Introduction
In Japan, komb (Laminaria japonica), a type of seaweed, has been consumed for centuries. It contains a variety of active compounds such as minerals and vitamins. Kombu also contains an abundance of dietary fiber, which is expected to have effects on intestinal regulation, obesity, cholesterol levels, and so on (Anderson et al., 2009; Otles and Ozgoz, 2014; Makki et al., 2018). Therefore, it is considered that kombu is a foodstuff with health-promoting benefits, and Japanese people actively incorporate it into their diets. Recently, other functional molecules in kombu were also reported through in vitro cell culture experiments, in vivo animal experiments, and human studies. For example, a previous study found that fucoidan, which is a polysulfated polysaccharide found in kombu, exhibited antithrombotic effects in humans (Ren et al., 2013). In addition, the intake of seaweed extract containing fucoxanthin, one of the carotenoids present in kombu, promoted weight loss, reduced the amounts of body and liver fat, and improved liver function in obese non-diabetic female patients (Abidov et al., 2010). Regarding kombu itself, it was reported that the ethanol extract of L. japonica Areshoung, which is a marine vegetable that is widely consumed in Korea, had protective effects against high fat diet-induced obesity in rats (Jang et al., 2013). In addition, tororokombu, a traditional Japanese food made from edible kelp, was found to counteract the increase in serum triglyceride levels induced by the administration of corn oil to rats, and had anti-obesity effects in mice fed a high-fat diet (Miyata et al., 2009). However, the effectiveness of kombu itself has barely been evaluated in human studies. In our pilot study, we first investigated how the frequent intake of kombu affects the body. Next, we examined whether frequent kombu intake could improve blood pressure and/or the levels of blood markers associated with lifestyle-related diseases, e.g., glucose, triglyceride, and cholesterol, because the improvement of lifestyle-related diseases is considered to be one of the most urgent issues in aging societies.
Materials and Methods
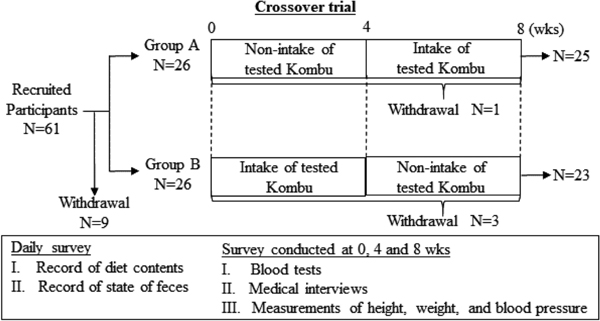
(1) Study design and subjects This study was approved by the ethics committee of Kobe University Graduate School of Medicine (#1279 & #1369). The human samples were used in accordance with the guidelines of Kobe University Hospital, and written informed consent was obtained from all subjects. The study had a randomized crossover design (Fig. 1). Sixty-one Japanese healthy adults (22 males, 39 females; age range: 34–86 years; mean age: 66.7 years) were recruited from among the general public. However, 9 subjects withdrew before the trial started. The remaining subjects were randomly divided into group A (N=26) and group B (N=26), but 4 of these subjects withdrew during the trial. Thus, 48 subjects (20 males, 28 females; age range: 39–86 years; mean age: 65.9 years) participated in the trial until its completion. Some of the subjects were taking drugs for hyperlipidemia, hypertension, diabetes, hypercholesterolemia, hyperuricemia, hyperglycemia, etc. During the treatment part of the crossover trial, the subjects consumed 6 g of roasted kombu (3 g roasted kombu k 2) (Minami Kayabe Fisheries Cooperative Associations, Hokkaido, Japan) every day for 4 weeks. Throughout the 8-week trial, the subjects recorded the contents of their diet and the state of their feces daily. Before the start of the trial (0 weeks), and at 4 and 8 weeks after the start of the trial, blood tests, medical interviews, and measurements of height, weight, pulse rate, and blood pressure were performed.
(2) Blood sampling and analysis Blood samples were collected in the morning using the standard venous blood sampling protocol. The collected blood was subjected to measurements of the following parameters: alanine aminotransferase (ALT), aspartate aminotransferase (AST), lactate dehydrogenase (LDH), g-glutamyl transpeptidase (-- GTP), blood urea nitrogen (BUN), creatinine (CRE), uric acid (UA), glucose (GLU), hemoglobin A1c (HbA1c), total cholesterol (T-Cho), high-density lipoprotein cholesterol (HDL-Cho), triglycerides (TG), white blood cell (WBC) count, red blood cell (RBC) count, hemoglobin (Hb), hematocrit (Ht), mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), mean corpuscular hemoglobin concentration (MCHC), platelet count (PLT), 1,5-anhydroglucitol (1,5-AG), insulin (INS), and C-peptide immunoreactivity (CPR). All of the above measurements were carried out by SRL, Inc. (Osaka, Japan).
(3) Medical interviews Gastrointestinal symptoms were evaluated using the Japanese version of the Gastrointestinal Symptom Rating Scale (GSRS) questionnaire. The subjects filled out the GSRS questionnaire anonymously. The GSRS questionnaire contains 15 questions, each of which is scored on a scale of 1 to 7. A higher score indicates that the relevant symptom is worse (Svedlund et al., 1988).
(4) Statistical analysis Inter-group homoscedasticity was assessed using the F-test. Then, statistical comparisons were carried out using the paired t-test or Wilcoxon signed-rank test. In all cases, p-values of less than 0.05 were considered to indicate a significant difference. The analyses were performed using the default conditions of JMP9 (SAS Institute Inc., Cary, NC) or Ekuseru-Toukei 2010 (Social Survey Research Information Co., Ltd., Tokyo, Japan).
Results and Discussion
Sixty-one subjects were recruited for this trial, 48 of whom completed it. The flow of participants through the trial is shown in Fig. 1. The aim of this study was to investigate the functionality of kombu in the general population. Therefore, in the process of recruiting the subjects, no consideration was given to the presence or absence of medication among the subjects. First, we compared the data obtained before and after the intake of kombu for 4 weeks, because some of the participants were taking cholesterol-lowering drugs, triglyceride-lowering drugs, and so on, and we considered that such evaluations were more suitable for the first step of this study than a crossover trial. The results of the blood tests and height, weight, pulse rate, and blood pressure measurements are shown in Table 1, and the results of the medical interviews are summarized in Table 2. The blood tests demonstrated that the intake of kombu for 4 weeks did not have any adverse effects on the subjects' bodily functions, for example, hemogram, hepatic functions, and kidney functions, although significant and slight increases were observed in T-Cho, HDL-Cho, and CPR levels, as were significant and slight decreases in UA levels (Table 1). Moreover, the responses to the GSRS questionnaire suggested the possibility that the intake of kombu for 4 weeks leads to relief from constipation, diarrhea, and hard stools (Table 2), indicating that frequent kombu intake may be effective at relieving intestinal ailments. In previous studies, it was demonstrated that supplementation with dietary fiber improved fecal incontinence (Bliss et al., 2001). For example, alginic acid, which is a soluble form of dietary fiber found in kombu, was suggested to improve colitis in an animal model (Razavi et al., 2008; Yamamoto et al., 2013), indicating the possibility that it induces positive bowel regulation. Kombu contains abundant amounts of fucoidan, which is also a soluble form of dietary fiber, and several reports about the biological functions of fucoidan have suggested that it may be effective at relieving intestinal ailments (Iraha et al., 2013; Lean et al., 2015). In Japan, it is traditionally considered that kombu is effective at improving intestinal regulation because it contains an abundance of dietary fiber (Anderson et al., 2009), and our results support this view. Furthermore, it was found that the intake of kombu for 4 weeks induced a feeling of fullness. As noted above, kombu contains an abundance of dietary fiber, and a previous report also indicated that the intake of fiber has the potential to induce such feelings, although the latter study did not involve dietary fiber from kombu (Bliss et al., 2011). The relationship between dietary fiber from kombu and the feeling of fullness remains unclear, but the dietary fiber contained in kombu may be involved in the feeling of fullness that participants reported after 4 successive weeks of intake. In the present study, the mean serum UA level was slightly but significantly reduced by the intake of kombu for 4 weeks (Table 1). Conversely, the mean serum levels of T-Cho, HDL-Cho, and CPR were slightly but significantly increased (Table 1). Regarding CPR, which is a marker of diabetes accompanied by obesity, liver disease, etc., the kombu-induced alterations in the subjects' CPR levels were within normal limits. The CPR results may not have clinical implications. On the other hand, the subjects' mean serum T-Cho level before the intake of kombu was inside of the standard range, and kombu intake increased it. In a previous study, kombu and alginic acid increased the plasma T-Cho levels of cholesterol diet-fed rats (Kiriyama et al., 1969), and an alginate-induced increase in serum T-Cho levels was also observed in another study (Nishide et al., 1993). In contrast, in a report by Ren et al., it was demonstrated that sodium alginate reduced serum T-Cho levels in rats (Ren et al., 1994). Thus, as inconsistent results have been obtained in animal experiments, it is difficult to explain our results regarding the subjects' serum T-Cho levels.
Table 1.
Effects of the intake of Kombu for 4 weeks on personal data and blood biochemical parameters.
|
|
Standard range
(Adults) |
Standard range
(Elderly adults) |
Pre |
Post |
P-value |
| Body weight |
kg |
|
|
60.0 |
59.9 |
0.737 |
| Body height |
cm |
|
|
159.1 |
158.9 |
0.045 |
| BMI |
|
< 24 |
< 24 |
23.66 |
23.67 |
0.787 |
| Pulse rate |
time/min |
60 – 100 |
60 – 80 |
67.9 |
68.5 |
0.684 |
| Blood pressure |
mmHg (diastolic) |
60 – 90 |
60 – 90 |
81.9 |
79.5 |
0.116 |
|
mmHg (systolic) |
100 – 140 |
100 – 140 |
142.8 |
140.2 |
0.347 |
|
|
Standard range(Males) |
Standard range(Females) |
Pre |
Post |
P-value |
| AST |
U/L |
10 – 40 |
10 – 40 |
21.5 |
22.2 |
0.157 |
| ALT |
U/L |
5 – 40 |
5 – 40 |
19.2 |
19.8 |
0.379 |
| LDH |
U/L |
115 – 245 |
115 – 245 |
188.8 |
190.5 |
0.651 |
| γ-GTP |
U/L |
≤70 |
≤30 |
32.7 |
29.7 |
0.227 |
| BUN |
mg/dL |
8.0 – 22.0 |
8.0 – 22.0 |
16.0 |
16.0 |
0.896 |
| CRE |
mg/dL |
0.61 – 1.04 |
0.47 – 0.79 |
0.79 |
0.80 |
0.296 |
| UA |
mg/dL |
3.7 – 7.0 |
2.5 – 7.0 |
5.5 |
5.3 |
0.048 |
| GLU |
mg/dL |
70 – 109 |
70 – 109 |
98.6 |
97.4 |
0.338 |
| HbA1c |
% |
4.6 – 6.2 |
4.6 – 6.2 |
5.5 |
5.5 |
0.322 |
| T-Cho |
mg/dL |
150 – 219 |
150 – 219 |
217.6 |
226.9 |
0.00005 |
| HDL-Cho |
mg/dL |
40 – 86 |
40 – 96 |
60.3 |
63.3 |
0.002 |
| TG |
mg/dL |
50 – 149 |
50 – 149 |
113.3 |
109.1 |
0.577 |
| WBC count |
/µL |
3,900 – 9,800 |
3,500 – 9,100 |
5541.7 |
5683.3 |
0.324 |
| RBC count |
×10,000 |
427 – 570 |
376 – 500 |
439.1 |
439.3 |
0.907 |
| Hb |
g/dL |
13.5 – 17.6 |
11.3 – 15.2 |
13.6 |
13.7 |
0.678 |
| Ht |
% |
39.8 – 51.8 |
33.4 – 44.9 |
40.8 |
40.7 |
0.67 |
| MCV |
fL |
82.7 – 101.6 |
79.0 – 100.0 |
93.1 |
93.2 |
0.308 |
| MCH |
pg |
28.0 – 34.6 |
26.3 – 34.3 |
31.1 |
31.2 |
0.159 |
| MCHC |
% |
31.6 – 36.6 |
30.7 – 36.6 |
33.4 |
33.5 |
0.341 |
| PLT |
×10,000 |
13.1 – 36.2 |
13.0 – 36.9 |
23.3 |
23.4 |
0.870 |
| 1,5-AG |
µg/mL |
14.9 – 44.7 |
12.4 – 28.8 |
17.2 |
17.0 |
0.278 |
| INS |
µIU/mL |
1.79 – 10.4 |
1.79 – 10.4 |
6.4 |
6.8 |
0.428 |
| CPR |
ng/mL |
0.74 – 3.48 |
0.74 – 3.48 |
1.41 |
1.65 |
0.002 |
The comparisons between the data obtained before (Pre) and after (Post) the intake of Kombu for 4 weeks were performed using the paired t-test or Wilcoxon signed-rank test, and associated p-values were calculated. The data shown in the ‘Pre’ and ‘Post’ columns are the mean values for each group. The standard ranges shown in Table 1 are used as diagnostic tools in Japan. ALT, alanine aminotransferase; AST, aspartate aminotransferase; LDH, lactate dehydrogenase; e-GTP, --glutamyl transpeptidase; BUN, blood urea nitrogen; CRE, creatinine; UA, uric acid; GLU, glucose; HbA1c, hemoglobin A1c; T-Cho, total cholesterol; HDL-Cho, high-density lipoprotein cholesterol; TG, triglyceride; WBC, white blood cell; RBC, red blood cell; Hb, hemoglobin; Ht, hematocrit; MCV, mean corpuscular volume; MCH, mean corpuscular hemoglobin; MCHC, mean corpuscular hemoglobin concentration; PLT, platelet count; 1,5-AG, 1,5-anhydroglucitol; INS, insulin; CPR, c-peptide immunoreactivity.
Table 2.
Results of the GSRS questionnaire.
|
Symptoms |
Pre |
Post |
P-value |
| Q1 |
Abdominal pain |
1.25 |
1.19 |
0.44 |
| Q2 |
Heartburn |
1.40 |
1.29 |
0.42 |
| Q3 |
Acid regurgitation |
1.29 |
1.21 |
0.16 |
| Q4 |
Sucking sensations in the epigastrium |
1.27 |
1.23 |
0.6 |
| Q5 |
Nausea and vomiting |
1.15 |
1.33 |
0.22 |
| Q6 |
Borborygmus |
1.48 |
1.60 |
0.40 |
| Q7 |
Abdominal distension |
1.23 |
1.56 |
0.008 |
| Q8 |
Eructation |
1.21 |
1.21 |
1.00 |
| Q9 |
Increased flatus |
2.02 |
2.25 |
0.22 |
| Q10 |
Decreased passage of stools |
2.33 |
1.91 |
0.02 |
| Q11 |
Increased passage of stools |
1.50 |
1.25 |
0.063 |
| Q12 |
Loose stools |
1.50 |
1.38 |
0.41 |
| Q13 |
Hard stools |
2.06 |
1.67 |
0.022 |
| Q14 |
Urgent need for defecation |
1.69 |
1.63 |
0.65 |
| Q15 |
Feeling of incomplete evacuation |
2.13 |
1.96 |
0.38 |
Each question is scored on a scale from 1 to 7. A higher score indicates that the symptom is worse. Comparisons between the data obtained before (Pre) and after (Post) the intake of Kombu for 4 weeks were performed using the paired t-test or Wilcoxon signed-rank test, and associated p-values were calculated. The data shown in the ‘Pre’ and ‘Post’ columns are the mean values for each group.
HDL-Cho is considered a beneficial cholesterol, and its increase as a result of kombu intake is desirable. In humans, it remains unclear whether kombu is associated with enhanced T-Cho level, so detailed investigations of the relationship between kombu and cholesterol in humans may need to be considered in terms of safety.
Blood test results that are outside of the standard range are recognized as signs or warnings of various diseases. Therefore, it is important to improve any abnormal values detected in blood tests. In this study, the subjects with abnormal systolic blood pressure, T-Cho, GLU, TG, INS, UA, or BMI values at the stage before kombu intake (Pre) were selected, and the effects of kombu intake on their abnormal values were evaluated (Fig. 2). In total, 25, 20, 5, 9, 3, 3, and 19 subjects exhibited abnormal systolic blood pressure, T-Cho, GLU, TG, INS, UA, and BMI values, respectively. After the intake of kombu for 4 weeks, the mean serum TG level of the subjects with abnormal values had decreased significantly (p=0.005). The mean serum insulin level of the subjects with abnormal values was also significantly reduced by kombu intake (p=0.036), although the number of subjects with abnormal serum insulin levels was low (N=3). Regarding systolic blood pressure and GLU, kombu intake tended to reduce these parameters in the subjects who exhibited abnormal values (p=0.124 and p=0.225, respectively). It was difficult to evaluate the influence of kombu intake on serum UA levels because only a few subjects displayed abnormal values (N=3), and only one exhibited a kombu intake-induced decrease in serum UA level. It could not be confirmed whether kombu intake had significant effects on the subjects' serum T-Cho levels or BMI. Based on our findings, it was suggested that kombu intake has a marked effect on high serum TG levels. In our study, a crossover trial was carried out (Fig. 1); therefore, crossover trial-based evaluations focusing on the participants with abnormal serum TG levels (N=9) were performed (Fig. 3). Of these subjects, 6 belonged to group A and 3 belonged to group B. Three (#5, #6, and #9) of these 9 participants were taking drugs for high blood pressure, hypercholesterolemia, gastritis, hepatic disorders, or pollen allergy. In a comparison between the two periods of the crossover trial, it was demonstrated that the intake of kombu for 4 weeks resulted in markedly lower serum TG levels; this result can be explained by the results shown in Fig. 2D, in which a significant decrease between Pre and Post was observed. In a previous study, seaweed supplementation significantly reduced serum TG levels, but not serum T-Cho levels, in patients with type 2 diabetes mellitus (Kim et al., 2008). That study (Kim et al., 2008) did not provide detailed information about the seaweed supplements, but seaweed including kombu might affect TG rather than other lipids such as Cho.


The reductions in the subjects' serum TG levels induced by kombu intake could have been due to the inhibition of TG absorption into the body, enhanced TG elimination in feces, or the promotion of TG metabolism, i.e., enhanced TG degradation. If kombu intake inhibits the absorption of TG into the body, our results regarding serum T-Cho levels should be similar to those for serum TG levels, because kombu contains a great abundance of dietary fiber, which is known to inhibit the absorption of T-Cho in the intestines. However, the intake of kombu for 4 weeks did not lead to decreased serum T-Cho levels. In the study by Wu and Peng (Wu and Peng, 1997), it was demonstrated that various dietary fiber molecules, such as konjac, pectin, alginic acid, and agar, decreased the serum cholesterol levels of rats fed lipid-rich diets, but did not affect their serum TG levels. In a human study, it was suggested that consuming a diet including r-glucan, which is another form of dietary fiber, induces lower serum T-Cho and low-density lipoprotein (LDL)-Cho levels, but not lower serum TG levels (Behall et al., 2004). Regarding fucoidan, it was reported that the oral administration of 500 mg once daily for 3 months decreased the serum LDL-Cho levels of obese or overweight adults (Hernández-Corona et al., 2014). In the present study, the intake of kombu for 4 weeks reduced serum TG levels, but not serum T-Cho levels, in the subjects with abnormally high serum concentrations of these molecules, so some factors other than fucoidan and alginic acid may contribute to the improvement of high serum TG levels.
The results of our pilot study suggest that frequent kombu intake may be effective against hypertriglyceridemia and intestinal ailments. Kombu has been used as a traditional foodstuff in Japan for centuries, so evaluations of its functionality in human studies are meaningful. Previously, microbes with porphyranases and agarases, which are the enzymes that metabolize polysaccharides in seaweeds, were found in the Japanese population, but were absent in North American individuals (Hehemann et al., 2010). This suggests the possibility that the effectiveness of seaweeds including kombu differs between Japanese individuals and other populations. The subjects in our study were Japanese, so cultural backgrounds need to be considered in interpreting the findings. In the crossover trial of this study, no washout period was set because the intake period was long (4 weeks), and it was not possible to force the removal of seaweeds from the diet during the study period. This point is one of the difficulties of crossover trials for foods as opposed to medicines. Although not setting a washout period may affect the results, the effects of kombu on hypertriglyceridemia could be observed in both the first and second halves of the kombu intake period. Therefore, it is considered that the effects of kombu on hypertriglyceridemia are not a problem. However, rigorous evaluations are required to clarify the functionality of kombu in humans, and our study is considered a ‘pilot study’. In the future, more detailed investigations, including studies that identify the active molecules in kombu and elucidate the molecular mechanisms underlying its functionality, are required.
Acknowledgements This study was supported by grants for project research (for the development of fundamental technology for the analysis and evaluation of functional agricultural products and functional foods) from the Ministry of Agriculture, Forestry, and Fisheries (MAFF) of Japan [M.Y.] and for AMED-CREST by the Japan Agency for Medical Research and Development [M.Y.]. We greatly appreciate the assistance of Minami Kayabe, Fisheries Cooperative Associations (Hokkaido, Japan), Akira Inoue, PhD, of Hokkaido University (Hokkaido, Japan), Takao Ojima, PhD, of Hokkaido University (Hokkaido, Japan), and Kazuki Kanazawa, PhD, of Kobe University (Hyogo, Japan).