A 71-year-old man with a history of complete atrioventricular block (CAVB), chronic atrial fibrillation (CAF), and diabetes mellitus presented with fever and shoulder pain. A permanent left-sided dual-chamber pacemaker had been implanted for CAVB 23 years ago. The last generator replacement was performed 6 years ago, but was complicated by a pocket infection, which required the new pacemaker to be implanted from the right side and removal of the left-sided generator, leaving the residual leads (Figure A). Despite the patient developing CAF, the postoperative course of the infection was uneventful after antibiotic therapy.
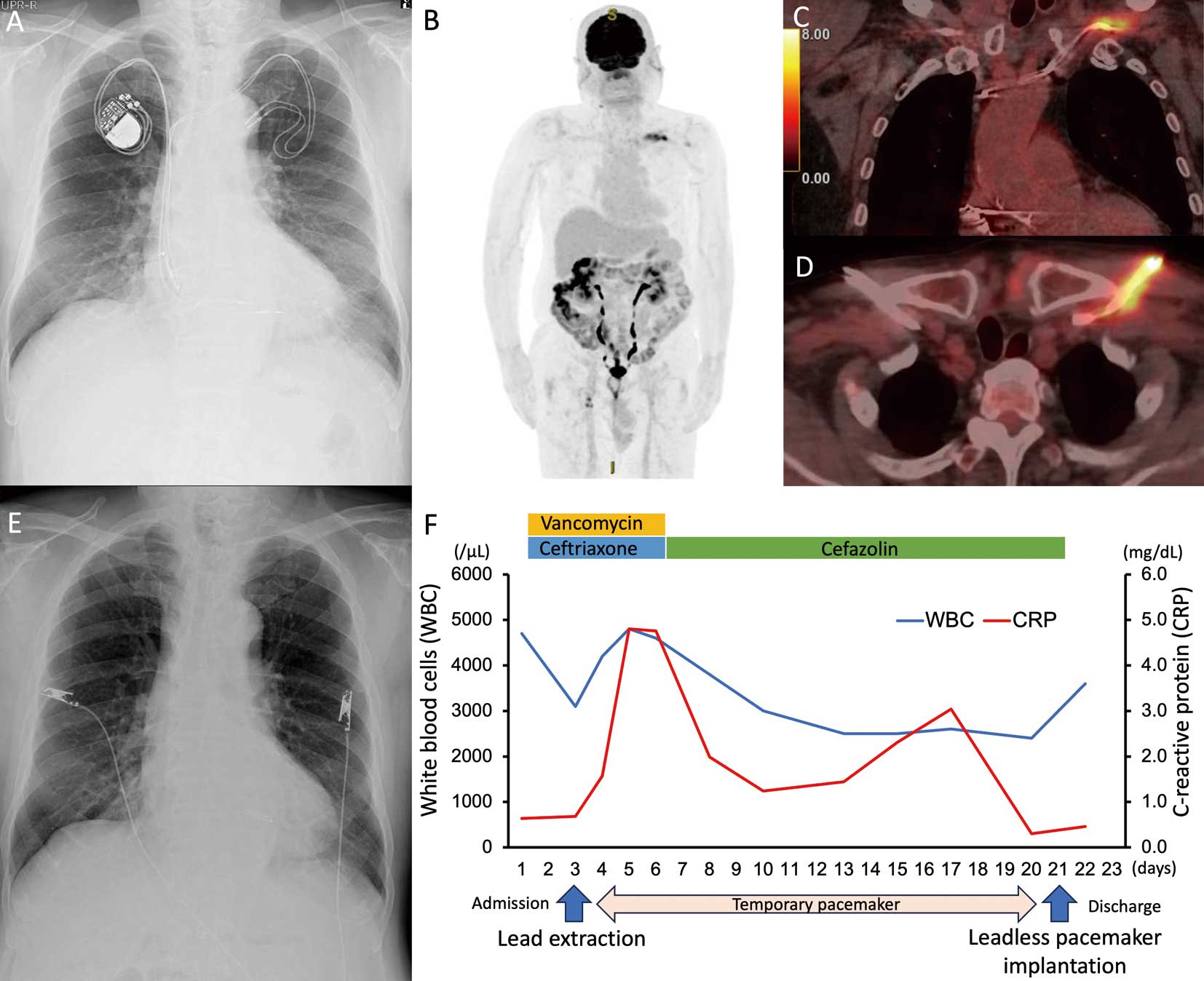
Three months before the current presentation, he underwent a tooth extraction and 1 week before presenting, he noticed fever and left shoulder pain, which was treated with analgesic and levofloxacin by his family doctor. However, his symptoms persisted, and so he presented to hospital. Physical examination revealed tenderness of the left subclavian lesion without skin erosion or redness. Laboratory data demonstrated positive inflammatory markers. Although blood cultures were negative and transthoracic echocardiography showed no vegetation, cardiac implantable electronic device (CIED) infection was clinically suspected. To confirm the diagnosis, a whole-body 18F-fluorodeoxyglucose positron emission tomography (FDG-PET) scan was performed, and there was avid uptake (maximum standardized uptake value of 7.8) along the residual leads (Figure B–D). The implanted pacemaker and residual leads were extracted, and a temporary pacemaker was placed. Staphylococcus epidermidis was identified in the culture of the residual leads. He was treated with antibiotics, and a leadless pacemaker was finally implanted after normalization of inflammatory markers (Figure E,F).
Although diagnosis of CIED infection can be clinically challenging, FDG-PET scan can detect the infection with high sensitivity even in cases of negative cultures.1
Disclosure
Y. Kobayashi is a member of Circulation Journal’s Editorial Team.