Brief Reports
Underreporting trends of occupational illnesses in Mexico

2018 Volume 60 Issue 1 Pages 85-88

Details
2018 Volume 60 Issue 1 Pages 85-88
Objective: To report trends underreporting levels of occupational illnesses (OI) in Mexico from 2000 to 2015. Methods: An ecological study was conducted. Data on OI was obtained from the Statistical Memories of the Mexican Institute of Social Security. We used univariate sensitivity analysis to estimate the average value and range. Results: During the 2000-2015 period, the estimated average OI underreporting in the Mexican population was 89.1%; the minimum was 81.8% in 2015 and the maximum 95% in 2007, with an annual decrement rate of 1% (p<0.05) was observed from 2007 to 2015. Conclusions: Important changes to improve reporting of OI have taken place since 2007, most likely due to the implementation of new policies in this matter. Even though the OI report in Mexico is higher than what the World Health Organization estimates for Latin America (18% in 2015), activities to address this problem remain insufficient. Furthermore, it is important to evaluate the current process of identification and registration of OI in order to identify those that need reinforcement, to guarantee adherence to regulations, to consolidate training systems, and importantly, to develop the governing capacity of the sanitation and labor authorities to exercise their coordinating and regulatory functions.
Occupational illnesses (OI) cause loses to workers, companies, health institutions, and the population at large1). They seem to be increasing due to the fast industrialization of some developing countries, causing six times more fatalities than those reported as occupational accidents2). According to estimates of the International Labor Organization (ILO), 160 million new cases of OI occur in the world2). Whereas, the Americas only report annually over 281,000 cases3). Mexico reported a little more than 12,000 new cases in 20154), a very small number considering the magnitude of the labor force in this country. ILO estimates OI incidence to be in the range of 2.5 and 5.4 per 1,000 exposed workers5).
OI reports foster research related to workers' health as well as identifies causal factors, as to identify problems, defining objectives and strategies in order to direct resources to improve workplace conditions and work environment, aiming to protect the health of workers1).
Nevertheless, underreporting the real burden of OI is a very important chronic problem in the grounds of occupational safety6-8). Developed countries traditionally show between 9% to 79% of underreporting; these percentages are larger in developing countries7-10). The World Health Organization (WHO) estimates that in Latin America only 1% to 4% of all OI are reported9). From 1994 to 2004, Mexico solely reported an underreporting prevalence of occupational injury from 26.3% to 77.9%11).
The national information on OI is scarce and unreliable due mainly to limitations in diagnosing occupational illness and to inefficient report systems. Furthermore, the Mexican Institute of Social Security (Instituto Mexicano del Seguro Social, IMSS) is the only Mexican health provider reporting OI, and it provides health services to only 40% of the employed population9,11). IMSS information is presented as a statistical report4) and it is published annually. In this context, the aim of this study was to analyze and examine the magnitude of underreporting OI and its trends in Mexico from 2000 to 2015.
An ecological study was conducted to compare trends in the percentage of OI underreporting in Mexico from 2000 to 2015. Data on OI was obtained from the Statistical Memories of the IMSS and is available on its website4). For comparison purpose, the total number of OI observed was compared with estimates of OI expected considering the employed population for each federal state per each study year. For estimates the OI incidence, we used to report by the ILO5).
The following equation provides the calculation of underreporting percentage:
allowing a nationwide projection. Univariate sensitivity analysis by @Risk7.5 was used with 10,000 interactions to estimate an average value and a range that would include 95% of the interactions. The annual percentage change was used to assess trends, and statistical significance was estimated using joinpoint models.
At the national level, the estimated incidence of OI showed a slight growing trend along the analyzed period of 2000-2015, with an annual growth rate of 2.3% (p<0.05). Nevertheless, the observed incidence was irregular, with a mean annual decrement of 4% (p=0.6) for the 2000-2007 period; conversely, after 2007, the trend varied considerably and it increased, with an annual growth rate of 13% (p<0.05).
The percentage of the estimated mean of OI underreporting was 89.1% over the 2000-2015 period nationally; the lowest percentage of OI underreporting (81.8%) was observed during 2015 and the highest (95%) in 2007. An irregular of OI underreporting trend was observed before 2007, with an annual growth percentage of 0.5% (p=0.6); after 2007, the OI underreporting decreased, with an annual decrement rate of 1% (p<0.05) from 2007 to 2015 (Fig. 1).
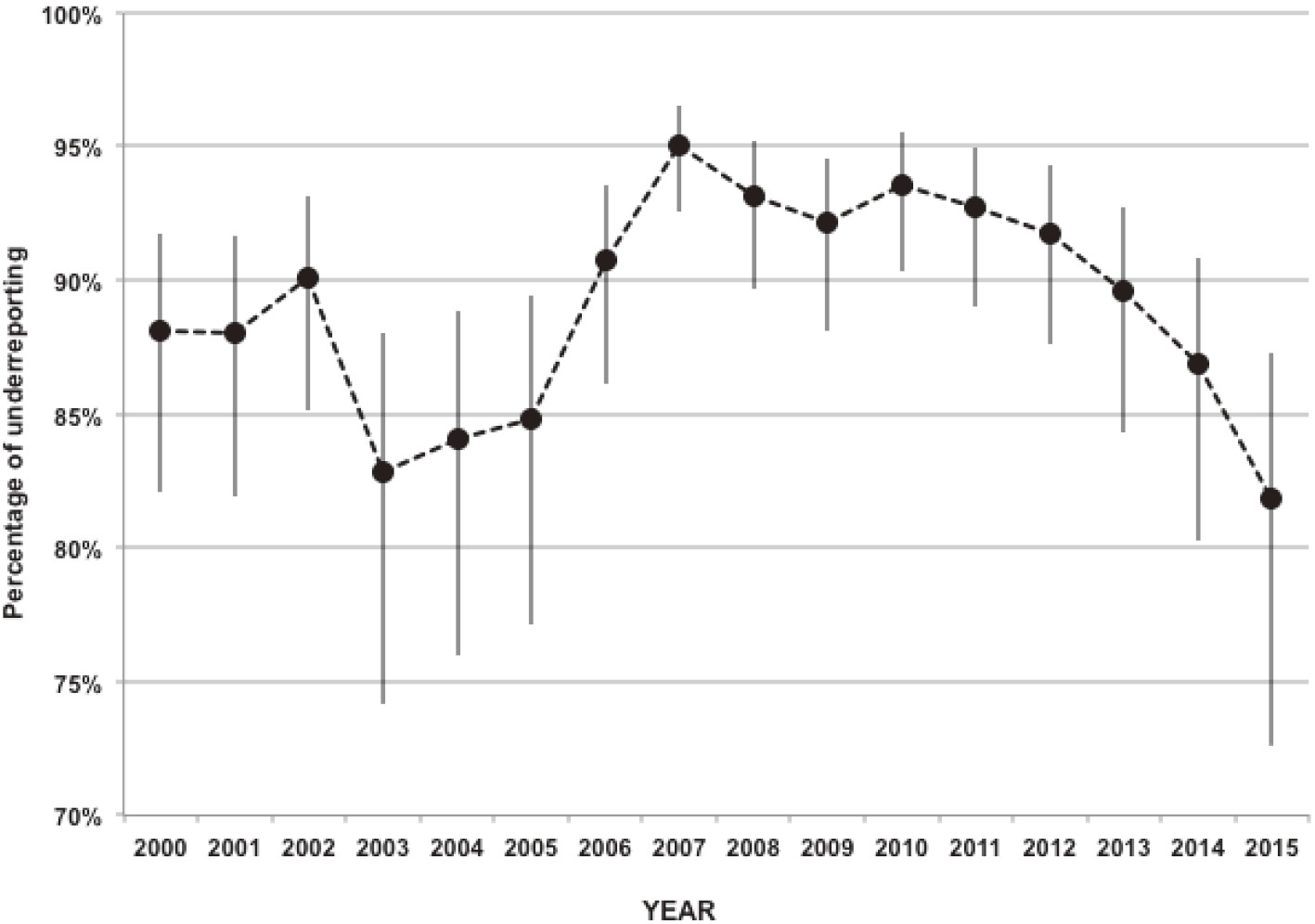
Underreporting of occupational illnesses in Mexico, 2000-2015.
Nationally, the trend of OI underreporting was irregular for the 2000-2015 period. However, the irregular trends observed during 2000-2007 can be attributed to the political change in Mexico's government, and a financial and political crisis of IMSS occurring during that period and their employees worked under protest. In December 2006, it had a new change in Mexico's presidential succession, and IMSS director, other important changes took place such as, digitalization of medical services and electronic record keeping along with changes in the institutional registry formats for occupational injuries and OI. Coincidentally, personnel trained in the area of occupational medicine were hired, thus improving the capabilities to identify and search for OI and their risk factors.
In addition, occupational health providers are strongly urged to expedite screening and early diagnosing on those workers at risk, by means of goal setting and yearly efficiency performance reviews. Additionally, ILO's updated listings of OI must be incorporated in the daily practice of medical personnel in order to improve reporting.
2015 showed the smallest percentage of OI underreporting since 2007 due to improved screening, diagnosing, and reporting of OI, reflecting recent efforts in OI registry recovery. Inasmuch as OI reports in Mexico are above the WHO estimations for Latin American countries (18.2% in 2015)9), and very similar to Spain's (17%)12), further actions are still necessary to correct OI underreporting in Mexico. Several characteristics attributable to the worker have been identified as contributing factors to OI underreporting, such as: the feeling of being healthy, improved earnings, apprehension to intimidation or harassment, employment in a non-manufacturing sector, small business employment, non-union employment, on temporary sick leave, considering pain as normal consequence of work or aging, lack of understanding about OI reporting systems, administrative obstacles7,8,10), health provider failure to detect or identify an OI, and long latency periods of some illnesses13).
It is also important to assess the strategy efficacy given that most medical personnel receive little training in OI recognition. Menzel and cols13), Haro-García and cols11) suggest a number of ways to incentivize OI reporting. They recommend certification and surveillance of OI mainly in special populations such as temporary workers and in those hired by contingency. Besides improving and updating administrative formats and recordkeeping methods in health settings, employers, and labor unions14), also by providing continuing education to health personnel on adequate recognition and registry of OI through continue health education programs on topics related to risk factors and OI14).
Likewise, political difficulties are found to be associated with a deficient estimation of OI given that Mexico has the IMSS as the single source of information for this task. In addition, their reports are incomplete, despite having legislation and regulation designed to signal the responsibility of employers to report OI. Officials responsible for surveillance and reinforcement of compliance need to improve reporting.
In conclusion, our findings suggest that the tendencies of OI underreporting have experienced a significant positive change since 2007; this improvement could be the outcome of changes made through the implementation of new policies in this matter. The reporting of OI is an important challenge in developed countries. Our study is the first in Mexico aimed to assess OI underreporting. It is intended to open a path to explore the magnitude of the problem and guide future studies designed to evaluate current procedures in order to identify areas in need of reinforcement. To assure the implementation of regulations and consolidate training systems, but most importantly, to develop the directing capacities of the sanitary and labor authorities in order to comply with their role in coordination and regulation, with the ultimate goal to improve the reporting of OI at the national level.
Conflicts of interest: The authors declare that there are no conflicts of interest.