Abstract
Objectives: Prolonged sitting with a flexed back and neck is recognized as being associated with an increased risk of neck and back pain disorders among overhead crane operators. The aim of this study was to compare back and head postures over a full shift of work between operators who experience back and neck pain, and healthy operators. Methods: In a first phase, the prevalence of musculoskeletal symptoms was assessed using the Nordic questionnaire among 120 crane operators. Based on first phase results, 17 operators with back/neck disorders were matched with 15 healthy operators based on age and selected to participate in the second phase of the study. Postures and movements were continuously measured over an 8 h shift using inclinometers. Results: The highest 12-month prevalence of musculoskeletal disorders was found in the lower back, neck and knees. Case and control groups differed significantly in back and head flexion angles at the 50th percentiles APDF (p < 0.05). There was also a significant difference in the time spent working in an extreme posture of the back and head between groups (p < 0.05). Conclusions: This is the first study to document work postures assumed during a full work shift and to compare postures between symptomatic and healthy overhead crane operators. Physical exposure in case group operators was characterized by more awkward and extreme postures in the back and head. The results of this study demonstrate that effective prevention strategies directed towards musculoskeletal disorders are required that address awkward work postures for overhead crane operators.
Introduction
Work-related musculoskeletal disorders (MSDs) affecting the back, shoulder, and neck are prevalent among workers whose work is monotonous, highly repetitive, or requires high precision1-5). Occupations that fall into these categories have higher risk for MSDS as demonstrated by epidemiological studies; these occupations include sewing machine operators, visual display unit operators, weavers, assembly-line workers, and crane operators6-8). In these occupations, workers sit for prolonged periods of time often in awkward positions, perform repeated fine movements with their upper extremities, and experience work-rest regimes that are insufficient for muscle recovery. To the lower risk of MSD, preventive programs are required that address these work factors9-12).
In this study, crane operation is considered; crane operators have an important role in many industries including those that manufacture steel products. These skilled workers are critical to both timely and safe production of steel goods. The nature of their work, however, exposes them to a higher risk for MSDs. Among operators of heavy equipment, Kushwaha and Kane12) reported that more than 90% of crane operators experience a range of MSDs with the upper back being most frequently affected (67%), followed by the neck (63%), lower back (52%), and shoulders (44%). Gustafson-Söderman13) reported that almost 70% of crane operators in their study, experienced discomfort with prolonged sitting in a forward-bent position. In a case-control study, Burdorf and Zondervan14) reported a 61% prevalence rate for lower back pain that was approximately twice as high as in their control group. With these high rates, it is evident that industries where cranes are used are faced with an ergonomic challenge that current prevention programs are failing to address successfully.
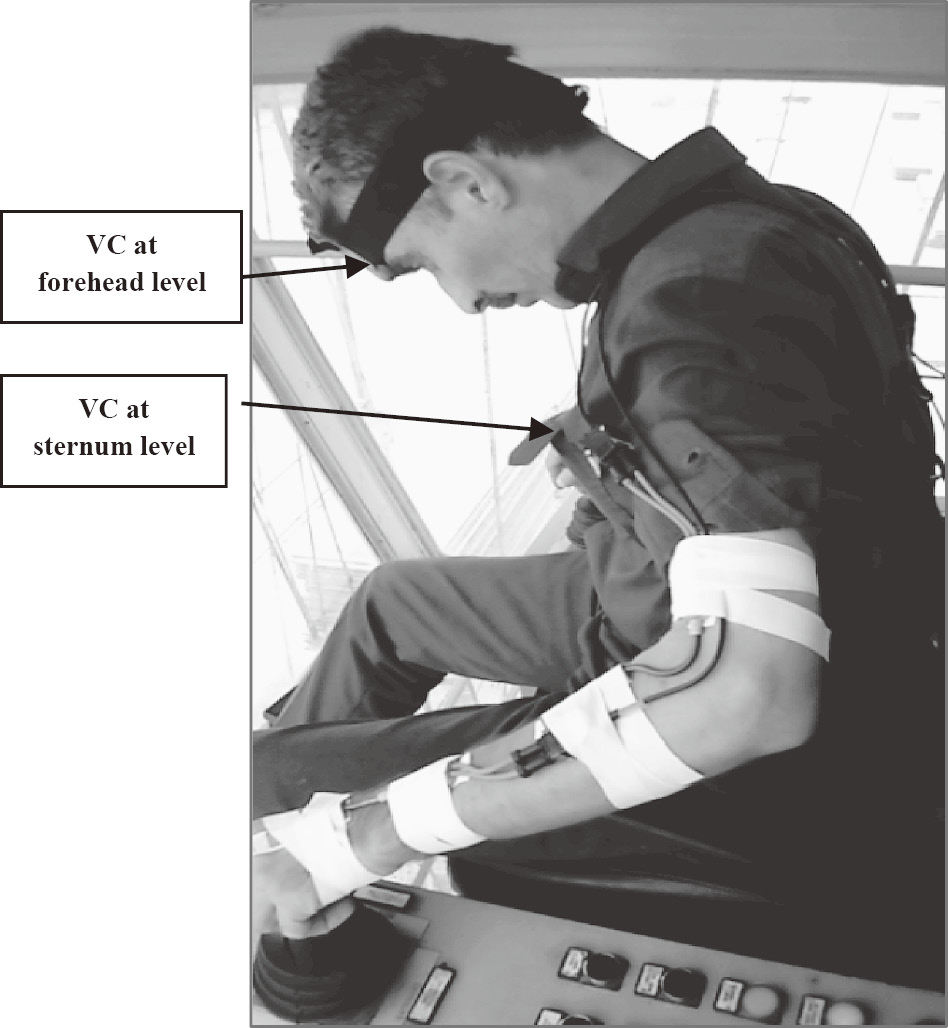
Overhead crane operators are a group of crane operators who may be at a higher risk for MSDs since they must assume an extreme forward-bent sitting position in order to view the loads being handled from the cabin that is positioned approximately 12 m above the ground (Fig. 1). Furthermore, they are required to hold this position continuously throughout the task of handling and transporting a load: The operator first positions electromagnets onto the load, then lifts the load with the crane and transfers the load to a delivery site where the load is placed, and last, releases the electromagnets from the load. While sitting in this position, the operator repeatedly moves their eyes and head to observe the load as it is handled and scan the environment for possible collisions, reaches to the controls positioned in front, and then works the controls using small reaching and hand movements12,15). Prevention strategies must therefore, center on ergonomic design of the cabin and seating.
The choice of exposure measurement methods depends on the tasks being assessed and the objectives of the evaluation. Methods should be robust enough to withstand the demands of work environments, as well as the range of worker tasks and positions.
To date, research investigations into MSDs with overhead crane operators have been qualitative in nature, using observational methods 10,12,15,16). There are only a few quantitative studies using motion capture technology. Among these, Munro M15) examined the postural demands of overhead crane operators by a video-based method. Video has been used for postural analysis in the field due to the relative simple and ease of collection and portability of equipment but it may not provide the most complete representation of posture throughout a given task or continuously during an entire work shift. Ray and Tewari16) used real time to measure work postures, but their method was observational and therefore, subject to low accuracy. Because the tasks of operators are complex (the height of loading and unloading varies) and there is no uniformity in tasks, a continuous sampling strategy is needed.
Other studies have also been conducted to evaluate musculoskeletal problems and postures of the crane operators using self-report and pen-paper based observational methods10,12), while the validity and reliability of these methods for the assessment of postural load in epidemiologic studies is probably not very high17).
Direct measurement, using inclinometers, has not yet been used to study the work demands of overhead crane operators; this methodology may reveal important findings that may help with ergonomic design because of their higher accuracy, particularly if findings are compared between symptomatic and healthy operators.
The main purpose of this study was to acquire a better understanding of the risk for MSDs by overhead crane operators. To approach this aim, several specific objectives were considered in the current study. First, a self-reported symptoms survey was done to acquire the prevalence of MSD symptoms among overhead crane operators. The second objective was to acquire an accurate record of trunk and head postures assumed by overhead crane operators throughout a full shift of work using on-body inclinometers. Then results were compared between operators who reported MSD symptoms and those who had no symptoms using a case-control method. Results from this study are expected to provide valuable information for the development of cost-effective MSD prevention strategies for overhead crane operators. These strategies may also be applied to other occupations with similar work demands and in which workers also experience high rates of MSDs.
Materials and Methods
This investigation took place at four steel manufacturing sites in two phases. The sites produced steel plates, black plates, and rebar. Overhead cranes were used to transport steel, hot slab, hot rolled coil, cold rolled coil, and other materials across the sites. The cabs where the operators sat and worked were similar across the four sites in respect to ergonomic chair, air conditioning, and visibility. Both static and moving overhead cranes were used at each site, with the latter being more frequent. At least 85% of the cabins on the cranes were positioned 12 m off the ground. In the first phase, overhead operators were asked to report on musculoskeletal discomfort and related absences in the previous 12 months; in the second phase, sitting postures were measured and then compared for operators with and without reported musculoskeletal symptoms using case-control methodology.
All participants in both phases were currently employed, and volunteered to participate. Before commencing each study, all participants received an explanation of the study objectives, how information would be handled, and the methods used; each participant provided written informed consent, which was pre-approved by the Ethics Review Committee of the Tehran University of Medical Sciences.
Phase 1
Participants
One-hundred and twenty (120) overhead crane operators participated. Their mean age was 33.04 ± 5.4 (mean ± standard deviation (SD) ) years, and mean work experience was 10.4 ± 4.7 years. The mean height was 174.1 ± 5.6 cm, and the mean body mass was 72.6 ± 7.04 kg.
Procedures
Musculoskeletal symptoms were assessed in the previous 12 months through an interview by the use of the Standardized Nordic Musculoskeletal Questionnaire (SNMQ) that was translated into Farsi language18). The questionnaire included two sections. The first section included demographic characteristics. The second section included questions about musculoskeletal symptoms experienced during the past year. Furthermore, the subjects were asked about sick-leave due to the complaints and they were asked whether the complaints were work related (i.e., caused by, or associated with work).
Phase 2
Participants
Participants were selected from those who had participated in Phase 1, and who had been working full time (~40 h/week) for at least 12 months. Participants were assigned to the control group if they had no current or previous history of neck or back pain within the prior 12 months based on responses to the SNMQ, company medical records and sick absences. Among the 120 operators who participated in Phase 1, 15 operators met this criterion. Seventeen operators were then selected for the case group based on age-matching. Table 1 shows the demographics for each group.
Table 1.
Mean (SD) demographics for the case and control groups
|
Age (years) |
Height (cm) |
Body mass (kg) |
Work experience (years) |
| Case (n=17) |
36.8 (3.4) |
173.1 (3.7) |
74 (3.6) |
10.8 (2) |
| Control (n=15) |
35.6 (4.4) |
176.2 (3.8) |
75.1 (3) |
8.3 (3) |
Head and trunk inclination in the sagittal and transverse planes were recorded continuously over an 8-h period while operators performed their normal assigned duties. Head and trunk flexion/extension and lateral bend angles were recorded using Virtual Corset (VC) tri-axial accelerometers (Microstrain,Williston,VT, USA). The VC is a wireless, battery-operated, lightweight (6.8 × 4.8 × 1.8 cm, 72 g), portable logger with 2 MB of onboard memory. Tri-axial accelerometers were validated in vitro for measuring velocity and postural data under static and dynamic conditions. The RMS angle error for static and dynamic conditions predicted was 1º and 3º, respectively19,20).
Two inclinometers were used: One was positioned on the forehead using double sided adhesive tape, and the second was positioned over the sternum using strapping to secure the device against erroneous movement. Prior to data collection, a reference upright standing position was recorded with participants instructed to stand upright and look at a mark on the wall that was positioned at eye level.
Throughout testing, data was logged using a portable logger with 2 MB of onboard memory at a sample rate of 7.5 Hz. Upon completion of testing, the raw signals were downloaded to a personal computer for analysis. Prior to signals analysis, inclinometer signals were filtered with a low pass of 3 Hz and a fourth order Butterworth filter7). The data was then normalized to the upright standing position that was recorded prior to testing. The head and trunk angles were then converted to an amplitude probability distribution functions (APDF) for comparison. The 10th, 50th, and 90th percentiles of the APDF were extracted and categorized as "low", "median", and "peak" angle, respectively. All signal processing and data calculations were completed using custom-written programs developed in Matlab R2007B (The Math Works Inc., Natick, MA, USA).
Statistical analysis
All statistical analyses were performed using SPSS 22.0 (SPSS Inc., Chicago, IL, USA). The Kolmogorov-Smirnov test was used to examine the normality of the distribution of data and the Shapiro-Wilk test was used for further confirmation. All data proved to be normally distributed. Paired t-tests (two-tailed) were then used to evaluate differences in head and trunk posture between the study and control groups. The significance level was chosen to be 0.05 (or equivalently, 5%). Further examination for influence from demographic factors was conducted using Spearman's correlation coefficients (rS).
Results
Phase 1: Prevalence of musculoskeletal symptoms
The prevalence of musculoskeletal symptoms among this group of overhead crane operators was high with almost every participant reporting some discomfort in one or more regions of the body. The most frequently reported symptomatic region was the lower back, followed by the neck with over 75% of participants reporting that they had experienced discomfort in each region within the previous 12 months or were currently experiencing discomfort (Table 2).
Table 2.
Prevalence (%) of musculoskeletal symptoms during the past 12 months (n=120)
| Body Region |
Participants (%) |
| Neck |
75.8 |
| Shoulder |
|
|
Dominant (right) |
15.8 |
|
Non-dominant (left) |
35.8 |
|
Both |
11.7 |
| Elbow |
|
|
Dominant (right) |
18.3 |
|
Non-dominant (left) |
0.8 |
|
Both |
18.3 |
| Wrist/hand |
|
|
Dominant (right) |
25.0 |
|
Non-dominant (left) |
9.2 |
|
Both |
31.7 |
| Upper back |
30.8 |
| Lower back |
85.8 |
| Hip/thigh |
31.7 |
| Knee |
68.3 |
| Leg/feet |
11.7 |
The difference in mean values for the median flexion angle of the trunk between the case and control groups was 4.7° with the case group sitting in a further forward-bent position (Table 3); this difference was significant (p = 0.04). A similar difference was observed for peak flexion with the mean difference being 5.4° (p = 0.02). Moreover, the time spent working in these postures was greater for the case group with significant differences observed for extreme and highly extreme postures (p = 0.05).
Table 3.
Mean (SD) postures and movements of the trunk and head, in 17 operator cases with symptoms and 15 operator controls without symptoms
|
|
Case Mean (SD) n=17 |
Control Mean (SD) n=15 |
Difference between Groups |
*p<0.05, statistically significant differences between cases and controls.
Negative values denote postures in extension and left bend, positive values in flexion and right bend. |
| Trunk-Flexion (˚) |
|
|
|
|
APDF 10th |
–5.6 (4) |
–3.4 (6) |
2.2 |
|
APDF 50th |
36.8 (7) |
32.1 (5) |
*4.7 |
|
APDF 90th |
49.4 (9) |
44.0 (6) |
*5.4 |
|
APDF 10th-90th |
53.3 (8) |
47.5 (7) |
5.8 |
|
Time spent in flexion (%) |
|
|
|
|
neutral (<20˚) |
48 (4) |
45 (6) |
3 |
|
extreme (>45˚) |
24 (5) |
20 (3) |
*4 |
|
highly extreme (>60˚) |
5 (2) |
3.6 (1) |
*1.4 |
| Trunk-Lateral bend (˚) |
|
|
|
|
APDF 10th |
–1.1 (4) |
–0.6 (3) |
0.5 |
|
APDF 50th |
7.1 (2) |
6 (5) |
1.1 |
|
APDF 90th |
9 (2) |
10 (3) |
1 |
|
APDF 10th-90th |
10.7 (3) |
10.9 (5) |
0.2 |
|
Time spent in lateral bend (%) |
|
|
|
|
Neutral (<10˚) |
96.4 (1) |
95.7 (3) |
0.7 |
| Head-Flexion (˚) |
|
|
|
|
APDF 10th |
5.8 (5) |
4.8 (2) |
1 |
|
APDF 50th |
28.6 (6) |
23.4 (4) |
*5.2 |
|
APDF 90th |
37.2 (7) |
33.6 (5) |
3.6 |
|
APDF 10th-90th |
29.2 (5) |
28.8 (6) |
0.4 |
|
Time spent in flexion (%) |
|
|
|
|
neutral (<20˚) |
43.6 (6) |
46.8 (7) |
3.2 |
|
extreme (>45˚) |
28.2 (8) |
22.8 (5) |
*5.4 |
| Head-Lateral bend (˚) |
|
|
|
|
APDF 10th |
–2.4 (6) |
–2.9 (6) |
0.5 |
|
APDF 50th |
13.5 (3) |
11.3 (4) |
2.2 |
|
APDF 90th |
17.3 (4) |
15.5 (2) |
1.8 |
|
APDF 10th-90th |
19.3 (8) |
10.9 (5) |
8.4 |
|
Time spent in head-Lateral bend (%) |
|
|
|
|
Neutral (<10˚) |
75.3 (5) |
76.2 (5) |
1.1 |
|
Extreme (>20˚) |
3.6 (2) |
2.3 (2) |
1.3 |
| Movement velocities (˚/s) |
|
|
|
|
APDF 10th |
1.7 (0.1) |
1.1 (0.1) |
0.6 |
|
APDF 50th |
13.8 (2) |
11.7 (2) |
2.1 |
|
APDF 90th |
35.7 (7) |
34.2 (6) |
1.5 |
Similar trends appeared for head flexion between the case and control groups although the differences were significant only for the median head flexion angle (p = 0.05). A significant difference emerged for time spent sitting with the head at an extreme angle with the case group spending a mean difference of 5.2% of their time with the head flexed greater than 45° (p = 0.04).
Lateral bend of the head and trunk remained relatively neutral throughout the entire shift with no significant differences emerging between the case and control groups. The power of the test for the median trunk and head lateral bend was 0.84 and 0.71, respectively. There was no significant difference in head angular velocity between groups. The power of the test for median head angular velocity was 0.89.
Lateral flexion and posture ranges for the head were similar in the two groups.
There were no significant correlations between head and trunk posture and age and work experience. Negative correlations between stature and median trunk flexion were found, although not statistically significant (rS = -0.35, p = 0.09, Table 4).
Table 4.
Correlation
1 between median trunk and head flexion and demographic characteristics of the crane operators (n=32)
| Variable |
Age |
Height |
Work experience (years) |
| Trunk-Flexion (˚) |
rS=0.03 (p=0.6) |
rS=–0.35 (p=0.09) |
rS=–0.15 (p=0.19) |
| Head Flexion (˚) |
rS=–0.13 (p=0.46) |
rS=0.16 (p=0.38) |
rS=0.14 (p=0.28) |
Discussion
The prevalence of MSDs was investigated among overhead crane operators in Phase 1 with the results showing a high 12-month prevalence of MSD symptoms affecting the upper body; the highest rates were recorded for the lower back and neck. In Phase 2, the trunk and neck postures were continuously recorded for an entire shift for two groups of operators: those with MSD symptoms and healthy operators. The kinematic results revealed that overhead crane operators with back and neck symptoms perform their work with significantly different trunk and neck postures compared to healthy operators.
Methodological considerations
The main characteristics of the present study that distinguishes it from existing research are threefold: a case-control approach, direct methods using inclinometers, and continuous measurement over an entire shift. It is well established that work factors such as visual requirements during loading and unloading, design and layout of the control panel, and the use of control levers by both hands can lead to long-term awkward work postures and ultimately to constrained postures; however, the detail of exposure to awkward sitting was limited owing to methodologies being observational or using video capture. In this study, back and head postures were measured using a digital inclinometer, which has been shown to have high accuracy and high reliability19). This approach revealed small differences between case and control groups which could be easily addressed in ergonomic design and work-rest regimes.
Musculoskeletal symptoms
Higher rate of MSDs, experienced by crane operators were shown in several preceding studies10,12,21). The findings in current study show that overhead crane operators have extremely high rates of MSDs, with almost all study participants reporting that they had experienced pain in at least one part of the body in the previous 12 months. This higher rate of MSD prevalence was comparable to those reported by Ray and Tewari16), who showed that 90% of crane operators in a metal manufacturing center in India had reported experiencing pain in the previous year using a modified Borg scale. Their results showed that pain appeared quickly, and reached a maximum level after 2.5 h of continuous work16), suggesting lengthy or extremely awkward work postures. The full day monitoring of work postures in Phase 2 of this study supports this conclusion with the results showing awkward trunk and head postures for most of the day.
Lower back pain showed the highest prevalence (86%) in this study, followed by the neck (76%) and knees (67%). Kushwaha and Kane12) also showed that that these same regions were most frequently affected; however, their rates were lower than those recorded here: lower back (52%), neck (63%) and knee pain (59%). Courtney and Chan22) reported similar rates to this study: lower back (88%), neck (81%), and upper back/shoulder pain (50%). Differences between studies may have occurred because of differences in the definitions of pain or discomfort. This study used a well-established discomfort questionnaire to assess musculoskeletal pain conditions rather than a modified effort scale, and therefore, these results should reflect a true picture of MSDs in the workplace. A second reason for variability is the study participants; this study addressed exclusively overhead crane operators who require a more extreme sitting position because of the visual requirements and the overhead location of the crane cabin. As a result, it was expected that prevalence would be higher in this study compared to those addressing MSDs with crane operators. Overall, the literature continues to show alarming high rates of MSD symptoms for crane operators.
In comparison to other sitting jobs previously identified as high risk work, overhead crane operators have higher rates of MSD symptoms: VDT operators23), dentists24), office workers25), and professional truck drivers26). Lower back pain in particular is higher compared to other sitting jobs including urban taxi drivers, professional truck drivers26,27), office workers25), and tractor drivers28,29). This may be due to more extreme postures or longer durations; further investigation comparing different occupations is required to determine if overhead crane operators are a unique subset of the occupations described as monotonous, highly repetitive, and requiring high precision. If this is the case, then prevention strategies borrowed from other occupations may be ineffective.
Postures and movements of the trunk and head
Awkward trunk and neck postures have been identified as one of the important risk factors in the development of trunk and neck pain in crane operators16,21); long durations of neck flexion greater than 20° are a contributing factor for neck and lower back pain30-32). The results showed that the trunk flexion angle was generally greater for the case group compared to the control group with significant differences observed between the two groups. Furthermore, the difference in the mean percentage of time was 4% and 1.4% for extreme and highly extreme postures, respectively. According to the study conducted by Beach and Parkinson33), long-term sitting in awkward postures, for 20 min or more, lead to the development of the mental and physical fatigue. Furthermore, the changes in the soft tissues of the trunk were observed after spending 5-20 min of constant trunk flexion. Since long durations of non-neutral, static postures leads to fatigue and muscular discomfort28), it is not surprising that the prevalence of lower back pain in overhead crane operators is high.
In this study, the mean stature of the case group was shorter (about 3.1 cm) compared to the control group; although, this difference had no significant influence on trunk flexion, there was a tendency for shorter operators to sit in more flexion than taller subjects. Therefore, the difference in stature between case and control groups may be one of the factors contributing to the postural differences between groups, which may be related to visual field. Crane operators require high visibility and attention in order to safely transport materials using the crane. Studies have shown that high demands on concentration and visibility can be an important factor on trunk posture with greater flexion assumed while performing tasks with high precision requirements15). However, one of the challenges is controlling for other influential factors given the high rate of MSDs in this work population. Therefore, further investigation into the effect of stature may reveal valuable information.
The findings of this study showed that overhead crane operators worked with the neck flexed more than 20° for large amounts of their work time and that the case group spend a greater proportion of their work time with the head flexed beyond 45°. According to a prospective study by Ariens and Bongers30), an increased risk for neck disorders was found in participants in various jobs, working with the neck flexed more than 20° for at least 70% of the working time.
It has been documented that a difference of about 5° in neck flexion angle may have a significant impact on the neck extensor moment and the muscle loads required from the neck extensors to support the weight of the head34). Hence, the present finding of about 5.4 difference in median head flexion angle between case and control groups may be of clinical importance, indicating that case operators had to sustain a greater neck extensor moment during work time.
In both groups, low angular velocity and lack of postural variation for the head, showed that working postures used by overhead crane operators are constrained which is a recognized risk factor for MSD affecting the neck35,36). In the case-control comparison, despite the higher angle of the head in the case group, there was no significant difference in angular velocity between the two groups. This could be an important finding; however, it is unknown if this change is an adaptive response to MSD symptoms or a true difference in working postures; a prospective study is required to determine if this is a potential approach for a prevention strategy.
In the present study, there were no significant difference between the case and control groups in some percentiles due to the small differences in physical exposure, and when there was a significant difference, the difference was small. These results are probably not associated with an increased risk of MSD, but they might indicate differences in variability of motor performance. For example, individuals with a larger motor variability show a higher probability of returning to normal postural strategies after experimental back pain than individuals with less flexibility37). Hägg and Åström38) conducted a case-control study among medical secretaries and found that the proportion of rest in the trapezius muscle activity was lower for those who had an MSD; these authors concluded that the pain caused more frequent changes of postures. Further studies should investigate muscle activity looking at activity levels as well as recovery in overhead crane operators.
Preventive measures
The results of this study demonstrate that effective prevention strategies directed towards MSDs are required that address awkward work postures for overhead crane operators. Since visual field appears to be the main cause for these awkward postures, engineering controls that address visibility will be important. The use of video surveillance in the cabins with the monitor positioned at eye level has previously been recommended to promote a neutral head and back position15). If the work posture cannot be improved, administrative measures addressing work schedules and work-rest regime may be required.
Interviews conducted in the first phase of the present study revealed that the majority of operators experienced high levels of vibration inside the cabins. Thus, this risk factor should receive special attention as a contributor to the development of back pain. Based on the evidence in ergonomic literature, overhead crane operators are exposed to awkward and static postures with whole body vibration for long- term due to the nature of their tasks28,39). Prolonged sitting with awkward posture and exposure to vibration increase the risk of MSDs in the back29).
Limitations
In the present study, the back and head postures of operators were evaluated for work performed at a height of 12 m above the ground; however, cranes that are either higher or lower will have different visibility and therefore, the postures may differ40). Further study is recommended to assess the effect of different crane heights on head and back postures.
Axial rotation of the head is associated with pain disorders affecting the neck31), this is an important consideration. A second limitation was the exclusion of rotation as a movement variable; this plane of movement was excluded because of limitations inherent to the inclinometer. Given that little lateral bending occurred, it may be that operators rely on rotational movements to shift their visual field. Since neck rotation depends on the crane height, in future studies it is recommended to determine axial rotation of the head, especially for the lower height crane.
Conclusion
This is the first study to document work postures assumed during a full work shift and to compare postures between symptomatic and healthy overhead crane operators. The results showed that overhead crane operators are exposed to awkward postures in the back and head regions for long durations. Physical exposure in case group operators was characterized by more awkward and extreme postures in the back and head. This situation may explain the higher rates of symptoms in the back and neck in case operators. Our findings show that more aspects than trunk and head postures must be considered. Thus, further studies should investigate the relation between the muscle activity and posture of the trunk and neck in overhead crane operators.
Acknowledgments: This study was a part of thesis work in PhD degree and funded by Tehran University of Medical Sciences. The authors would like to thank the participants for their kind contributions.
Conflicts of interest: The authors declare that there are no conflicts of interest.
References
- 1) Nordander C, Ohlsson K, Åkesson I, et al. Risk of musculoskeletal disorders among females and males in repetitive/constrained work. Ergonomics 2009; 52: 1226-1239.
- 2) Ranney D, Wells R, Moore A. Upper limb musculoskeletal disorders in highly repetitive industries: precise anatomical physical findings. Ergonomics 1995; 38: 1408-1423.
- 3) Larsson B, Søgaard K, Rosendal L. Work related neck-shoulder pain: a review on magnitude, risk factors, biochemical characteristics, clinical picture and preventive interventions. Best Pract Res Clin Rheumatol 2007; 21: 447-463.
- 4) Van Rijn RM, Huisstede BM, Koes BW, Burdorf A. Associations between work-related factors and specific disorders of the shoulder-a systematic review of the literature. Scand J Work Environ Health 2010; 36: 189-201.
- 5) Lee H-Y, Yeh W-Y, Chen C-W, Wang J-D. Prevalence and psychosocial risk factors of upper extremity musculoskeletal pain in industries of Taiwan: a nationwide study. J Occup Health 2005; 47: 311-318.
- 6) Nawawi R, Deros BM, Daruis DDI, Ramli A, Md Zein R, editors. A pilot study on work-related neck-shoulder pain among sewing machine operators. Appl Mech Mater 2014; 471: 167-171. (Trans Tech Publ.).
- 7) Afshari D, Motamedzade M, Salehi R, Soltanian AR. Continuous assessment of back and upper arm postures by long-term inclinometry in carpet weavers. Appl Ergon 2014; 45: 278-284.
- 8) Dianat I, Karimi MA. Musculoskeletal symptoms among handicraft workers engaged in hand sewing tasks. J Occup Health 2016; 58: 644-652.
- 9) Holmström E, Engholm G. Musculoskeletal disorders in relation to age and occupation in Swedish construction workers. Am J Ind Med 2003; 44: 377-384.
- 10) Bovenzi M, Pinto I, Stacchini N. Low back pain in port machinery operators. J Sound Vib 2002; 253: 3-20.
- 11) Das B, Ghosh T. Assessment of ergonomical and occupational health related problems among VDT workers of West Bengal, India. Asian J Med Sci (pokhara) 2014; 1: 26-31.
- 12) Kushwaha DK, Kane PV. Ergonomic assessment and workstation design of shipping crane cabin in steel industry. Int J Ind Ergon 2016; 52: 29-39.
- 13) Gustafson-Söderman U. The effect of an adjustable sitting angle on the perceived discomfort from the back and neck-shoulder regions in building crane operators. Appl Ergon 1987; 18: 297-304.
- 14) Burdorf A, Zondervan H. An epidemiological study of low-back pain in crane operators. Ergonomics 1990; 33: 981-987.
- 15) Munro M. Quantification of muscular, postural, and upper limb movement demands during overhead crane operation to evaluate the potential efficacy of a camera based system 2014 (Doctoral dissertation).
- 16) Ray PK, Tewari V. Ergonomic design of crane cabins: a case study from a steel plant in India. Work 2012; 41: 5972-5976.
- 17) Takala EP, Pehkonen I, Forsman M, et al. Systematic evaluation of observational methods assessing biomechanical exposures at work. Scand J Work Environ health 2010; 36: 3-24.
- 18) Choobineh A, Lahmi M, Shahnavaz H, Khani Jazani R, Hosseini M. Musculoskeletal symptoms as related to ergonomic factors in Iranian hand-woven carpet industry and general guidelines for workstation design. Int J Occup Saf Ergon 2004; 10: 157-168.
- 19) Amasay T, Zodrow K, Kincl L, Hess J, Karduna A. Validation of tri-axial accelerometer for the calculation of elevation angles. Intl J Ind Ergon 2009; 39: 783-789.
- 20) Hansson G, Asterland P, Holmer N-G, Skerfving S. Validity and reliability of triaxial accelerometers for inclinometry in posture analysis. Med Biol Eng Comput 2001; 39: 405-413.
- 21) Brkić VS, Klarin M, Brkić AD. Ergonomic design of crane cabin interior: The path to improved safety. Saf Sci 2015; 73: 43-51.
- 22) Courtney AJ, Chan AH. Ergonomics of grab unloaders for bulk materials handling. Int J Ind Ergon 1999; 23: 61-66.
- 23) Cook C, Burgess-Limerick R, Chang S. The prevalence of neck and upper extremity musculoskeletal symptoms in computer mouse users. Int J Ind Ergon 2000; 26: 347-356.
- 24) Hayes M, Cockrell D, Smith D. A systematic review of musculoskeletal disorders among dental professionals. Int J Dent Hyg 2009; 7: 159-165.
- 25) Cho CY, Hwang YS, Cherng RJ. Musculoskeletal symptoms and associated risk factors among office workers with high workload computer use. J Manipulative Physiol Ther 2012; 35: 534-540.
- 26) Robb MJ, Mansfield NJ. Self-reported musculoskeletal problems amongst professional truck drivers. Ergonomics 2007; 50: 814-827.
- 27) Chen JC, Chang WR, Chang W, Christiani D. Occupational factors associated with low back pain in urban taxi drivers. Occupational Medicine 2005 (doi: 10.1093/occmed/kqi125).
- 28) Burdorf A, Naaktgeboren B, de Groot HC. Occupational risk factors for low back pain among sedentary workers. J Occup Env Med 1993; 35: 1213-1220.
- 29) Lis AM, Black KM, Korn H, Nordin M. Association between sitting and occupational LBP. Eur Spine J 2007; 16: 283-298.
- 30) Ariëns G, Bongers P, Douwes M, et al. Are neck flexion, neck rotation, and sitting at work risk factors for neck pain? Results of a prospective cohort study. Occup Environ Med 2001; 58: 200-207.
- 31) Baker NA, Sussman NB, Redfern MS. Discriminating between individuals with and without musculoskeletal disorders of the upper extremity by means of items related to computer keyboard use. J Occup Rehabil 2008; 18: 157-165.
- 32) Palmer KT, Smedley J. Work relatedness of chronic neck pain with physical findings-a systematic review. Scand J Work Environ Health 2007; 165-191.
- 33) Beach TA, Parkinson RJ, Stothart JP, Callaghan JP. Effects of prolonged sitting on the passive flexion stiffness of the in vivo lumbar spine. Spine J 2005; 5: 145-154.
- 34) Szeto GP, Straker LM, O'Sullivan PB. A comparison of symptomatic and asymptomatic office workers performing monotonous keyboard work-1: neck and shoulder muscle recruitment patterns. Man Ther 2005; 10: 270-280.
- 35) Aarås A, Horgen G, Bjørset HH, Ro O, Thoresen M. Musculoskeletal, visual and psychosocial stress in VDU operators before and after multidisciplinary ergonomic interventions. Appl Ergon 1998; 29: 335-354.
- 36) Karlqvist L, Tornqvist EW, Hagberg M, Hagman M, Toomingas A. Self-reported working conditions of VDU operators and associations with musculoskeletal symptoms: a cross-sectional study focussing on gender differences. Int J Ind Ergon 2002; 30: 277-294.
- 37) Jensen BR, Schibye B, Søgaard K, Simonsen EB, Sjøgaard G. Shoulder muscle load and muscle fatigue among industrial sewing-machine operators. Eur J Appl Physiol Occup Physiol 1993; 67: 46775.
- 38) Hägg GM, Åström A. Load pattern and pressure pain threshold in the upper trapezius muscle and psychosocial factors in medical secretaries with and without shoulder/neck disorders. Int Arch Occup Environ Health 1997; 69: 423-432.
- 39) Waters T, Genaidy A, Viruet HB, Makola M. The impact of operating heavy equipment vehicles on lower back disorders. Ergonomics 2008; 51: 602-636.
- 40) Krishna O, Maiti J, Ray P, Mandal S. Assessment of risk of musculoskeletal disorders among crane operators in a steel plant: A data mining-based Analysis. Hum Factors Ergon Manuf 2015; 25: 559-572.
