies for intractable diseases, as a comprehensive support measure unlike any other in the world.2 The Guidelines for intractable disease measures defined an intractable disease as: (1) a disease with no known cause, no known treatment methods, and a high risk of permanent disability; and (2) a disease with a chronic course that is not only economically problematic but also mentally and emotionally burdensome to families because of the resources required to care for patients. Under the Guidelines, TAO was designated as an intractable disease, and patients were eligible for extensive medical support. Thus, almost all TAO patients were enrolled in this program, and the data reflected the total number of patients with TAO in Japan. However, the incidence of TAO has declined rapidly since then, although the reasons for its epidemiological transition, as well as the cause of the disease, remain a mystery. A change in the government’s policy in 2015 regarding the registration of intractable diseases has led to a tightening of the indications for patient eligibility to receive subsidies. Since then, patients who have not adequately met the indications based on the TAO diagnostic criteria and severity have been hesitant to register or continue registration, so it is possible that data reflecting the overall current status of this disease in Japan will not be available in the future. In the current issue of the Journal, Watanabe et al3 present their report based on data collected from the period just before the policy change; such data are very valuable for understanding the actual status of patients with TAO in Japan.
Article p ????
The etiology of TAO is still unknown, but is believed to be related to the pathogenesis of periodontitis.4 Owing to improvements in public health and the decrease in the number of smokers in Japan, periodontitis has become less common, and the number of patients with TAO has decreased accordingly. In severe cases, TAO progresses to loss or amputation of the fingers and toes. However, compared with atherosclerosis obliterans (ASO) the number of cases leading to major amputation is extremely small, and deaths due to TAO are considered rare; therefore, the duration of the disease may be protracted. Although the results of the present study are incomplete, because they are based on public data, and it was not intended as a medical study, it is the largest study to analyze the clinical and living conditions of patients with TAO, including long-term sufferers. It is noteworthy that the results suggest that amputation of fingers and toes may have an impact on patients’ education and employment. The results further suggest that it is important to prevent amputation and to minimize the disease’s impact on patients’ social lives through early diagnosis and therapeutic intervention, together with guidance on actions such as smoking cessation.
In recent years, progress has been made in the treatment of TAO, but the decreasing number of patients with TAO has resulted in a decreased amount of attention to the disease. TAO was once considered difficult to treat with revascularization surgery because of the risk of peripheral arterial occlusions. However, endovascular therapy5,6 and bypass surgery7,8 have shown some efficacy, and the long-term prognosis is reasonably good. We are actively performing bypass surgery in patients with this disease (Figure). In addition, there have been reports of successful results with therapeutic angiogenesis, which may become the treatment of choice in the future.9 We have experienced cases of remarkable efficacy of treatment with angiogenesis using autologous bone marrow mononuclear cell transplantation.10 Smoking cessation treatment has also progressed, and pharmacotherapy is now widely used to treat tobacco dependence as a disease, rather than relying solely on the patient’s own efforts, as was the case in the past. Previously, the Shionoya Classification, which has existed for many years, was the gold standard for diagnosis.11 However, in actual clinical practice, it is estimated that only about 30% of patients fulfill the criteria,12,13 and in Japan in recent years, only 12% of patients who were newly certified as intractable disease registrants met the criteria.14 Because of changes in dietary habits and the aging of the population in Japan, risk factors for atherosclerosis have become coexistent in many middle-aged and elderly patients, and the criteria for definitive diagnosis of TAO have been reviewed. Currently, the minimum diagnostic criteria for designation as an intractable disease are: (1) onset at <50 years of age and no risk factors for atherosclerosis, and (2) occlusion of the popliteal artery or an upper extremity artery, or a history of migratory phlebitis. However, the Japanese guidelines for PAD,15 revised in 2022, propose new diagnostic criteria that emphasize symptoms and characteristic imaging findings at the time of onset. In Europe and the USA, the age at which patients are developing atherosclerosis is decreasing, and diabetes and lipid abnormalities are currently excluded from the criteria. Establishment of diagnostic methods and standardization of diagnostic criteria are awaited.
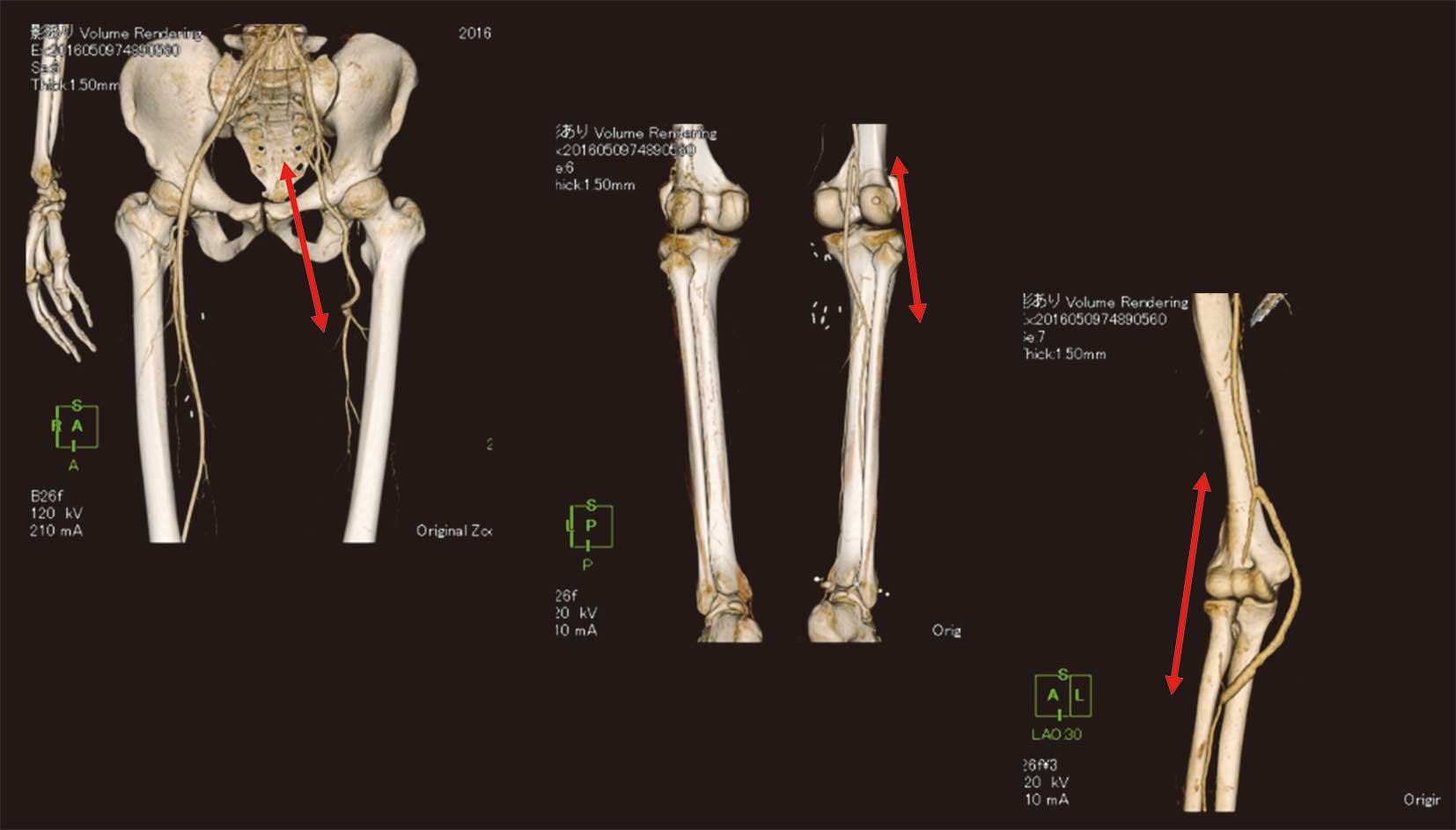
Multiple surgical bypass procedures for a single patient with thromboangiitis obliterans. (Left to Right) The patient underwent a single-staged external iliac–deep femoral artery bypass, an above-knee popliteal–tibioperoneal trunk bypass, and a brachial–radial artery bypass for multiple arterial occlusions (Red arrows).
It is still very important to differentiate TAO from other diseases such as ASO, because TAO has not yet disappeared, and appropriate diagnosis is required in an aging society and in the era of younger patients with atherosclerosis.
We thank Lorraine Law, BSc, from Edanz (https://jp.edanz.com/ac) for editing a draft of this manuscript.
The author declares that there are no conflicts of interest.
Not applicable.