抄録
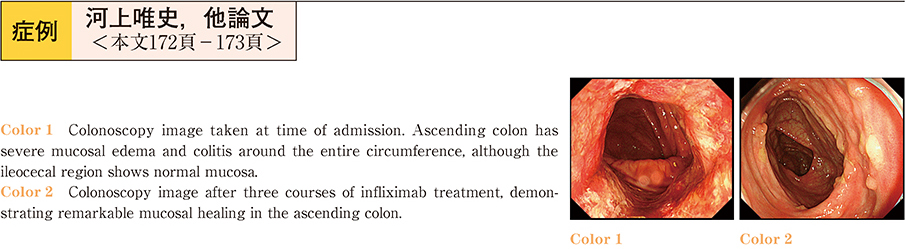
A 29-year-old woman was first diagnosed with ulcerative colitis (proctitis) six months previously. Remission was successfully induced with mesalazine, but treatment was interrupted. In spite of repeated treatment with mesalazine, symptoms exacerbated and the patient presented at our hospital. Laboratory analysis revealed leukocytosis and elevated serum CRP level. Enteropathogenic Escherichia coli and CMV antigenemia assays were negative. Colonoscopy revealed severe mucosal edema, colitis involving the entire circumference, and ulcerative lesions with a punched out appearance in the ascending colon. Examination of the transverse colon through to the sigmoid colon showed almost normal mucosa, and the rectum showed granularity of the mucosa─typical of ulcerative colitis (UC) . Differential diagnoses such as Crohn’s disease or drug-induced colitis were possible, but it was difficult to make a definitive diagnosis. The patient was admitted to our hospital, and prednisolone therapy was initiated at a dose of 60 mg/day, according to the treatment regime for severe UC. Endoscopic findings showed improvements in the mucosal edema. Conversely, pseudopolyposis of the intestinal wall was seen. On the 32nd day, the patient suddenly developed severe melena and shock. Although surgery was advised, the patient declined. Infliximab was started at a dose of 5 mg/kg, and symptoms rapidly improved. Endoscopic findings after three courses of treatment showed remarkable mucosal healing.