
- Issue 12 Pages 695-
- Issue 11 Pages 611-
- Issue 10 Pages 551-
- Issue 9 Pages 485-
- Issue 8 Pages 405-
- Issue 7 Pages 345-
- Issue 6 Pages 281-
- Issue 5 Pages 239-
- Issue 4 Pages 191-
- Issue 3 Pages 137-
- Issue 2 Pages 83-
- Issue 1 Pages 1-
- Issue Special_Issue P・・・
- Issue Supplement2 Pag・・・
- Issue Supplement1 Pag・・・
- |<
- <
- 1
- >
- >|
-
Yurina Saito, Kazuhiro Nishikawa, Tadafumi Asaoka, Kazuyoshi Yamamoto, ...Article type: ORIGINAL ARTICLE
2021Volume 54Issue 12 Pages 839-845
Published: December 01, 2021
Released on J-STAGE: December 28, 2021
JOURNAL OPEN ACCESS FULL-TEXT HTMLPurpose: Preoperative CD4 count is an indicator of outcome in human immunodeficiency virus (HIV)-positive patients who undergo surgery. The aim of this study was to compare the rate of postoperative complications in HIV-positive and HIV-negative patients. We also studied the effect of inguinal hernioplasty on HIV infection status. Materials and Methods: A retrospective study was performed in 316 patients who underwent inguinal hernioplasty from January 2008 and December 2012. Of these patients, 9 were HIV-positive. The rates of surgical site infection (SSI), bleeding, hematoma, seroma, recurrence, chronic pain, and period of hospitalization were compared in the HIV-positive and HIV-negative cases. Data were also collected for perioperative changes in HIV viral titers and CD4 counts in the HIV-positive group. Results: There were no significant differences in the rates of SSI, bleeding, hematoma, seroma, recurrence, chronic pain, and period of hospitalization between the two groups. The median preoperative viral titer and CD4 count were 40 copy/ml and 378 cells/mm3, respectively, and neither of these values changed significantly postoperatively. No patients developed opportunistic infections in the perioperative period. Conclusion: HIV-positive patients with a CD4 count >200 cells/mm3 can safely undergo inguinal hernioplasty, similarly to HIV-negative patients.
View full abstractDownload PDF (565K) Full view HTML
-
Junji Maehara, Nobue Futawatari, Yusuke Akimoto, Ryutaro Watanabe, Yok ...Article type: CASE REPORT
2021Volume 54Issue 12 Pages 846-852
Published: December 01, 2021
Released on J-STAGE: December 28, 2021
JOURNAL OPEN ACCESS FULL-TEXT HTMLA 45-year-old man underwent laparoscopic proximal gastrectomy with jejunal interposition via the antecolic route for early esophagogastric junction cancer four years ago. Nine months postoperatively, a CT scan revealed the transverse colon herniating into the left thoracic cavity through the esophageal hiatus. The size of the hernia gradually increased and the patient experienced respiratory distress during exercise. Thus, laparoscopic hernia repair was performed for esophageal hiatal hernia involving the transverse colon. The herniated transverse colon and omentum were reduced in the abdomen. The size of the hernia orifice was 8 cm. The hiatal hernia defect was closed by primary suture, with mesh placed to overlie the posterior hiatal closure. The postoperative course was uneventful and there has been no recurrence in 6 months after surgery. We report a rare case of laparoscopic hernia repair for esophageal hiatal hernia involving the transverse colon after laparoscopic proximal gastrectomy.
View full abstractDownload PDF (819K) Full view HTML -
Hazuki Miyazaki, Kazuhiro Nishikawa, Takuya Hamakawa, Reishi Toshiyama ...Article type: CASE REPORT
2021Volume 54Issue 12 Pages 853-860
Published: December 01, 2021
Released on J-STAGE: December 28, 2021
 JOURNAL OPEN ACCESS FULL-TEXT HTML
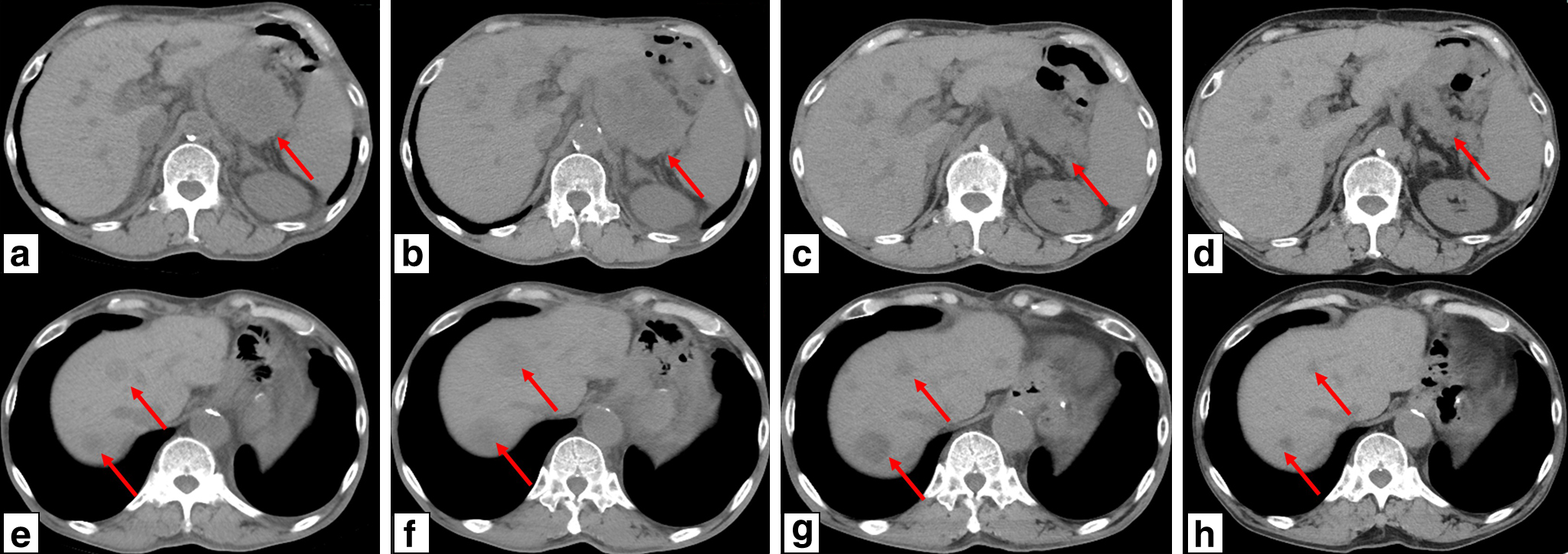
JOURNAL OPEN ACCESS FULL-TEXT HTMLWe report a case of recurrence of HER2-positive esophagogastric junction cancer in which nivolumab was effective as fourth-line treatment. A 71-year-old man underwent distal gastrectomy for gastric cancer 15 years ago. Twelve years after the operation, type 3 cancer was found at the esophagogastric junction, and total remnant gastrectomy and lower esophagectomy were performed. Since recurrence in para-aortic lymph nodes was observed 2 months after the operation, capecitabine+oxaliplatin+trastuzumab therapy was started, and then paclitaxel+ramucirumab and trifluridine/tipiracil were administered. Since increased pancreatic tail lymph node metastasis and new multiple liver metastases were observed during the course, nivolumab was introduced as fourth-line treatment at 1 year and 9 months after the start of the first-line treatment. A temporary increase in lesion growth occurred in during the first course, but after the third course there was a marked reduction of the metastatic lesion and the outcome became a partial response (PR). Both performance status and tumor markers have improved, and PR is currently being maintained.
View full abstractDownload PDF (1440K) Full view HTML -
Naoki Ishizaka, Yudai Kuroiwa, Tsuyoshi Notake, Akira Shimizu, Koji Ku ...Article type: CASE REPORT
2021Volume 54Issue 12 Pages 861-868
Published: December 01, 2021
Released on J-STAGE: December 28, 2021
JOURNAL OPEN ACCESS FULL-TEXT HTMLA 56-year-old woman was found to have a tumor of 2 cm in size on the pancreatic side of the descending part of the duodenum on upper gastrointestinal endoscopy. Abdominal CT showed a 2-cm, well-defined nodule with a poor contrast effect, and a swollen lymph node suspected to be due to lymph node metastasis around the head of the pancreas. Endoscopic ultrasonography (EUS) showed a low echo mass with an irregular margin in the third layer. EUS-guided biopsy led to diagnosis of this region as neuroendocrine neoplasm (NEN), and pancreaticoduodenectomy was performed. Histopathological examination revealed that the tumor had grown just below the mucosa of the accessory papilla of the duodenum and surrounded the accessory pancreatic duct, leading to diagnosis of NEN derived from the accessory papilla of the duodenum. Metastasis of NEN to lymph nodes around the head of the pancreas was also diagnosed. The postoperative course was uneventful and the patient was discharged 22 days after the operation. Most duodenal NEN occurs in the bulb and descending region, whereas NEN in the accessory papilla of the duodenum is rare, with an incidence of only 2.2%. However, NEN derived from the accessory papilla has a high risk of lymph node metastasis, even if the tumor diameter is small. We report a case of resection of NEN of the accessory papilla of the duodenum.
View full abstractDownload PDF (1506K) Full view HTML -
Takumi Habu, Akihiro Sako, Kotaro Nishida, Koichi Komatsu, Keiichi Ara ...Article type: CASE REPORT
2021Volume 54Issue 12 Pages 869-875
Published: December 01, 2021
Released on J-STAGE: December 28, 2021
JOURNAL OPEN ACCESS FULL-TEXT HTMLAn 82-year-old male underwent endoscopic choledocholithotomy and endoscopic gallbladder stenting (EGBS) for acute cholecystitis with choledocholithiasis. Cholecystitis subsided and he was discharged from hospital. However, CT performed for hematemesis 30 days after stenting revealed a pseudoaneurysm in the right hepatic artery, suggesting penetration of the cystic duct. On the same day, the patient was diagnosed with hemobilia due to penetration of the pseudoaneurysm and underwent open hemostasis and cholecystectomy. Subsequently, he was discharged again because of the absence of intra-abdominal complications. The pseudoaneurysm was located adjacent to the stent and was penetrated, resulting in hematemesis and melena. This can be explained by mechanical stimulation, implicating an iatrogenic injury due to EGBS. We herein report a rare case of an iatrogenic pseudoaneurysm that was caused by EGBS and may have been penetrated during the procedure.
View full abstractDownload PDF (1102K) Full view HTML -
Koki Akiyama, Yusuke Ohara, Yohei Owada, Tomoyuki Sugi, Shun Yamanaka, ...Article type: CASE REPORT
2021Volume 54Issue 12 Pages 876-883
Published: December 01, 2021
Released on J-STAGE: December 28, 2021
JOURNAL OPEN ACCESS FULL-TEXT HTMLOsler-Weber-Rendu disease (Osler’s disease or hereditary hemorrhagic telangiectasia) is a rare disease that causes abnormal capillary dilatation in multiple organs. This disease can cause organ disorders due to hemorrhage and shunts; therefore, it requires careful attention during surgery. Here, we report the case of a 65-year-old female with gastrointestinal bleeding due to Osler’s disease who had a history of treatment of surgery, endoscopy, and blood transfusion. The patient underwent colonoscopy for anemia, which revealed sigmoid colon cancer, for which laparoscopic sigmoidectomy was performed. Abnormal dilatation of the mesenteric vessels was present, but precise preoperative hemodynamic evaluation and careful intraoperative maneuver of hemostasis provided a safe surgery without complications.
View full abstractDownload PDF (997K) Full view HTML -
Tomoki Sugimoto, Akira Inoue, Takamichi Komori, Yujiro Nishizawa, Yosh ...Article type: CASE REPORT
2021Volume 54Issue 12 Pages 884-891
Published: December 01, 2021
Released on J-STAGE: December 28, 2021
 JOURNAL OPEN ACCESS FULL-TEXT HTML
JOURNAL OPEN ACCESS FULL-TEXT HTMLThe patient was a 45-year-old man who previously had sexual intercourse with a man. He was referred to our department for left abdominal pain that had persisted for half a year. Colonoscopy revealed a circumferential type 2 tumor with stenosis in the rectosigmoid colon, and biopsy specimens from the tumor revealed a well-differentiated tubular adenocarcinoma. In addition, disseminated round erosions with a white coat were detected on the anal aspect of the tumor. Trophozoite amoeba was identified histologically and the patient was diagnosed with amoebic colitis. Abdominal CT revealed enhanced rectosigmoid wall thickening and swelling of the para-aortic and hilar lymph nodes. Given the risk of anastomotic leakage due to obstructive colitis, a self-expanding metallic stent was placed preoperatively. Twenty days after antibiotic treatment, colonoscopy showed improvement of amoebic colitis. Forty-two days after stent placement, laparoscopic high anterior resection was performed for rectal cancer. The final pathological finding for rectal cancer was pT3N2M1 Stage IV. The patient was discharged on postoperative day 9 without any complications.
View full abstractDownload PDF (1210K) Full view HTML -
Mayu Tashiro, Yoshiki Kajiwara, Takahiro Einama, Hideyuki Shimazaki, E ...Article type: CASE REPORT
2021Volume 54Issue 12 Pages 892-900
Published: December 01, 2021
Released on J-STAGE: December 28, 2021
JOURNAL OPEN ACCESS FULL-TEXT HTMLA 69-year-old man was diagnosed with anastomotic recurrence two and a half years after he underwent lower anterior resection for Stage IIIa upper rectal cancer. In a preoperative examination, contrast-enhanced CT showed a smooth-contour tumor of 2 cm in diameter anterior to the inferior vena cava. The tumor adjoined the inferior part of the third portion of the duodenum and had enlarged over time. FDG positron emission tomography showed abnormal uptake in the tumor. As we considered that the tumor was derived from retroperitoneum tissue, we first performed super-low anterior resection with a diverting ileostomy for anastomotic recurrence. However, endoscopic ultrasonographic fine needle aspiration cytology after surgery strongly suggested that the tumor was an adenocarcinoma. Since no other primary lesions were found, the tumor was diagnosed as recurrence of rectal cancer and was resected at the time of stoma closure. The pathological findings were consistent with metastasis of rectal cancer.
View full abstractDownload PDF (1536K) Full view HTML -
Taku Hattori, Satoru Takayama, Kohei Takura, Koshiro Harata, Masaki Sa ...Article type: CASE REPORT
2021Volume 54Issue 12 Pages 901-908
Published: December 01, 2021
Released on J-STAGE: December 28, 2021
JOURNAL OPEN ACCESS FULL-TEXT HTMLThere have been many reported cases of treatment for median arcuate ligament syndrome (MALS), but definite criteria for diagnosis remain controversial. Duplex US and CT angiography can suggest findings consistent with MALS, but differential diagnosis of celiac trunk stenosis should also be considered. We report a case of pancreaticoduodenal artery aneurysm associated with MALS that was diagnosed with intravascular ultrasound and treated by transcatheter arterial embolization and laparoscopic release of the median arcuate ligament.
View full abstractDownload PDF (1300K) Full view HTML -
Tetsuro Tominaga, Takashi Nonaka, Akiko Fukuda, Masaaki Moriyama, Shos ...Article type: CASE REPORT
2021Volume 54Issue 12 Pages 909-916
Published: December 01, 2021
Released on J-STAGE: December 28, 2021
JOURNAL OPEN ACCESS FULL-TEXT HTMLMost myelolipomas arise from the adrenal gland. Occurrence of this tumor in the pelvic space is extremely rare and there is no report of the tumor arising from the lateral pelvic area. We present a case of a 52-year-old woman with extra-adrenal myelolipoma. Abdominal CT incidentally detected a mass of 36×34 mm that contained fat density in the right lateral pelvic area. The tumor increased to 44×35 mm in diameter during one year of follow up. MRI showed a decrease of the apparent diffusion coefficient in the solid part of the tumor, which was suspected to have malignant potential. Laparoscopic tumor resection was then performed. The tumor was 40×40×20 mm in size. The histopathological diagnosis was extra-adrenal myelolipoma composed of hematopoietic elements and mature fat tissue. The postoperative course was uneventful, and the patient was discharged at 9 days postoperatively. In cases of myelolipoma, a detailed examination and use of appropriate follow-up by imaging are crucial for differential diagnosis and choice of an appropriate surgical approach.
View full abstractDownload PDF (1424K) Full view HTML
-
Tsutomu FujiiArticle type: EDITOR'S NOTE
2021Volume 54Issue 12 Pages en12-
Published: December 01, 2021
Released on J-STAGE: December 28, 2021
JOURNAL OPEN ACCESS FULL-TEXT HTMLDownload PDF (164K) Full view HTML
- |<
- <
- 1
- >
- >|