抄録
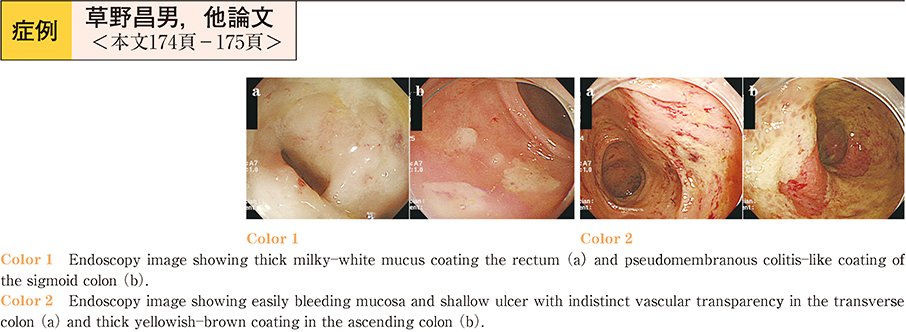
The patient was a 75-year-old woman receiving several medications─aspirin, amlodipine, candesartan, furosemide, spironolactone, rosuvastatin and triazolam─for cerebral infarction, hyperlipidemia, hypertension and sleeplessness. Furthermore the woman was being medicated with lansoprazole for reflux esophagitis. She developed watery diarrhea after taking lansoprazole for approximately four months. The woman presented at our hospital after suffering watery diarrhea for five months. Colonoscopic examination showed thick mucus coating the rectum and a pseudomembranous coating in the sigmoid colon. Colonic mucosal biopsy showed marked inflammatory cells, and a diagnosis of erosive colitis and proctitis was made. However, the diarrhea continued and a second colonoscopy was performed. This showed easily blee-ding mucosa and a shallow ulcer with indistinct vascular transparency in the transverse colon and thick yellowish-brown coating in the ascending colon. A colonic mucosal biopsy showed a thick collagen band in the subepithelial region, and collagenous colitis was diagnosed. The patient’s watery diarrhea was relieved one week after changing lansoprazole to omeprazole. Colonoscopic and pathological findings one year later showed visibly normal mucosa. In this case colonoscopic findings were atypical for collagenous colitis.