Just Because the Acute Myocardial Infarction Patient Is Simply Elderly, or Is There Something Else? ― We Need to Acknowledge Sex Differences ―
論文ID: CJ-23-0755
詳細
論文ID: CJ-23-0755
In this issue of the Journal, Shikuma et al1 present their study based on the extensive dataset of the Japanese Registry Of All cardiac and vascular Diseases-Diagnosis Procedure Combination (J-ROAD-DPC). This study is a pivotal foundation for formulating strategies addressing acute myocardial infarction (AMI) in Japan. The key finding is that female patients with AMI received suboptimal treatment compared with their male counterparts. Furthermore, the age-stratified analysis revealed female sex as an adverse prognostic factor. Previous studies have explored sex disparities in AMI from various perspectives and conventionally in Japan, AMI in women is characterized by advanced age compared with men, with a notable proportion that is ineligible for percutaneous coronary intervention (PCI), leading to poorer prognoses. A JACCS case analysis of 2,981 patients focusing on cases of coronary artery stent placement for AMI, observed that although women exhibited higher acute-phase mortality rates, sex did not emerge as an independent prognostic factor according to multivariate analysis.2 In contrast, young women with AMI presented distinct etiologies than men, with a higher incidence of conditions such as collagen diseases, coronary artery dissection, vasculitis, and the contemporary entity of Myocardial Infarction with Non-Obstructive Coronary Artery (MINOCA)3 (Figure). As a result, inferior outcomes compared with males have been reported,4 although based on limited numbers of cases, and clear-cut prognostic differences attributable to sex have not been consistently demonstrated. Due to the relatively lower incidence of AMI in women in general, any comparison with men is heavily influenced by age, and the effect on prognosis is not always discernible. Consequently, debates regarding whether female sex itself constitutes an adverse prognostic factor have risen.5,6
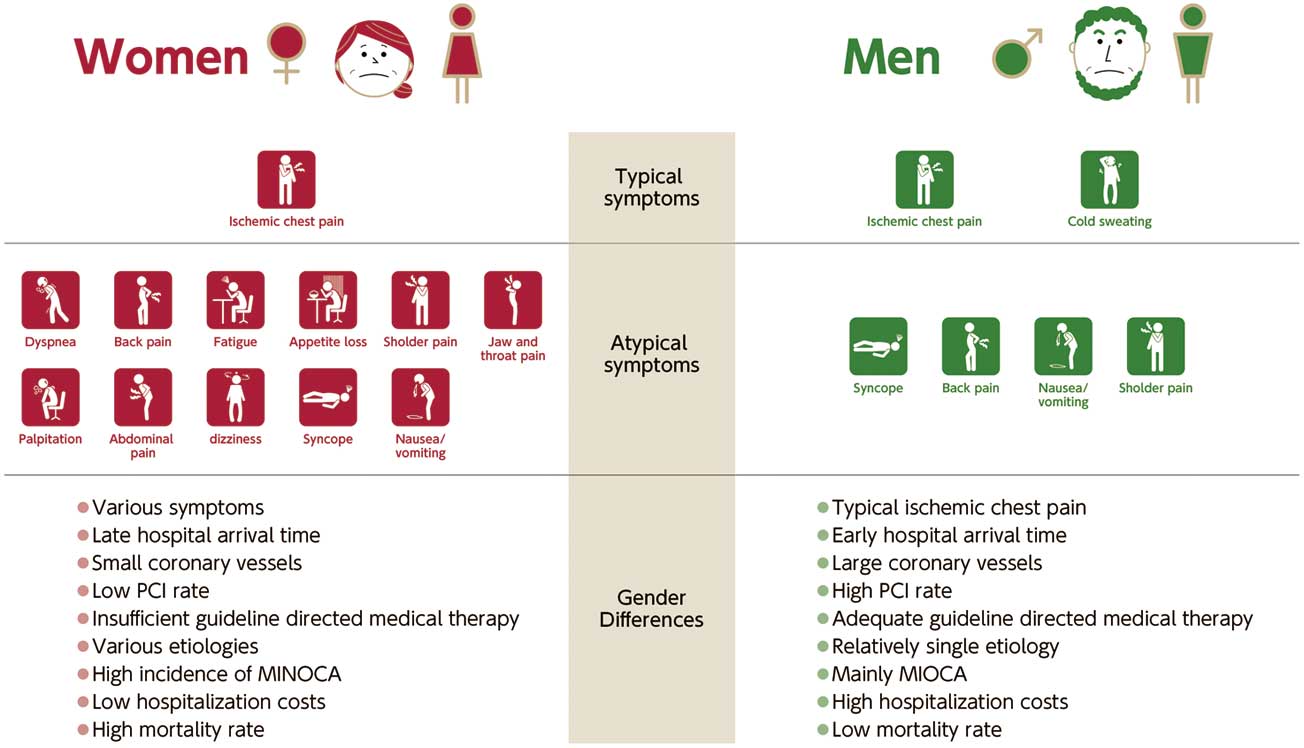
Female patients often present with symptoms that are atypical of those generally experienced by men. In addition, they frequently have a late hospital arrival time, small coronary vessels, insufficient standard drug therapy, various etiologies, high incidence of MINOCA, low hospitalization costs, and high mortality rate compared with male patients. The varied etiology includes not only atherosclerosis, but also diseases such as coronary dissection, collagen disease, and vasculitis. MINOCA, Myocardial Infarction with Non-Obstructive Coronary Artery.
Article p ????
Recent overseas reports have highlighted that women experience prolonged time to admission at PCI centers compared with men, resulting in reduced PCI rates, ultimately leading to higher in-hospital mortality rates for women.7 In Japan, the JAMIR study demonstrated that women experienced longer prehospital delay and lower coronary PCI rates than men.8 Nonspecific symptoms play a substantial role in the factors influencing treatment of female patients. Previous studies have indicated that women more often present with nausea and dyspnea, fewer episodes of sweating, and with symptoms other than “typical” ischemic chest pain9 (Figure). The descriptions of symptoms in AMI cases have primarily been those experienced by male patients, and a future emphasis on nonspecific symptoms is warranted. Additionally, unmarried women have been reported to experience prolonged time to admission compared with married females, underscoring the need for evaluation and awareness from the perspective of the social histories of women.
Furthermore, from the standpoint of healthcare providers, risk evaluation is crucial. Physicians tend to underestimate cardiovascular risks in women, resulting in suboptimal risk mitigation strategies and lower rates of standard pharmacotherapy at discharge than for men.10 Reports specifically highlight that the proportion of patients receiving standard treatment at discharge is lower for women compared with men.11 Based on the results from the present study in Japan,1 there is a pressing need for a more comprehensive approach to sex-based cardiovascular care in our country. Additionally, disparities in treatment outcomes due to absence of sex concordance between doctors and patients, as well as regional variations, should not be overlooked.12 This study has identified regional disparities in the eligibility of PCI for elderly patients. Rural areas tend to opt for conservative management without PCI,13 potentially indicating a lower likelihood of invasive treatment in elderly women compared with elderly men. Moreover, although women have fewer vessels affected by atherosclerosis, anatomically their coronary vessels are significantly smaller than those of men, potentially influencing stent and balloon size selection.14 It is imperative to acknowledge that such anatomical sex-based differences may affect the outcomes of PCI.
In Japan, the Japanese National Plan for Promotion of Measures Against Cerebrovascular and Cardiovascular Disease has been enacted, and immediate action is warranted. Female patients with AMI have a wide spectrum of underlying conditions compared with men, and their treatment and social aspects have distinctive features, necessitating multifaceted strategies. A report has suggested that treatment outcomes by female physicians may be superior to those of their male counterparts, highlighting the need for comprehensive approaches to sex-based healthcare.15 This study is an invaluable contribution to the importance of tailored interventions for women across all age groups. Next, the Japanese Circulation Society guidelines should discuss this point, and further development of research from this perspective in the future is eagerly awaited.
None.
Name of the ethics committee: N/A. Reference number: N/A.