-
A Meta-Analysis
Fei Li, Shengda Hu, Xianyong Zhou, Xiaofei Mei, Yafeng Zhou
2020 Volume 61 Issue 4 Pages
641-650
Published: July 30, 2020
Released on J-STAGE: July 30, 2020
Advance online publication: July 18, 2020
JOURNAL
FREE ACCESS
A number of studies have showed the relationship between R353Q (rs6046) polymorphism in factor VII gene and coronary heart disease (CHD). However, the results remain controversial due to the limitations of the research objects and small sample size of individual study. We conducted this meta-analysis to validate the association between R353Q (rs6046) polymorphism and the risk of CHD.
The relevant data was collected up to March 25, 2019 from PubMed, Web of Science, CNKI, and Wanfang databases. We examined all eligible studies using the Newcastle-Ottawa Quality Assessment Scale (NOS). The odds ratio (OR) and its corresponding 95% confidence interval (CI) were adopted to evaluate the relationship between the R353Q (rs6046) polymorphism and CHD. Stata version 14.0 (Stata Corporation, USA) was used in all statistical tests.
There were at least 28 eligible studies, including 14626 cases and 17994 controls, included in our meta-analysis. R353Q (rs6046) polymorphism was associated with the reduced risk of CHD in four genetic models: allele model (Q versus R: OR = 0.79, 95% CI: 0.69 to 0.90, P < 0.001, I2 = 56.4%), homozygote (co-dominant) model (QQ versus RR: OR = 0.72, 95% CI = 0.58 to 0.92, P = 0.004, I2 = 5.8%), heterozygote (co-dominant) model (RQ versus RR: OR = 0.71, 95% CI = 0.58 to 0.86, P = 0.001, I2 = 75.4%), and dominant model (RQ+QQ versus RR: OR = 0.74, 95% CI = 0.63 to 0.865, P < 0.001, I2 = 64.1%) excluding recessive model (QQ versus RR+RQ: OR = 0.86, 95% CI = 0.57 to 1.28, P = 0.447, I2 = 51.6%).
The results of the current meta-analysis suggested that R353Q (rs6046) polymorphism was associated with the reduced risk of CHD, especially in Asians.
View full abstract
-
Wei Gong, Han Shi, Mengwen Yan, Yan Yan, Xiao Wang, Siyi Li, Xiaonan H ...
2020 Volume 61 Issue 4 Pages
651-657
Published: July 30, 2020
Released on J-STAGE: July 30, 2020
Advance online publication: July 18, 2020
JOURNAL
FREE ACCESS
Ventricular free wall rupture (FWR) is a catastrophic complication of that occurs after acute myocardial infarction (AMI), and at present, its clinical characteristics are unclear. We analyzed a total of 6,712 consecutive patients who presented with ST-segment elevation myocardial infarction (STEMI), and 78 patients with FWR after STEMI were enrolled in the study. Patients' demographic data, clinical manifestation, laboratory test results, and angiographic features were then collected and analyzed. FWR occurred in 78 cases (1.16%), and the inhospital mortality of FWR was up to 92.3%. Among the 78 FWR patients, 72 obtained accurate rupture time. FWR typically occurred within the first week after the infarct. Compared to late-phase FWR (more than 48 hours after STEMI) patients, early-phase FWR (during 48 hours after STEMI) patients showed significantly higher random glucose and higher percentage of anterior myocardial infarction. Besides, dual antiplatelet therapy (DAPT), β-blockers, and angiotensin-converting enzyme inhibitors/angiotensin receptor blocker (ACEI/ARB) were used less frequently in early-phase FWR patients. Moreover, we first reported the precipitating factors of FWR. Defecating, transporting, acute emotional upset, diets, and invasive treatment turned out to be the main triggers for FWR. Furthermore, we found that patients who survived from FWR were younger, had higher β-blocker coverage in the inhospital treatment, and had a higher frequency of primary PCI. FWR remains an infrequent but devastating complication of STEMI. We have found several factors related to the occurrence and prognosis of FWR. This study provides evidence for a better understanding of FWR.
View full abstract
-
Wen Su, Man Wang, Jiegao Zhu, Weiping Li, Xiaosong Ding, Hui Chen, Hon ...
2020 Volume 61 Issue 4 Pages
658-664
Published: July 30, 2020
Released on J-STAGE: July 30, 2020
Advance online publication: July 08, 2020
JOURNAL
FREE ACCESS
Increased body mass index (BMI) is a well-established risk factor for cardiovascular disease; however, patients with elevated BMI, in comparison to those with low BMI, seem to have better survival, a phenomenon reported as "obesity paradox," which remains controversial. We investigated the effect of BMI on cardiac mortality post acute myocardial infarction (AMI).
In this analysis, 3562 AMI patients were included and classified into four groups based on BMI values. The primary endpoint was cardiac death. Compared to normoweight group, overweight and obese group subjects were younger, mostly men, and more likely to receive percutaneous coronary intervention (PCI) and had higher levels of glucose and lipids, but lower level of NTproBNP. Subjects in the underweight group were older, were mostly women, had lower Barthel index (BI), were less likely to receive PCI, and had lower levels of glucose and lipids, but higher level of N-terminal pro-brain natriuretic peptide (NTproBNP) and higher rates of left ventricular ejection fraction (LVEF) < 50%. During a median follow-up period of 1.9 years, cardiac death occurred significantly more in the underweight group (30.0%, 10.6%, 7.0%, and 5.0% among the four groups from underweight to obese; P < 0.001 for trend). The Cox analysis revealed that underweight was an independent predictor of subsequent cardiac death (odds ratio (OR), 1.86; 95% confidence interval (CI), 1.07-3.25) and identified that older age, BI < 60, higher levels of cardiac troponin I (cTnI), LVEF < 50%, and not receiving PCI were independently associated with increased risk of cardiac death.
Patients who were underweight were at greater risk of cardiac death post AMI. In addition, older age, frail, higher levels of cTnI, LVEF < 50%, and not receiving PCI also independently predicted cardiac mortality post AMI.
View full abstract
-
Serial OCT Analysis
Yuji Matsuda, Takashi Ashikaga, Taro Sasaoka, Yu Hatano, Tomoyuki Umem ...
2020 Volume 61 Issue 4 Pages
665-672
Published: July 30, 2020
Released on J-STAGE: July 30, 2020
Advance online publication: July 18, 2020
JOURNAL
FREE ACCESS
Supplementary material
Clinical outcomes after percutaneous coronary intervention (PCI) for severely calcified lesions remain poor. The purpose of this study was to investigate the neointimal response after everolimus-eluting stents (EES) for severely calcified lesions treated with rotational atherectomy (RA) using optical coherence tomography (OCT).
We retrospectively analyzed 34 lesions in which PCI was performed with EES deployment following RA and OCT was performed immediately after PCI and at follow-up (nine months). The EES was either durable-polymer (DP) EES (22 lesions) or bioabsorbable polymer (BP) -EES (12 lesions). Strut coverage and malapposition were evaluated at 1-mm intervals of cross-section (CS) by serial OCT analysis. Malapposed strut was defined as having the distance from luminal border > 100 μm.
A total of 11,823 struts immediately after PCI and 11,720 struts at follow-up were analyzed. Immediately after PCI, the strut-level analysis showed no significant differences in the percentage of malapposed struts between the DP-EES group and the BP-EES group. At follow-up, the BP-EES group showed a more prevalent covered strut compared with the DP-EES group (strut-level analysis: 95% versus 97%, P = 0.045; CS-level analysis: 97% versus 100%, P < 0.01; lesion-level analysis: 27% versus 83%, P < 0.01, respectively).
In severely calcified lesions requiring RA, the BP-EES group achieved better neointimal coverage than the DP-EES group at nine months. Additional prospective studies are needed.
View full abstract
-
Yong Hoon Kim, Ae-Young Her, Myung Ho Jeong, Byeong-Keuk Kim, Sung-Jin ...
2020 Volume 61 Issue 4 Pages
673-684
Published: July 30, 2020
Released on J-STAGE: July 30, 2020
Advance online publication: July 18, 2020
JOURNAL
FREE ACCESS
Supplementary material
Hyperglycemia is an important risk factor for poor clinical outcomes in patients with acute myocardial infarction (AMI). The relative superiority of the long-term clinical outcomes of durable-polymer (DP) -based and biodegradable-polymer (BP) -based newer-generation drug-eluting stents (DESs) after successful percutaneous coronary intervention (PCI) in patients with AMI and prediabetes is not well established. We compared the clinical outcomes in such patients between DP-based and BP-based newer-generation DESs.
A total of 4,377 patients with AMI and prediabetes were divided into the following two groups: the DP-DES group (n = 3,775; zotarolimus-eluting stents [ZES; n = 1,546] and everolimus-eluting stents [EES; n = 2,229]) and the BP-DES group (n = 602; biolimus-eluting stents [BES]). The primary endpoint was the occurrence of major adverse cardiac events (MACEs), defined as all-cause death, recurrent myocardial infarction (re-MI), or any repeat revascularization. The secondary endpoint was the occurrence of stent thrombosis (ST).
The 2-year adjusted hazard ratio (aHR) of MACEs for ZES versus EES, ZES versus BES, EES versus BES, and ZES/EES versus BES (aHR: 1.125; 95% confidence interval [CI], 0.834-1.518; P = 0.440) were similar. The cumulative incidence of ST was also comparable between the DP-DES and BP-DES groups (aHR: 1.407; 95% CI, 0.476-4.158; P = 0.537). Moreover, the 2-year aHRs of all-cause death, CD, re-MI, target lesion revascularization (TLR), target vessel revascularization (TVR), and non-TVR were similar.
Patients with AMI and prediabetes who received DP-DES or BP-DES during PCI showed comparable safety and efficacy during the 2-year follow-up period.
View full abstract
-
Takumi Hatta, Shunichi Yoda, Misa Hayase, Koyuru Monno, Yusuke Hori, H ...
2020 Volume 61 Issue 4 Pages
685-694
Published: July 30, 2020
Released on J-STAGE: July 30, 2020
Advance online publication: July 18, 2020
JOURNAL
FREE ACCESS
Left ventricular (LV) mechanical dyssynchrony assessed with phase analysis of electrocardiogram (ECG) -gated single photon emission computed tomography (SPECT) myocardial perfusion imaging (MPI) is useful for predicting major cardiac events (MCEs) in patients with cardiac dysfunction. However, there is no report on its usefulness in Japanese patients with known or suspected stable coronary artery disease (CAD) with preserved LV ejection fraction (LVEF).
We retrospectively investigated 3,374 consecutive patients with known or suspected CAD who underwent rest 201Tl and stress 99mTc-tetrofosmin ECG-gated SPECT MPI and had preserved LVEF (≥ 45%), and followed them up to confirm their prognosis for three years. The composite endpoint was the onset of MCEs consisting of cardiac death, non-fatal myocardial infarction (MI), unstable angina pectoris, and severe heart failure requiring hospitalization. LV mechanical dyssynchrony was evaluated with phase analysis with the Heart Risk View-F software to obtain the phase bandwidth and standard deviation.
During the follow-up, 179 patients experienced MCEs: cardiac death (n = 42); non-fatal MI (n = 34); unstable angina pectoris (n = 54); and severe heart failure (n = 49). Results of the multivariate analysis showed age, a history of MI, diabetes mellitus, summed stress score, and stress phase bandwidth to be independent predictors for MCEs. In Kaplan-Meier analysis, prognoses were significantly stratified with the tertiles of stress phase bandwidth.
LV mechanical dyssynchrony assessed with ECG-gated SPECT MPI is useful for predicting a prognosis and stratifying the risk of MCEs in Japanese patients with known or suspected stable CAD with preserved LVEF.
View full abstract
-
Naomi Hirota, Shinya Suzuki, Masao Yamasaki, Naoki Matsumoto, Kousuke ...
2020 Volume 61 Issue 4 Pages
695-704
Published: July 30, 2020
Released on J-STAGE: July 30, 2020
Advance online publication: July 18, 2020
JOURNAL
FREE ACCESS
The "on-therapy range" of direct oral anticoagulants is the 90% interval of drug concentration. Previously, we reported the on-therapy range of rivaroxaban in a single-center cohort. The present study aimed to confirm the range and intraindividual reproducibility in a multicenter cohort.
Eligible patients with non-valvular atrial fibrillation under rivaroxaban treatment for prevention of ischemic stroke were enrolled from nine institutes in Tokyo, Japan, between June 2016 and May 2017 (n = 324). The first and second (three months later) blood samples both taken within 1-5 hours after rivaroxaban intake were analyzed (n = 219). Plasma concentration of rivaroxaban (PC-Riv) and prothrombin time (PT) with five reagents were measured.
The 90% interval of PC-Riv was 47.3-532.9 ng/mL. The 90% interval of PT measured with RecombiPlasTin 2G was 11.8-22.3 seconds, the widest range among the five reagents examined. PC-Riv reproducibility within a 90% interval was evaluated bidirectionally (first-to-second and second-to-first), and 92.4% of samples were reproducible. The change rate (CR) of PC-Riv between two samplings ranged widely, and high CR (≥54.3%, cutoff for predicting non-reproducibility) was predicted by concomitant drugs (non-dihydropyridine calcium antagonist and thiazide) and mitral regurgitation.
We reported the on-therapy range of rivaroxaban in a multicenter cohort. This range was consistent with that of a single-center cohort and was highly reproducible within three months in daily clinical practice. However, caution is necessary regarding several factors that may affect the intraindividual variation of PC-Riv.
View full abstract
-
Hao Rong, Lei Huang, Nake Jin, Jun Hong, Jianan Hu, Shanshan Wang, Yuq ...
2020 Volume 61 Issue 4 Pages
705-712
Published: July 30, 2020
Released on J-STAGE: July 30, 2020
JOURNAL
FREE ACCESS
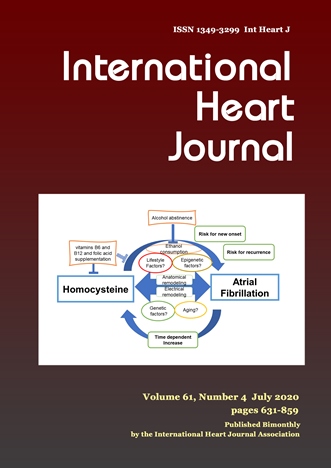
There is increasing evidence linking plasma homocysteine levels and atrial fibrillation (AF). The association between an elevated level of plasma homocysteine and AF was examined by meta-analysis in this study.
The PubMed and ScienceDirect databases until August 2019 were utilized to collect previous literature on homocysteine and the potential relation to AF. The pooled effects were evaluated depending on standardized mean differences (SMDs) or odds ratios (ORs) with 95% confidence intervals (CIs), and the calculation was performed using Stata 12 software.
A total of 11 validated articles were included in the meta-analysis. For pooled effect, the results confirmed that AF patients had higher homocysteine levels than control subjects (SMD: 0.58, 95%CI: 0.09-1.06). Compared with control subjects, homocysteine levels were higher in paroxysmal AF (SMD: 0.45, 95%CI: 0.18-0.72) and persistent AF patients (SMD: 1.21, 95%CI: 0.50-1.92). The pooled analysis suggested that patients with elevated homocysteine levels had markedly higher risk of AF compared with lower homocysteine levels in the categorical variable (OR: 2.21, 95%CI: 1.16-4.21) and continuous variable analyses (OR: 1.13, 95%CI: 1.00-1.27), respectively. In addition, the pooled analysis indicated that recurrent AF patients had significantly higher homocysteine levels than those without recurrence (SMD: 0.65, 95%CI: 0.42-0.88). The pooled analysis of the categorical variables indicated that elevated homocysteine levels were associated with increased risk of AF recurrence (OR: 3.81, 95%CI: 3.11-4.68). However, the association was weak in the pooled analysis of continuous variables (OR: 1.88, 95%CI: 0.74-4.81).
Our meta-analysis identified that plasma homocysteine levels were significantly elevated in AF and recurrent AF patients. Elevated homocysteine is associated with increased risk of AF and AF recurrence.
View full abstract
-
Franz-Josef Neumann, Simon Redwood, Mohamed Abdel-Wahab, Thierry Lefèv ...
2020 Volume 61 Issue 4 Pages
713-719
Published: July 30, 2020
Released on J-STAGE: July 30, 2020
Advance online publication: July 18, 2020
JOURNAL
FREE ACCESS
Differences in the benefits of conscious sedation (CS) and general anesthesia (GA) during transfemoral aortic valve implantation (TAVI) are unclear.
We aimed to assess differences in procedural and clinical outcomes based on the type of anesthesia received during TAVI.
We analyzed SOURCE 3 Registry data for patients who received the SAPIEN 3 valve by type of anesthesia used during TAVI.
Of the 1694 TAVI patients, 1027 received CS and 667 received GA. Patients were similar at baseline (81.5 years; Society of Thoracic Surgeons risk score 7.0). Compared with the GA group, the CS group had fewer intra-procedural transesophageal echocardiography (TEE) and post implantation dilatations performed, and less contrast medium was used. The CS group had significantly less kidney injury at 7 days post-procedure than the GA group (0.4% versus 1.5%, P = 0.014). Moderate paravalvular leaks (PVL) occurred more frequently in the CS group versus the GA group (2.2% versus 0.8%; P = 0.041). No severe PVL were reported. Median total hospital length of stay (LOS) after TAVI was 10 days in the CS group and 11 days in the GS group. At 30 days, all-cause death was 2.1% in CS and 1.7% in GS (P = 0.47), and myocardial infarction was 0.2% in CS and 0.1% in GS (P = 0.83).
Our analyses found no significant major outcome differences between CS and GA during TAVI.
View full abstract
-
Motoko Ueda, Toru Kubo, Yuri Ochi, Asa Takahashi, Kazuya Miyagawa, Yui ...
2020 Volume 61 Issue 4 Pages
720-726
Published: July 30, 2020
Released on J-STAGE: July 30, 2020
Advance online publication: July 18, 2020
JOURNAL
FREE ACCESS
Hemodialysis (HD) is one of the important risks for the development of cardiovascular disease, including aortic valve stenosis (AS). Although aortic valve replacement (AVR) is a beneficial treatment for AS, HD patients are known to show a high rate of mortality after AVR than non-HD patients.
We retrospectively studied 109 patients who underwent AVR for severe AS, 18 of which were HD patients. Survival rate after AVR, preoperative clinical data, and surgical procedure were investigated.
In preoperative clinical features, left ventricular end-diastolic diameter was larger, intraventricular septum thickness (IVST) was thicker, left ventricular mass index (LVMI) was higher, left ventricular ejection fraction was lower, E/e' was higher, and pulmonary arterial wedge pressure (PAWP) was higher in the HD group than in the non-HD group. During a follow-up period of 3.2 ± 2.3 years after AVR, patients receiving HD had a worse prognosis than those without HD treatment: the 3-year survival rate after surgery in the HD group was 36.2% and that in the non-HD group was 84.9%. With regard to prognostic factors in the whole cohort, significant differences were found in IVST, LVMI, E/e', PAWP, and HD. In patients receiving HD, abnormally high PAWP for their right atrial pressure (RAP) was observed, suggesting that PAWP and RAP were discordant, and univariate analysis revealed that high PAWP was the only predictor of mortality in HD patients after surgery.
Preoperative PAWP with a discordant pattern in HD patients might be an important prognostic predictor after AVR.
View full abstract
-
Hiroaki Nakaya, Naoyuki Yokoyama, Yusuke Watanabe, Akihisa Kataoka, Ku ...
2020 Volume 61 Issue 4 Pages
727-733
Published: July 30, 2020
Released on J-STAGE: July 30, 2020
Advance online publication: July 18, 2020
JOURNAL
FREE ACCESS
Despite witnessing an upsurge in heart valve diseases (HVDs), the correlation between HVDs and atherosclerotic peripheral arterial obstructive disease (PAOD) remains unclear. This study aims to investigate the prevalence and predictors of PAOD in HVDs.
In this study, a total of 245 consecutive patients were examined: 153 with severe aortic valve stenosis (AS), 66 with severe primary mitral valve regurgitation (MR), and 26 with severe pure native aortic valve regurgitation (AR). All patients underwent ultrasound scan of the carotid artery to ascertain the presence of internal carotid artery stenosis (ICAS). ICAS was defined as a peak systolic velocity ≥ 125 cm/second and/or ≥ 50% reduction in diameter. In addition, we measured the ankle-brachial index in each leg using a volume plethysmograph. A result of ≤ 0.9 was considered lower extremity artery disease (LEAD).
The presence of ICAS was statistically more frequent in patients with severe AS than in patients with severe MR and AR (11.1% versus 1.5% versus 3.8%; P = 0.038). LEAD was present in patients with severe AS (17.6%) and MR (10.6%) but not in patients with severe AR (P = 0.037). The multivariate analysis revealed that the presence of severe AS (OR, 5.6 [1.3-24.9]; P = 0.023) was an independent predictor for ICAS, while history of coronary artery disease (OR, 4.8 [2.2-10.5]; P < 0.001) was an independent predictor for LEAD.
The prevalence of PAOD varies depending on each valvular disease. Individual screening should be considered on the basis of atherosclerotic risk factors, especially for patients with severe AS.
View full abstract
-
Mitsuo Sobajima, Teruhiko Imamura, Hiroshi Onoda, Hiroyuki Kuwahara, S ...
2020 Volume 61 Issue 4 Pages
734-738
Published: July 30, 2020
Released on J-STAGE: July 30, 2020
Advance online publication: July 18, 2020
JOURNAL
FREE ACCESS
Peri-procedural elevated B-type natriuretic peptide (BNP) is also associated with worse outcomes following transcatheter aortic valve implantation (TAVI). However, the mechanism of BNP regulation in patients with severe aortic stenosis (AS) remains unknown. Consecutive patients with severe AS who were referred for TAVI were enrolled in our prospective registry. BNP levels were correlated with other clinical variables. Ninety-six patients (84.7 ± 5.0 years old, 34% males) were investigated in this study. Plasma BNP averaged 353 ± 179 pg/mL. Log10 BNP had no significant correlation with severity of AS including aortic valve area and maximum flow velocity across the aortic valve (P > 0.05 for all), whereas a higher left ventricular end-diastolic dimension (LVDd) index was a significant factor associating with BNP >100 pg/mL with an odds ratio of 1.34 (95% confidence interval 1.06-1.52, P = 0.004) adjusted for several other echocardiographic parameters, with a cutoff of 30.8 mm/m2 (equivalent to LVDd 44 mm). In conclusion, among the patients with severe AS who undergo TAVI, even slight eccentric hypertrophy can cause a considerable increase in BNP level.
View full abstract
-
Yuki Kimura, Takahiro Okumura, Shingo Kazama, Naoki Shibata, Hideo Ois ...
2020 Volume 61 Issue 4 Pages
739-747
Published: July 30, 2020
Released on J-STAGE: July 30, 2020
Advance online publication: July 18, 2020
JOURNAL
FREE ACCESS
The metabolism of branched-chain amino acids (BCAAs) is reported to change in heart failure (HF) and correlate with cardiac function. However, the effect of BCAAs on HF remains controversial. We investigate the prognostic value of the plasma BCAA level in nonischemic dilated cardiomyopathy (NIDCM).
This study enrolled 39 NIDCM patients, who underwent plasma amino acid (AA) analysis. The ratio of BCAAs to total AAs was calculated. All patients were divided into two groups at the median of BCAA/total AA ratio; high BCAA/total AA group (≥ 0.15, n = 20) and low BCAA/total AA group (< 0.15, n = 19). A cardiac event was defined as a composite of cardiac death, hospitalization for worsening HF, and lethal arrhythmia.
The mean age was 51.1 ± 12.3 years and left ventricular ejection fraction (LVEF) was 32.7 ± 10.1%. In the low BCAA/total AA group, the body mass index and the total cholesterol level were lower than in the high BCAA/total AA group. The BCAA/total AA ratio was positively correlated with LVEF (r = 0.35, P = 0.031) and negatively correlated with brain natriuretic peptide (r = −0.37, P = 0.020). The low BCAA/total AA group had a lower cardiac event-free rate (5-year: 100% versus 73%; P = 0.019). In univariate analysis, angiotensin converting enzyme inhibitor or angiotensin II receptor blocker (hazard ratio: 0.045, P = 0.0014), hemoglobin (hazard ratio: 0.49 per 1 g/dL, P = 0.0022), and BCAA/total AA ratio < 0.15 (hazard ratio: not available, P = 0.0066) were major predictors for cardiac events.
The BCAA/total AA ratio might be a useful predictor for future cardiac events in patients with NIDCM.
View full abstract
-
Takuto Arita, Shinya Suzuki, Yuko Kato, Hiroto Kano, Junji Yajima, Shu ...
2020 Volume 61 Issue 4 Pages
748-754
Published: July 30, 2020
Released on J-STAGE: July 30, 2020
Advance online publication: July 18, 2020
JOURNAL
FREE ACCESS
Although bisoprolol is used widely to treat patients with heart failure (HF), little information is available regarding the association between the dose of bisoprolol administered and the bisoprolol plasma concentration (Bis-PC) in real-world clinical practice.
This was a single-center, observational study in 114 patients with HF receiving once-daily bisoprolol. After determination of trough Bis-PC, the relationship between the dose of bisoprolol and Bis-PC was analyzed. In a multiple linear regression model, the dose of bisoprolol and estimated creatinine clearance (reciprocal number) were identified as independent predictors. HF severity and hepatic function were not associated with Bis-PC.
Bis-PC was increased by renal dysfunction, which explained most of the discrepancy between the dose of bisoprolol administered and Bis-PC.
View full abstract
-
Shu-Ting Huang, Kai-Peng Sun, Ning Xu, Qiang Chen, Hua Cao
2020 Volume 61 Issue 4 Pages
755-760
Published: July 30, 2020
Released on J-STAGE: July 30, 2020
Advance online publication: July 18, 2020
JOURNAL
FREE ACCESS
To assess changes in the quality of life in adult patients undergoing percutaneous device closure of atrial septal defect (ASD).
We used a standard Medical Outcome Study Short Form 36 (SF-36) that includes psychological and physiological aspects to assess and analyze the quality of life of 73 adult patients who underwent percutaneous device closure of ASD.
Of the 73 patients who were investigated in this study, 67 completed questionnaires successfully. The following findings were revealed after analyzing the preoperative results and postoperative results. In some dimensions ( "physical functioning," "vitality," "general health" ), the postoperative perception was better than the preoperative status. Some differences were found in the quality of life feedback between the case group and the control group. Among the different subgroups, older patients scored lower than younger patients on most dimensions, and men seemed to perform better on "role-physical" factors than women. Unmarried people performed worse on "role-physical" and "bodily pain" than married people. Among people with different academic degrees, those with higher degrees demonstrated better scores on multiple dimensions ( "role-physical," "mental health," "social functioning," and "general health" ) than those with lower degrees.
After percutaneous device closure of ASD, most adult patients feel that the quality of life is improved compared with that during the preoperative status. With the change of patients' own conditions, their quality of life seems to change differently. In order to better help patients integrate into life, psychological and physical support is still needed.
View full abstract
-
Yan Zhang, Yu-Min Sun, Ying-Jia Xu, Cui-Mei Zhao, Fang Yuan, Xiao-Juan ...
2020 Volume 61 Issue 4 Pages
761-768
Published: July 30, 2020
Released on J-STAGE: July 30, 2020
Advance online publication: July 08, 2020
JOURNAL
FREE ACCESS
Congenital heart defect (CHD) represents the most common birth deformity, afflicting 1% of all births worldwide, and accounts for substantial morbidity and mortality. Increasing evidence highlights the pivotal roles of genetic etiologies in the pathogenesis of CHD, and pathogenic mutations in multiple genes, including TBX5 encoding a cardiac core transcription factor key to cardiovascular morphogenesis, have been involved in CHD. However, due to pronounced genetic heterogeneity of CHD, the genetic determinants underlying CHD in most cases remain obscure. In this investigation, by sequencing analysis of the coding exons and flanking introns of the TBX5 gene in 198 unrelated patients affected with CHD, a novel heterozygous mutation, NM_000192.3: c.692C>T; p. (Pro231Leu), was identified in an index patient with familial double outlet right ventricle (DORV), ventricular septal defect (VSD), and atrioventricular block (AVB). Genetic analysis of the proband's pedigree showed that the mutation co-segregated with the diseases. The missense mutation, which altered the amino acid conserved evolutionarily, was absent from 266 unrelated healthy subjects. Functional analyses with a dual-luciferase reporter assay system unveiled that the Pro231Leu-mutant TBX5 was associated with significantly reduced transcriptional activity on its target genes MYH6 and NPPA. Furthermore, the mutation disrupted the synergistic transactivation between TBX5 and NKX2-5 as well as GATA4, two other transcription factors causally linked to CHD. This study firstly links TBX5 loss-of-function mutation to familial DORV, VSD, and AVB, which provides novel insight into the mechanism underpinning CHD and AVB, suggesting potential implications for genetic evaluation and individualized treatment of patients affected by CHD and AVB.
View full abstract
-
Akihiro Ogawa, Kazuhiro Shimizu, Takahiro Nakagami, Hiroshi Maruoka, K ...
2020 Volume 61 Issue 4 Pages
769-775
Published: July 30, 2020
Released on J-STAGE: July 30, 2020
Advance online publication: July 18, 2020
JOURNAL
FREE ACCESS
The number of heart failure patients is increasing rapidly in Japan because of its large elderly population. As age increases, arterial stiffness and physical dysfunction progress. This study aimed to evaluate the association between the physical function and arterial stiffness in elderly heart failure patients.
This retrospective, observational study includes data from 100 heart failure patients aged ≥ 65 years who were admitted to our hospital and underwent cardiac rehabilitation. The Cardio-Ankle Vascular Index (CAVI) was measured as an indicator of arterial stiffness. Body composition was assessed by bioelectrical impedance analysis. To determine the degree of physical function, we assessed handgrip strength, five-meter walk speed (5MWS), five-repetition sit-to-stand time (5RSST) and six-minute walk distance (6MWD). Sarcopenia was defined using Asian guidelines based on physical function and body composition.
Among 100 patients, 47.0% of patients had sarcopenia. After adjustments for age, sex, atrial fibrillation, and ischemic cardiomyopathy, CAVI was significantly higher in with sarcopenia patients than those without sarcopenia. Age, handgrip strength, 5MWS, 5RSST, and 6MWD were associated with CAVI, and 6MWD was as an independent determinant factor of CAVI.
6MWD was recognized as an accurate physical function indicator. These findings suggested that physical function and arterial stiffness complement each other. To restore cardiac dysfunction, improving both arterial stiffness and physical function might be useful.
View full abstract
-
Yasushi Teshima, Ryosuke Shiga, Shotaro Saito, Hidekazu Kondo, Akira F ...
2020 Volume 61 Issue 4 Pages
776-780
Published: July 30, 2020
Released on J-STAGE: July 30, 2020
Advance online publication: July 18, 2020
JOURNAL
FREE ACCESS
The properties of glucose changes in patients with chronic heart failure remain elusive. In the present study, we investigated the sequential changes of interstitial glucose concentrations in patients with chronic heart failure and heart disease who were not undergoing antidiabetic therapy.
A glucose monitoring device (FreeStyle Libre Pro) was attached to the backside of an upper arm and the interstitial glucose concentration was monitored every 15 minutes for 1 week. Eleven patients with chronic heart failure (Heart failure (+) ) and 7 patients with chronic heart diseases but not with heart failure (Heart failure (−) ) were enrolled. The average level and peak value of interstitial glucose concentrations, and the duration of hyperglycemia (≥ 140 mg/dL) were not significantly different between Heart failure (+) and Heart failure (−). The duration of hypoglycemia (< 80 mg/dL) was significantly longer and the trough value was significantly lower in Heart failure (+) compared with Heart failure (−). Most of the patients in Heart failure (+) were exposed to a long duration of hypoglycemia from midnight to morning. Importantly, none of the patients who showed hypoglycemia complained of any subjective symptoms during hypoglycemia. Malabsorption may be one of the mechanisms of hypoglycemia.
In summary, patients with chronic heart failure are at risk of developing hypoglycemia even if they do not undergo any antidiabetic therapy.
View full abstract
-
Takuya Matsumoto, Satoshi Kodera, Hiroki Shinohara, Hirotaka Ieki, Tos ...
2020 Volume 61 Issue 4 Pages
781-786
Published: July 30, 2020
Released on J-STAGE: July 30, 2020
Advance online publication: July 18, 2020
JOURNAL
FREE ACCESS
The development of deep learning technology has enabled machines to achieve high-level accuracy in interpreting medical images. While many previous studies have examined the detection of pulmonary nodules in chest X-rays using deep learning, the application of this technology to heart failure remains rare. In this paper, we investigated the performance of a deep learning algorithm in terms of diagnosing heart failure using images obtained from chest X-rays. We used 952 chest X-ray images from a labeled database published by the National Institutes of Health. Two cardiologists verified and relabeled a total of 260 "normal" and 378 "heart failure" images, with the remainder being discarded because they had been incorrectly labeled. Data augmentation and transfer learning were used to obtain an accuracy of 82% in diagnosing heart failure using the chest X-ray images. Furthermore, heatmap imaging allowed us to visualize decisions made by the machine. Deep learning can thus help support the diagnosis of heart failure using chest X-ray images.
View full abstract
-
Yuta Torii, Kenya Kusunose, Robert Zheng, Hirotsugu Yamada, Rie Amano, ...
2020 Volume 61 Issue 4 Pages
787-794
Published: July 30, 2020
Released on J-STAGE: July 30, 2020
Advance online publication: July 18, 2020
JOURNAL
FREE ACCESS
Supplementary material
Advanced age, obesity, and muscle weakness are independent factors in the onset of deep vein thrombosis (DVT). Recently, an association between sarcopenia and DVT has been reported. We hypothesized that sarcopenia related factors, observed by ultrasonography, are associated with the regression effect on the thrombus following anticoagulation therapy. The present study focused on gastrocnemius muscle (GCM) thickness and the GCM's internal echogenic brightness. We examined the association with DVT regression following direct oral anticoagulants (DOACs) treatment.
The prospective cohort study period was between October 2017 and August 2018. We enrolled 46 patients diagnosed with DVT by ultrasonography, who were aged >60 years old and treated with DOACs. Sarcopenia was evaluated using the Asian Working Group for Sarcopenia flowchart. The average DOACs treatment period was 94 days, and 29 patients exhibited thrombus regression. On univariate logistic regression analysis, sarcopenia, average GCM diameter index, and gastrocnemius integrated backscatter index were significantly associated with thrombus regression. In a multivariate model, only the average GCM diameter index correlated with thrombus regression.
The average GCM diameter index is associated with DVT regression treated with DOACs. Considering the GCM diameter during DVT treatment can be a marker to make a decision for the treatment of DVT.
View full abstract
-
Jie Ni, Yihai Liu, Mingyue Wu, Jun Wang, Dujuan Sha, Biao Xu
2020 Volume 61 Issue 4 Pages
795-798
Published: July 30, 2020
Released on J-STAGE: July 30, 2020
Advance online publication: July 18, 2020
JOURNAL
FREE ACCESS
To investigate the association of shock on admission with predicting intensive care unit (ICU) mortality, hospital mortality, and neurological outcomes of post cardiac arrest patients.
This was a retrospective study of cardiac arrest (CA) patients admitted to ICU. Student's t test and Chi-square test were performed to compare the difference of non-shock and shock group. Multivariable regression analysis was performed to investigate shock and its association with ICU mortality, hospital mortality, and neurologic outcomes and linear regression analysis to explore its correlation with length of stay in hospital.
A total of 374 CA patients were analyzed, with 200 (53.5%) patients in the presence of shock on admission. Shock was significantly associated with higher ICU mortality (OR 2.42, 95% CI 1.60 to 3.68; P < 0.001), hospital mortality (OR 2.33, 95% CI 1.54 to 3.54; P < 0.001), and more unfavorable neurological outcomes (OR 1.98, 95% CI 1.30 to 3.02; P = 0.001). After adjusting for confounding factors, shock was still an independent predictor of ICU mortality (OR 2.40, 95% CI 1.30 to 4.43; P = 0.005).
Shock on admission of CA patients was significantly associated with ICU mortality.
View full abstract
-
Comparison Between Each Generation
Hisataka Maki, Toru Hara, Masaki Tsuji, Akihito Saito, Shun Minatsuki, ...
2020 Volume 61 Issue 4 Pages
799-805
Published: July 30, 2020
Released on J-STAGE: July 30, 2020
JOURNAL
FREE ACCESS
Therapeutic strategies for pulmonary arterial hypertension (PAH) have made remarkable progress over the last two decades. Currently, 3 types of drugs can be used to treat PAH; prostacyclins, phosphodiesterase 5 inhibitors, and endothelin receptor antagonists (ERA). In Japan, the first generation ERA bosentan was reimbursed in 2005, following which the 2nd generation ERAs ambrisentan and macitentan were reimbursed in 2009 and 2015, respectively. The efficacy of each ERA on hemodynamics in PAH patients remains to be elucidated. The aims of this study were to evaluate the hemodynamic effects of ERAs and compare these effects among each generation of ERAs.
We retrospectively examined the clinical parameters of 42 PAH patients who were prescribed an ERA (15 bosentan, 12 ambrisentan, and 15 macitentan) and who underwent a hemodynamic examination before and after ERA introduction at our institution from January 2007 to July 2019.
In a total of 42 patients, mean pulmonary arterial pressure (mPAP) and pulmonary vascular resistance (PVR) were significantly decreased and cardiac index was significantly increased after ERA introduction (P < 0.001) and the World Health Organization-Functional class (WHO-Fc) was significantly improved after ERA introduction (P = 0.005). Next, in a comparison between 1st and 2nd generation ERAs, 2nd generation ERAs were found to have brought about greater improvements in hemodynamic parameters (mPAP and PVR. P < 0.01), heart rate, brain natriuretic peptide, arterial oxygen saturation, and mixed venous oxygen saturation than the 1st generation ERA bosentan.
We conclude that all ERAs could successfully improve the hemodynamics of PAH patients and that the newer generation ERAs, ambrisentan and macitentan, seemed to be preferable to bosentan.
View full abstract
-
Clinical Implication for Surgery
Riku Arai, Daisuke Fukamachi, Naotaka Akutsu, Yasuo Okumura, Masashi T ...
2020 Volume 61 Issue 4 Pages
831-837
Published: July 30, 2020
Released on J-STAGE: July 30, 2020
JOURNAL
FREE ACCESS
Ventricular septal rupture (VSR) is one of the fatal complications of myocardial infarction in the percutaneous coronary intervention era. A rapid diagnosis, medical and mechanical support, and surgical intervention are required for recovery and survival. In such a situation, the risk of complications associated with surgery is very high, especially in very elderly patients, in which any therapeutic strategy should be carefully discussed by the heart team. Herein, we describe two cases of VSRs after recent myocardial infarction (RMI) in very elderly patients that required debate regarding whether to perform surgery. The patients included a 93-year-old man and 89-year-old man, both of which were not highly frail before the RMI occurred. In the former case, a conservative strategy was adopted because the risk of surgery was considered, but he did not survive. On the other hand, the latter patient underwent surgery and his life was ultimately saved. Based on these two cases, we concluded that even if the patients are very old, if possible, surgical intervention should be fully considered.
View full abstract
-
A Case with a Perimitral Atrial Tachycardia with an Epi-Endocardium Breakthrough
Jun Oikawa, Hidehira Fukaya, Shinichi Niwano, Daiki Saito, Tetsuro Sat ...
2020 Volume 61 Issue 4 Pages
838-842
Published: July 30, 2020
Released on J-STAGE: July 30, 2020
Advance online publication: July 18, 2020
JOURNAL
FREE ACCESS
Complex atrial tachycardias (ATs) after catheter ablation or a MAZE procedure is sometimes difficult to determine the circuits of the tachycardia. A high-density, grid-shapes mapping catheter has been launched, which can be useful for detecting the detail circuits of tachycardias on three-dimensional mapping systems. The signal quality is also important for performing electrophysiological studies (EPSs), such as entrainment mapping, to identify the circuit. This unique mapping catheter has 1 mm electrodes on 2.5 Fr shafts, which improve the signal quality. The high-quality intracardiac electrograms facilitate differentiating small critical potentials, which allows us to perform detailed entrainment mapping in targeted narrow areas. Here, we describe a patient with a perimetral AT with epi-endocardium breakthrough after a MAZE surgery and catheter ablation, which was treated successfully along with detailed entrainment mapping using the HD Grid. This catheter with high-quality signals could be a significant diagnostic tool for a classic EPS as well as for the construction of 3D mapping.
View full abstract
-
Emergency Percutaneous Retrieval and Subsequent Successful Leak Closure in a Patient with Cardiogenic Shock and Multiorgan Failure
Roberta Bottino, Gabriela Tirado-Conte, Angela McInerney, Francisco No ...
2020 Volume 61 Issue 4 Pages
843-847
Published: July 30, 2020
Released on J-STAGE: July 30, 2020
Advance online publication: July 18, 2020
JOURNAL
FREE ACCESS
Paravalvular leak (PVL) is a serious complication of surgical valve replacement, often affecting elderly, multimorbid, high-risk patients. The risk of surgical intervention is often prohibitive in these cases, and so percutaneous PVL closure emerged as a feasible and effective management strategy, with a low complication rate. Specific devices for closure of PVL's are currently not widely available, and so PVLs are closed using generic vascular closure devices, which may result in residual paravalvular regurgitation or even closure device displacement. Although rare, late displacement of the closure device with prosthetic impingement can be life threatening, requiring urgent intervention.
We present a case of a seventy-year-old gentleman with rheumatic heart disease and multiple previous mechanical aortic and mitral valve replacements. After repeated admissions for decompensated heart failure, secondary to paravalvular mitral regurgitation, a percutaneous paravalvular leak closure was performed with successful reduction of the leak. He represented 30 days later with cardiogenic shock and multiorgan failure secondary to torrential central mitral regurgitation caused by late displacement of the closure device with mitral prosthesis impingement. Due to an excessively high surgical risk, his case was successfully managed percutaneously with retrieval of the displaced device and closure of the PVL using two Amplatzer Vascular Plug III devices. At the six-month review, he remains asymptomatic.
Percutaneous PVL closure is an effective strategy for patients with prohibitive surgical risk. Late closure device displacement can be a life-threatening complication. Our case demonstrates that percutaneous management of this complication is feasible even in patients presenting in extremis.
View full abstract
-
Shye-Jao Wu, Ya-Fen Fan
2020 Volume 61 Issue 4 Pages
848-850
Published: July 30, 2020
Released on J-STAGE: July 30, 2020
JOURNAL
FREE ACCESS
Right ventricular (RV) dysfunction may occur after cardiac surgery and it is not rare after corrective repair of tetralogy of Fallot (TOF). If traditional treatments with volume management, infusion of inotropic agents, and use of pulmonary vasodilators cannot stabilize the patient, extracorporeal membrane oxygenation (ECMO) or a ventricular assist device (VAD) will be considered as the last resort. Here, we report a young infant patient with RV failure after corrective repair of TOF and without closure of an atrial septal defect (ASD), who was rescued by veno-venous (VV) -ECMO.
View full abstract
-
A Case Report and Literature Review
Yoichi Iwamoto, Shun Matsumura, Hirotaka Ishido, Hideaki Senzaki, Sato ...
2020 Volume 61 Issue 4 Pages
851-855
Published: July 30, 2020
Released on J-STAGE: July 30, 2020
JOURNAL
FREE ACCESS
Protein-losing enteropathy (PLE) is one of the major complications after a Fontan operation. Some PLE patients suffer from concurrent gastrointestinal bleeding. An effective treatment regimen for such patients has not been established yet. Further, it remains unknown whether PLE and gastrointestinal bleeding coexist independently, or protein losing is associated with gastrointestinal bleeding. We report a 7-year-old steroid-refractory post-Fontan PLE case suggesting the latter pathogenesis together with a literature review.
View full abstract
-
Takayasu Ito, Ryuji Okamoto, Akimasa Matsuda, Yoshito Ogihara, Norikaz ...
2020 Volume 61 Issue 4 Pages
856-858
Published: July 30, 2020
Released on J-STAGE: July 30, 2020
Advance online publication: July 08, 2020
JOURNAL
FREE ACCESS
Nutcracker syndrome (NCS), which is defined as compression of the left renal vein between the aorta and the superior mesenteric artery, is usually benign and self-limiting. Long-term renal venous retention increases the risk of renal vein thrombosis. However, NCS rarely develops into isolated thrombosis of the left renal vein; the reason for this process remains unknown. We describe a young man with antiphospholipid syndrome, who developed overt pulmonary thromboembolism due to an isolated thrombus in the left renal vein. Complicating antiphospholipid syndrome might trigger acute pulmonary thromboembolism (APTE) in patients with NCS. To the best of our knowledge, this is the first report of APTE arising due to isolated left renal vein thrombosis in patients with NCS.
View full abstract
 2020 Volume 61 Issue 4 Pages 705-712
2020 Volume 61 Issue 4 Pages 705-712