Chain of Survival ― Important Role of General Citizens as Lay Rescuers ―
論文ID: CJ-23-0727
この記事には本公開記事があります。

詳細
論文ID: CJ-23-0727
Out-of-hospital cardiac arrest (OHCA) is a leading cause of death, and the number of OHCA patients is increasing every year in Japan, and cardiac OHCAs are estimated to exceed 80,000 per year in 2021.1 To improve survival with favorable neurological outcomes after OHCAs, the 2020 American Heart Association guidelines2 emphasize the important concept of the “Chain of Survival”, which includes lay rescuers. In adult cardiac arrest, the primary focus is on rapid recognition, rapid cardiopulmonary resuscitation (CPR), and defibrillation of shockable arrhythmias. This approach is based on OHCAs in adults being cardiac in origin, especially myocardial infarctions and fatal arrhythmias. The role of the general citizen as a lay rescuer in performing bystander-CPR is important, and education to motivate participation in the Chain of Survival is mandatory. The 2022 Annual Report of the Japanese Fire and Disaster Management Agency shows the importance of general citizens as lay rescuers (Figure).
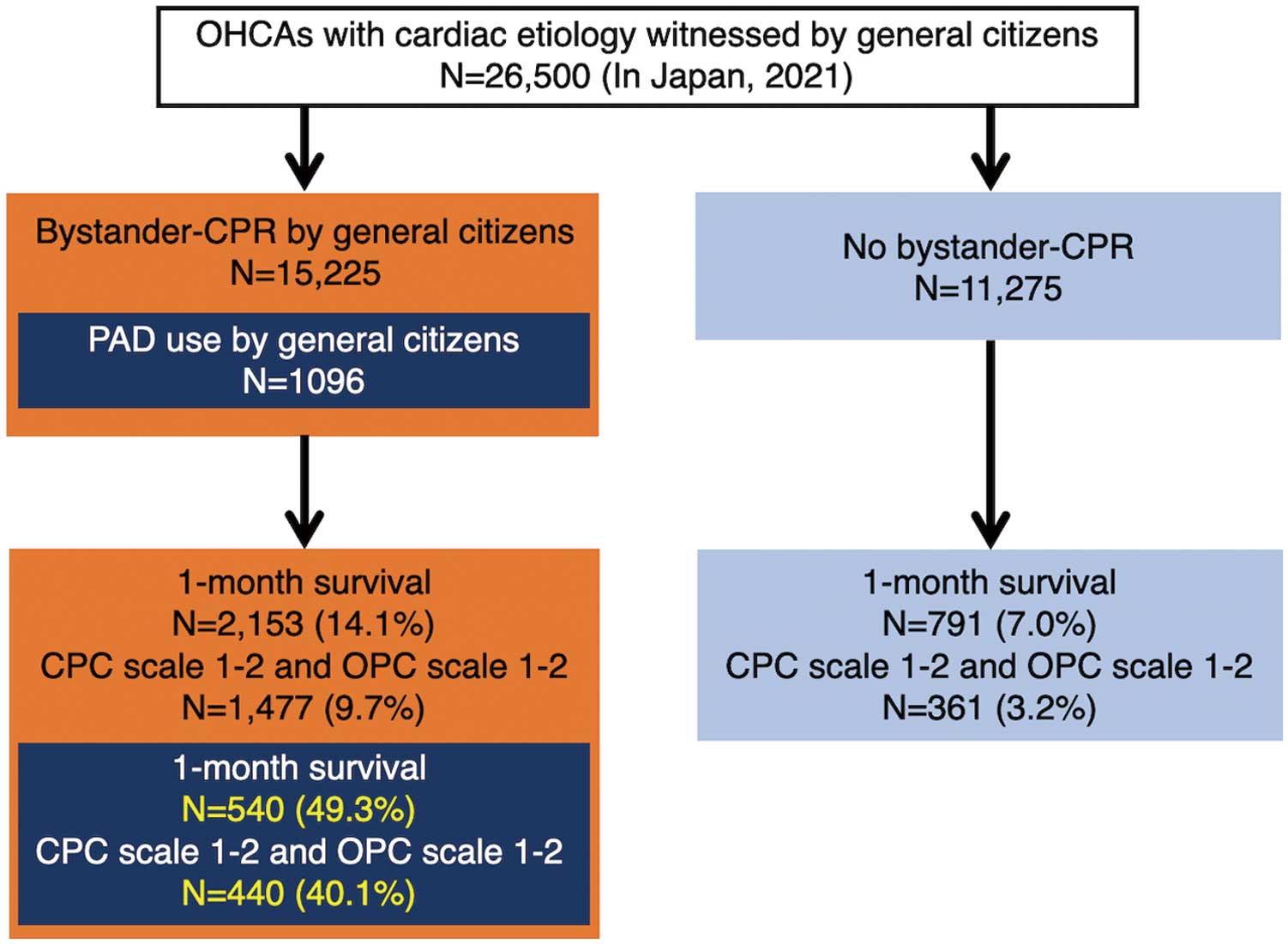
One-month survival rate by performance of CPR by general citizens. Reproduced with permission of the Japanese Fire and Disaster Management Agency.1 CPC, cerebral performance category; CPR, cardiopulmonary resuscitation; OHCA, out-of-hospital cardiac arrest; OPC, overall performance category; PAD, public access defibrillation.
Article p ????
Chest compression-only CPR (CCCPR) requires less time and effort for training than conventional CPR and has received attention for its potential to improve outcomes when used as bystander CPR.3,4 In a meta-analysis using data from 3 randomized trials, dispatcher-assisted CCCPR improved the survival in adults with OHCAs more than that with standard CPR.4 One of the benefits of CCCPR is that, for both lay rescuers and healthcare providers, avoiding ventilation during CPR may improve patient survival after cardiac arrest by minimizing the hands-off time and providing uninterrupted, high-quality chest compressions. On the other hand, in specific situations, such as remote time–distance areas, conventional bystander CPR without dispatcher-assisted CPR significantly improved survival after cardiogenic OHCAs.5
In this issue of the Journal, Kawai et al report the 10-year trend in bystander-CPR in a city where CCCPR training was widely performed in combination with conventional CPR training.6 From 2010 to 2019, a total of 168,053 inhabitants received CPR training (accounting for 41.9% of the local population: 18.2% with conventional CPR and 23.7% with CCCPR). Although CPR training was widely disseminated over the 10 years, the proportion of bystander CPR did not increase: 43.3% in 2010 and 40.0% in 2019. However, a positive change in the quality of the CPR was observed, with a significant improvement in high-quality bystander CPR (odds ratio (OR) for a 1-year increase, 1.09; 95% confidence interval (CI) 1.04–1.15, adjusted OR for a 1-year increase, 1.09; 95% CI 1.04–1.14). No improvement in either 1-month survival or 1-month survival with favorable neurological outcomes was observed. Although the results did not meet the authors’ expectations or reward the efforts of CPR training, the results were useful in understanding the outcome of local implementation of education regarding OHCAs. As in the International Liaison Committee on Resuscitation (ILCOR) advisory statement, local implementation is an important element of “the formula for survival”, together with medical science and educational efficiency.7 Considering that CPR training with CCCPR did not increase bystander CPR over the 10-year study period, long-term continued education may be needed, as well as continuous information sharing through social media.
Because general citizens play a main and important role in bystander CPR, it is important to regularly inform them that active participation in CPR training can improve both the acute survival and survival with favorable neurological outcomes of patients with OHCAs. One option is through social networking, an example being the increased use of X (previously Twitter) at scientific meetings.8,9 However, the potential risk of social networking services, such as the propagation of misinformation and copyright infringement, must be taken into consideration.9
Several issues need to be addressed. First, is anything else needed to improve the Chain of Survival for OHCAs? In the Chain of Survival, the next step after high-quality CPR is defibrillation. The proportion of shockable rhythms ranged from 5.5% to 13.9% in the present report,6 and shocks by public access defibrillators (PAD) were seldom performed (0–1.8%). Moreover, after the state of emergency declaration for COVID-19 in Japan, there was a drastic decrease in the use of PAD and that decrease was related to the decrease in the acute survival and survival with favorable neurological outcomes of patients with OHCAs, even though the proportion of bystander-initiated CPR did not change.10 This result emphasizes the importance of the use of PAD. Second, when and how should general citizens be retrained in CPR? There are few reports on repeat training sessions for CPR,11 and the optimal interval or frequency to receive CPR training to maximize motivation to participate in bystander CPR for OHCAs has not been fully elucidated. Is CCCPR training alone enough as retraining? Should there be a choice of conventional CPR training, because lay rescuers can be encouraged to perform compressions and simultaneous ventilation if properly trained, considering the potential benefits of conventional CPR outlined in the 2020 American Heart Association guidelines.2
Finally, based on the current report in a city in Japan,6 we can determine that the role of general citizens as lay rescuers was very important but not sufficient, so we cannot improve clinical outcomes after OHCAs without having a team that includes trained general citizens.
The author thanks John Martin for his linguistic assistance.
Y.M. received lecture fees from Abbott, Medtronic, and Johnson and Johnson, outside of the submitted work.