
- Issue 12 Pages 695-
- Issue 11 Pages 611-
- Issue 10 Pages 551-
- Issue 9 Pages 485-
- Issue 8 Pages 405-
- Issue 7 Pages 345-
- Issue 6 Pages 281-
- Issue 5 Pages 239-
- Issue 4 Pages 191-
- Issue 3 Pages 137-
- Issue 2 Pages 83-
- Issue 1 Pages 1-
- Issue Special_Issue P・・・
- Issue Supplement2 Pag・・・
- Issue Supplement1 Pag・・・
- |<
- <
- 1
- >
- >|
-
Kohei Kasahara, Takashi Kosaka, Sho Sato, Yusaku Tanaka, Hiroshi Miyam ...Article type: CASE REPORT
2021Volume 54Issue 8 Pages 505-513
Published: August 01, 2021
Released on J-STAGE: August 31, 2021
JOURNAL OPEN ACCESS FULL-TEXT HTMLA 43-year-old male presented with dizziness due to severe anemia. Gastrointestinal endoscopy revealed a large submucosal tumor with bleeding from the ulcer in the anterior wall of the upper stomach. A biopsy specimen indicated a gastrointestinal stromal tumor (GIST). Abdominal enhanced CT revealed an extraluminal growth type GIST of 11.0 cm in diameter and a contrast defect in the left gastric vein extending to the splenic vein and portal vein trunk. FDG-PET/CT showed abnormal accumulation in the gastric main tumor (SUVmax 9.9) and intravascular contrast defect (SUVmax 5.6). These findings led to diagnosis of GIST with a tumor embolus in the portal vein. The patient underwent total gastrectomy with distal pancreatomy with splenectomy and removal of the tumor embolus in the portal vein. Pathological examination of the resected specimen revealed proliferation of spindle cells. Immunohistochemical staining was positive for CD117 (c-kit), DOG1 and CD34, and negative for S-100. Anticoagulant therapy was administered for postoperative portal thrombus. The patient was discharged on the 38th hospital day. Postoperative chemotherapy with imatinib mesylate was started, and the patient is presently alive without recurrence 12 months after surgery.
View full abstractDownload PDF (1506K) Full view HTML -
Yoshiaki Tatsumi, Tetsuya Sakai, Takashi Ito, Katsuya Ami, Masaki Tana ...Article type: CASE REPORT
2021Volume 54Issue 8 Pages 514-522
Published: August 01, 2021
Released on J-STAGE: August 31, 2021
 JOURNAL OPEN ACCESS FULL-TEXT HTML
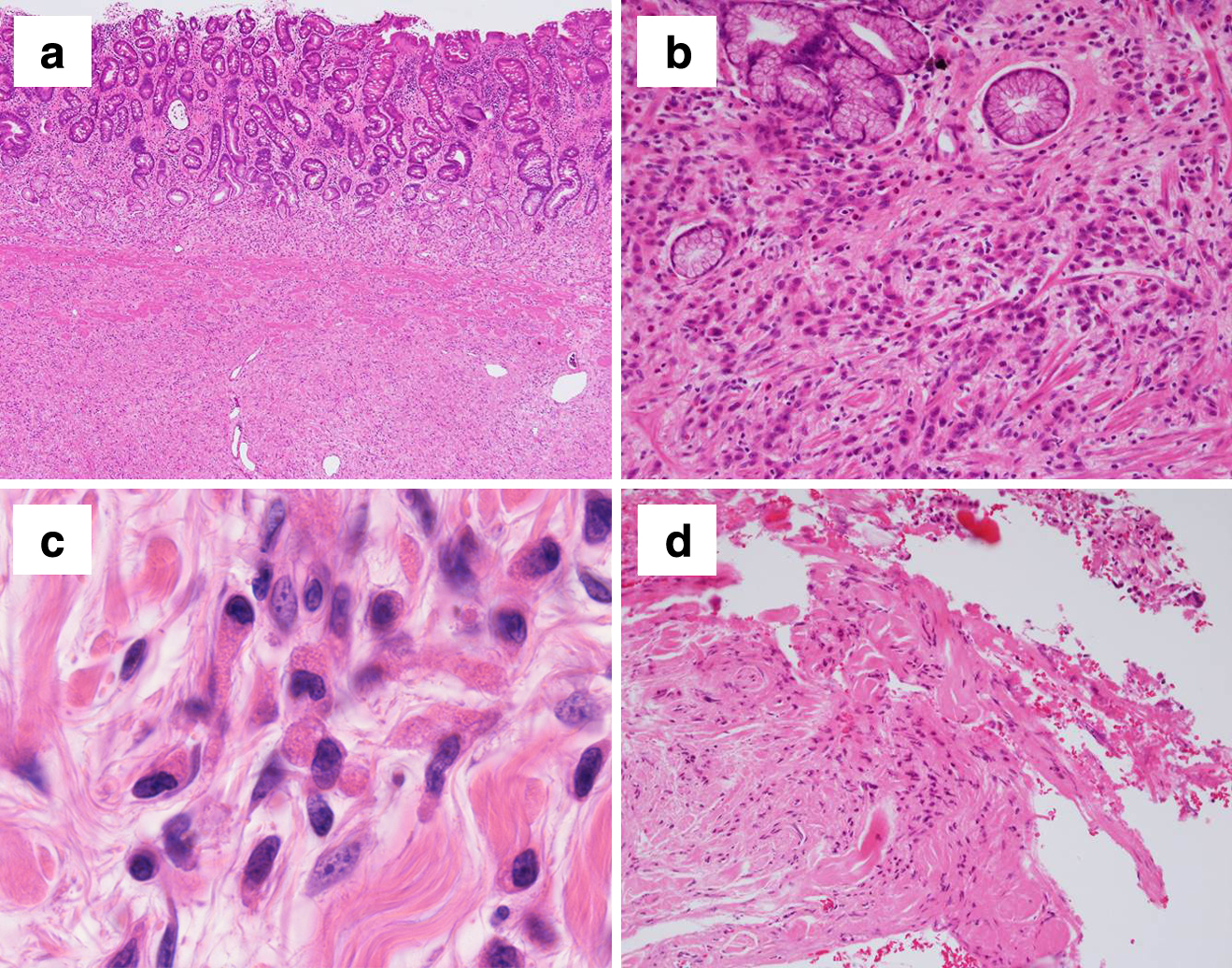
JOURNAL OPEN ACCESS FULL-TEXT HTMLA 76-year-old woman was referred to our hospital for complaints of nausea, loss of appetite, and an upper abdominal mass,. Initially, she was diagnosed with multiple gastric ulcers with Helicobacter pylori infection by upper gastrointestinal endoscopy, and medication was administered. However, reexamination by endoscopy after this treatment revealed type 4 advanced gastric cancer, special type (miscellaneous carcinoma). Additional tests, including immunostaining with anti-lysozyme antibody (lysozyme staining), revealed Paneth cell gastric cancer (World Health Organization classification) and distal gastrectomy was performed. Twenty-two months after the operation, there was no obvious recurrence. Paneth cells are found in gastric mucosa as a result of intestinal metaplasia. Several studies have reported that Paneth cell-like cells containing positive granules that stain with lysozyme are found in gastric cancer tissue during the process of carcinogenesis. However, Paneth cell gastric cancer, in which small tumor cells containing granules in the cytoplasm infiltrate diffusely, as in the present case, is extremely rare.
View full abstractDownload PDF (2282K) Full view HTML -
Takahiro Haruna, Tadashi Yokoyama, Hiroshi Maruyama, Atsushi Hirakata, ...Article type: CASE REPORT
2021Volume 54Issue 8 Pages 523-530
Published: August 01, 2021
Released on J-STAGE: August 31, 2021
JOURNAL OPEN ACCESS FULL-TEXT HTMLAn 85-year-old woman was diagnosed with locally advanced pancreatic carcinoma involving the superior mesenteric artery and portal vein. She underwent subtotal stomach-preserving pancreaticoduodenectomy with portal vein resection after chemoradiotherapy. The postoperative course was uneventful. However, she was readmitted to our hospital with anemia and melena 3 months postoperatively. CT showed an obstructed portal vein and formation of collaterals adjacent to the hepaticojejunostomy site. Double-balloon endoscopy revealed red color sign-positive varices around the hepaticojejunostomy site, and hemorrhage from the varices was diagnosed. Endoscopic therapy was not possible because it was difficult to maintain a table position for endoscopy. Therefore, partial splenic embolization (PSE) was performed to reduce portal venous pressure and control the hemorrhage. Melena and anemia have not occurred after PSE. Ectopic variceal hemorrhage caused by extrahepatic portal vein obstruction is a lethal complication after intraperitoneal surgery, and early detection and treatment of the hemorrhagic source remain difficult. No guidelines for variceal hemorrhage around the hepaticojejunostomy site have been established. This case suggests that PSE should be considered as treatment for variceal hemorrhage around the hepaticojejunostomy site.
View full abstractDownload PDF (886K) Full view HTML -
Naoki Ikenaga, Akira Inoue, Takamichi Komori, Yujiro Nishizawa, Hisate ...Article type: CASE REPORT
2021Volume 54Issue 8 Pages 531-537
Published: August 01, 2021
Released on J-STAGE: August 31, 2021
JOURNAL OPEN ACCESS FULL-TEXT HTMLThe patient was a 68-year-old man who underwent laparoscopic super-low anterior resection with bilateral lymph node dissection for lower rectal cancer. The histopathological diagnosis was pT2N0M0, pStage I. Postoperatively, paralytic ileus occurred, but the patient was discharged after conservative treatment. Three months after surgery, the patient presented to our hospital as an emergency for a complaint of severe right inguinal pain. An abdominal contrast-enhanced CT scan revealed a closed loop of the small intestine on the right side of the pelvis, and an emergency operation was performed under a diagnosis of strangulated bowel obstruction. Intraoperative findings revealed that the small intestine had strayed into the gap between the right upper bladder artery and the right internal iliac artery, which had been exposed by lateral lymph node dissection. The small intestine was entrapped and necrotic, but the entrapment was easily released. After confirming that the left upper bladder and right lower bladder arteries were preserved, we decided to ligate and dissect the right upper bladder artery to prevent recurrence of the entrapment. Partial resection of the small intestine, including the necrotic intestine, and anastomotic reconstruction were then performed. A histopathological examination showed necrosis of the entire intestinal wall. We believe that this is the first reported case of strangulated bowel obstruction caused by exposed blood vessels after laparoscopic super-low anterior resection with lateral lymph node dissection for rectal cancer.
View full abstractDownload PDF (993K) Full view HTML -
Misaki Matsumiya, Masaru Koizumi, Naoya Kasahara, Kazuhiro Endo, Hidek ...Article type: CASE REPORT
2021Volume 54Issue 8 Pages 538-547
Published: August 01, 2021
Released on J-STAGE: August 31, 2021
 JOURNAL OPEN ACCESS FULL-TEXT HTML
JOURNAL OPEN ACCESS FULL-TEXT HTMLA 48-year-old man underwent skin grafting from the left inguinal region to the left forearm one month previously. He noticed abdominal discomfort after discharge and was admitted to another hospital because of progression of abdominal pain and a decreased level of consciousness. An enhanced CT scan revealed extensive portal venous thrombosis. Lower gastrointestinal bleeding developed the following day, and he was transferred to our hospital and diagnosed with superior mesenteric venous thrombosis. Enhanced CT showed no intestinal necrosis. Anticoagulant therapy was started and the thrombosis had almost resolved 40 days later. However, after starting oral intake, the patient developed vomiting. Small bowel radiographs and 3D-CT showed significant proximal intestinal stenosis. Small bowel resection was performed on the 59th day after transfer. The pathological diagnosis was ischemic enteritis with venous thrombosis. The patient was discharged 20 days after intestinal resection and he has had no recurrence of symptoms. In this case, 3D-CT was useful to determine the range of intestinal stenosis and the required area of resection.
View full abstractDownload PDF (1337K) Full view HTML -
Yasunori Tsuchiya, Tetsuya Omura, Nagayoshi Ota, Shozo Hojo, Koshi Mat ...Article type: CASE REPORT
2021Volume 54Issue 8 Pages 548-555
Published: August 01, 2021
Released on J-STAGE: August 31, 2021
JOURNAL OPEN ACCESS FULL-TEXT HTMLA 75-year old woman with a history of hypertension, hyperlipidemia and surgery for uterine myoma underwent laparoscopic sigmoidectomy and D3 lymph node dissection for sigmoid colon cancer. Constipation, anal discomfort, and clear drainage from the anus began 5 months after the operation, and a month later she visited our hospital. At 6 months after laparoscopic sigmoidectomy, CT revealed a severely thickened rectum from the anastomosis to the anus and dilatation of the internal iliac vein; and colonoscopy revealed severe erosion from the anastomosis to the anal side. Conservative treatment for about one month did not improve her symptoms and findings, and she then developed extensive anal bleeding and hypovolemic shock. Severe edema and fibrosis of the rectum and surrounding tissue were found in an emergency operation, and abdominoperineal resection was performed. Macroscopic findings of the resected specimen showed a severely thickened rectum wall. Histological findings showed dilated and meandering veins with congestion from the rectal submucosa to perirectal tissue. We suspected that this ischemic colitis was caused by venous stasis due to two pelvic surgeries.
View full abstractDownload PDF (1787K) Full view HTML -
Shodai Mizuno, Ryo Seishima, Koji Okabayashi, Masashi Tsuruta, Kohei S ...Article type: CASE REPORT
2021Volume 54Issue 8 Pages 556-562
Published: August 01, 2021
Released on J-STAGE: August 31, 2021
JOURNAL OPEN ACCESS FULL-TEXT HTMLA 24-year-old woman visited the emergency room at our hospital with a complaint of left abdominal pain. She had a history of bilateral internal carotid artery dissection and bilateral vertebral artery dissection and had been diagnosed with vascular Ehlers-Danlos syndrome (EDS) 8 months before. Abdominal CT at the time of her visit revealed intramural emphysema and free air at the splenic curve of the colon, which suggested colonic perforation. Given that abdominal pain was localized, making it unlikely to be due to peritonitis, and that there are high risks associated with surgery in patients with vascular EDS, we chose conservative treatment. After admission, the inflammatory reaction and abdominal symptom improved steadily, and she was discharged on the 29th hospital day. Although surgery is a basic treatment strategy for colonic perforation, a careful decision is required since delayed wound healing often causes serious postoperative complications. This case suggests that conservative treatment can be an option if symptoms are mild and the general condition is relatively good in patients who have been diagnosed with vascular EDS.
View full abstractDownload PDF (857K) Full view HTML -
Toshihiro Soeta, Hiroo Naito, Naoki Akishige, Takahiro Tsuchiya, Shun ...Article type: CASE REPORT
2021Volume 54Issue 8 Pages 563-570
Published: August 01, 2021
Released on J-STAGE: August 31, 2021
JOURNAL OPEN ACCESS FULL-TEXT HTMLA 63-year old woman was admitted to our hospital due to appetite loss and persistent left abdominal pain. Laboratory data showed severe leukocytosis with elevated white blood cells (WBCs) (76,900/mm3). Transverse colon cancer was diagnosed based on CT and colonoscopy. There were no findings suggestive of infections or blood malignancy, but granulocyte-colony stimulating factor (G-CSF) was elevated to 340 pg/ml. Thus, colon cancer with production of G-CSF was suspected. Left colectomy, pancreatic tail resection and splenectomy with covering ileostomy were performed. Pathological findings indicated that the tumor was adenocarcinoma that was immunohistochemically positive for G-CSF. The serum G-CSF level and WBC count decreased to normal ranges after the operation. The final diagnosis was G-CSF-producing colon cancer. On postoperative day 21, the WBC count increased to 17,500/mm3 and CT revealed liver metastasis. Systemic chemotherapy was administered, but the patient died 14 months after the operation. We present this case as an extremely rare example of G-CSF-producing colon cancer as a tumor with a poor prognosis.
View full abstractDownload PDF (1092K) Full view HTML -
Osamu Inamoto, Shigeo Kyutoku, Kazuyuki Okada, Yuya Miyauchi, Hidekazu ...Article type: CASE REPORT
2021Volume 54Issue 8 Pages 571-578
Published: August 01, 2021
Released on J-STAGE: August 31, 2021
JOURNAL OPEN ACCESS FULL-TEXT HTMLA 64-year-old woman underwent endoscopic resection for a neuroendocrine tumor of the lower rectum. Histological examination showed a positive vertical margin and vascular invasion. Additional laparoscopic intersphincteric rectal resection with ileostomy was then performed. Three months after the operation, a gastrografin enema showed that the space on the ventral side of the colorectal anastomosis was filled with contrast agent, and a rectovaginal fistula was diagnosed. At first, simple suture closure of the fistula was performed under lumbar anesthesia, but the fistula recurred. Seven months after the initial surgery, filling of the internal pudendal artery perforator flap was performed. The postoperative course was uneventful and the patient was discharged 9 days after the operation. Currently, there has been no recurrence of the fistula for 16 months after flap filling. There have been reports of various treatments for rectovaginal fistula after rectal resection, but relatively few have focused on internal pudendal artery perforator flap filling. We report this case with a review of the literature.
View full abstractDownload PDF (1256K) Full view HTML
-
Hiroya KuroyanagiArticle type: EDITOR'S NOTE
2021Volume 54Issue 8 Pages en8-
Published: August 01, 2021
Released on J-STAGE: August 31, 2021
JOURNAL OPEN ACCESS FULL-TEXT HTMLDownload PDF (174K) Full view HTML
- |<
- <
- 1
- >
- >|