
- |<
- <
- 1
- >
- >|
-
Satoru OSHINO, Naoki TANI, Hui Ming KHOO, Kuriko KAGITANI-SHIMONO, Shi ...2023 年 63 巻 5 号 p. 173-178
発行日: 2023/05/15
公開日: 2023/05/15
[早期公開] 公開日: 2023/04/06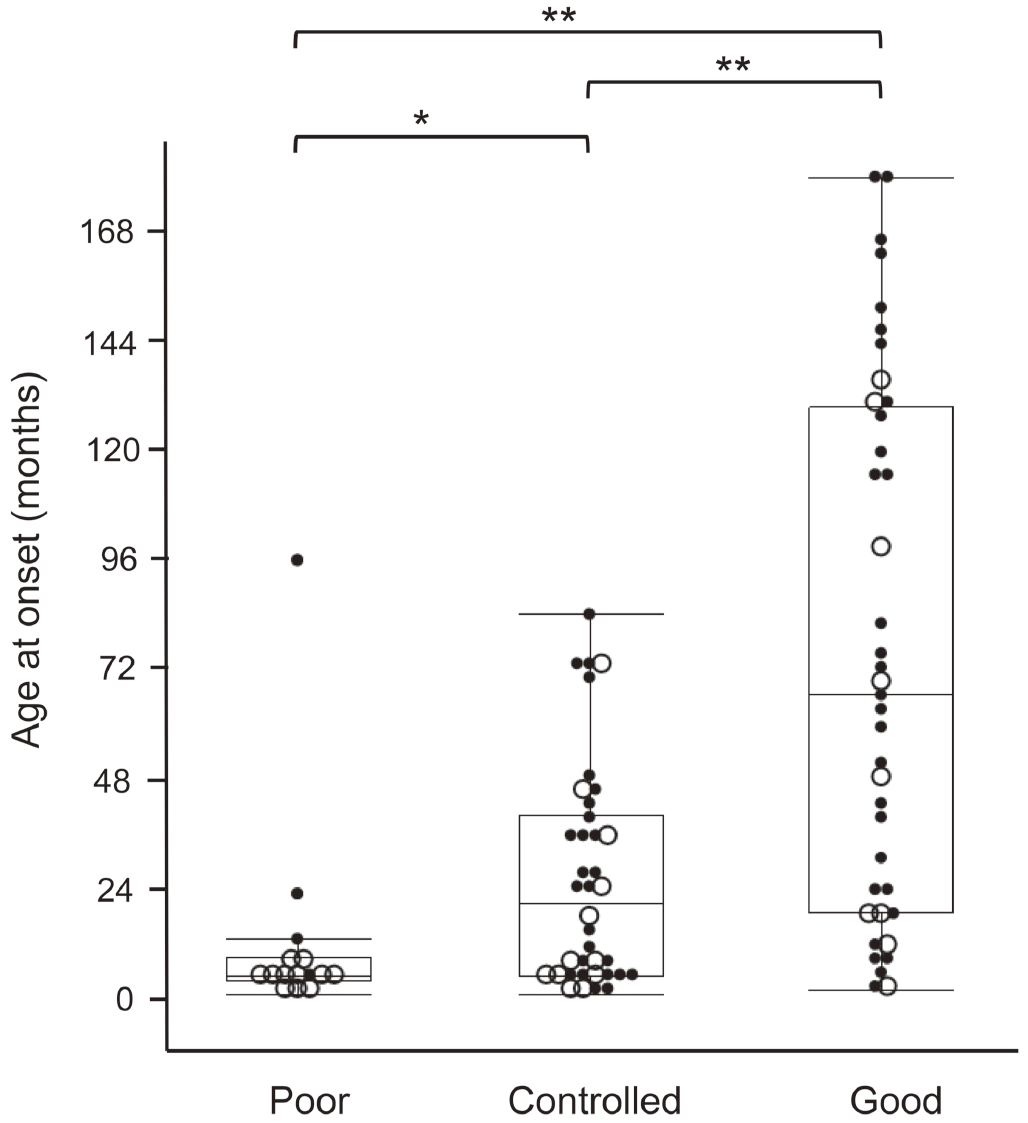 ジャーナル オープンアクセス
ジャーナル オープンアクセスSuccessful surgery for drug-resistant pediatric epilepsy can facilitate motor and cognitive development and improve quality of life by resolution or reduction of epileptic seizures. Therefore, surgery should be considered early in the disease course. However, in some cases, the estimated surgical outcomes are not achieved, and additional surgical treatments are considered. In this study, we investigated the clinical factors related with such unsatisfactory outcomes.
We reviewed the clinical data of 92 patients who underwent 112 surgical procedures (69 resection and 53 palliation procedures). Surgical outcomes were assessed according to the postoperative disease status, which was classified as good, controlled, and poor. The following clinical factors were analyzed in relation to surgical outcome: sex, age at onset, etiology (malformation of cortical development, tumor, temporal lobe epilepsy, scar, inflammation, and non-lesional epilepsy), presence of genetic cause, and history of developmental epileptic encephalopathy. At a median of 59 (30-81.25) months after the initial surgery, the disease status was good in 38 (41%), controlled in 39 (42%), and poor in 15 (16%) patients. Among the evaluated factors, etiology exhibited the strongest correlation with surgical outcomes. Tumor-induced and temporal lobe epilepsy were correlated with good, whereas malformation of cortical development, early seizure onset, and presence of genetic cause were correlated with poor disease status. Although epilepsy surgery for the patients who present with the latter factors is challenging, these patients demonstrate a greater need for surgical treatment. Hence, development of more effective surgical options is warranted, including palliative procedures.
抄録全体を表示PDF形式でダウンロード (223K) -
Satoshi MAESAWA, Tomotaka ISHIZAKI, Manabu MUTOH, Yoshiki ITO, Jun TOR ...2023 年 63 巻 5 号 p. 179-190
発行日: 2023/05/15
公開日: 2023/05/15
[早期公開] 公開日: 2023/03/31 ジャーナル オープンアクセス
ジャーナル オープンアクセスStereotactic electroencephalography (SEEG) is receiving increasing attention as a safe and effective technique in the invasive evaluation for epileptogenic zone (EZ) detection. The main clinical question is whether the use of SEEG truly improves outcomes. Herein, we compared outcomes in our patients after three types of intracranial EEG (iEEG): SEEG, the subdural electrode (SDE), and a combined method using depth and strip electrodes. We present here our preliminary results from two demonstrative cases. Several international reports from large epilepsy centers found the following clinical advantages of SEEG: 1) three-dimensional analysis of structures, including bilateral and multilobar structures; 2) low rate of complications; 3) less pneumoencephalopathy and less patient burden during postoperative course, which allows the initiation of video-EEG monitoring immediately after implantation and does not require resection to be performed in the same hospitalization; and 4) a higher rate of good seizure control after resection. In other words, SEEG more accurately identified the EZ than the SDE method. We obtained similar results in our preliminary experiences under limited conditions. In Japan, as of August 2022, dedicated electrodes and SEEG accessories have not been approved and the use of the robot arm is not widespread. The Japanese medical community is hopeful that these issues will soon be resolved and that the experience with SEEG in Japan will align with that of large epilepsy centers internationally.
抄録全体を表示PDF形式でダウンロード (2101K)
-
Kazuhiro WAKAMATSU, Sumio ISHIAI, Nobuko AIHARA, Sho KUROKAWA, Yusuke ...2023 年 63 巻 5 号 p. 191-199
発行日: 2023/05/15
公開日: 2023/05/15
[早期公開] 公開日: 2023/03/01 ジャーナル オープンアクセス
ジャーナル オープンアクセス
電子付録Language tasks for monitoring intraoperative language symptoms have not yet been established. This study aimed to examine whether the quantitative evaluation of language function with visual and auditory naming during awake craniotomy predicts early postoperative language function in patients. Thirty-seven patients with brain tumors in the language-dominant hemisphere were included. They underwent visual and auditory naming preoperatively and at the end of tumor resection for intraoperative evaluation. Using the Western Aphasia Battery, their overall language functions were evaluated preoperatively, early postoperatively (within 1 week), and late postoperatively (after 1 month). The preoperative and intraoperative changes in the visual and auditory naming scores were significantly correlated with most of the Western Aphasia Battery score changes between the preoperative and early postoperative evaluations, which was more remarkable for auditory naming. Multiple linear regression analysis showed that changes in the auditory naming score predicted the preoperative to early postoperative changes in the aphasia quotient of the Western Aphasia Battery. Receiver operating characteristics analysis showed a higher area under the curve or discriminative power for auditory than visual naming in predicting the development or exacerbation of aphasia in the early postoperative period. Considering the analyses applied separately for low- and high-grade glioma, auditory naming, which taps into a wider range of linguistic functions, may be more informative than visual naming as language evaluation in awake craniotomy for the early postoperative development of aphasia, especially for patients with high-grade glioma.
抄録全体を表示PDF形式でダウンロード (386K) -
Yoshitaka NAGASHIMA, Yusuke NISHIMURA, Takayuki AWAYA, Nobuhiro HATA, ...2023 年 63 巻 5 号 p. 200-205
発行日: 2023/05/15
公開日: 2023/05/15
[早期公開] 公開日: 2023/04/13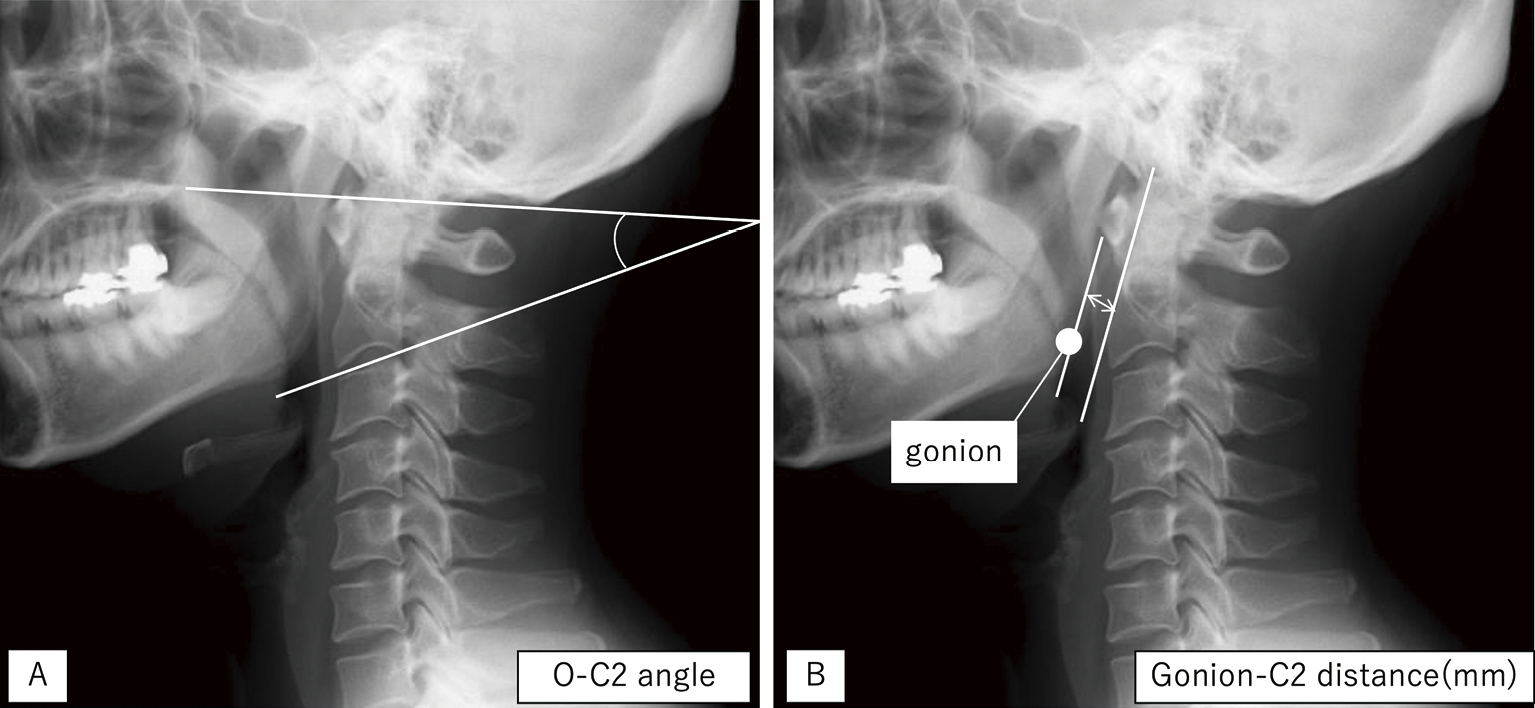 ジャーナル オープンアクセス
ジャーナル オープンアクセスThe Occipito (O) -C2 angle reflects the correct craniocervical spine alignment; however, the poor image quality of standard intraoperative fluoroscopy at times lead to inaccurate measurements. Herein, we preliminarily investigated the relationship between the O-C2 angle and the Gonion-C2 distance, which is based on the positioning of the mandible and the cervical spine. We enrolled patients who underwent cervical spine radiography in neutral, flexion, and extension positions from January 2020 to October 2020. The difference by posture changes for each parameter was defined as the Δ value, and the Spearman's rank correlation coefficient was determined. Furthermore, we determined the cutoff value of the ΔGonion-C2 distance to predict a decrease of > 10° in the ΔO-C2 angle, which is reported to be related to dysphagia and dyspnea. Seventy-four patients were included. Spearman's rank correlations for the neutral, flexion, and extension positions were 0.630 (P < 0.001), 0.471 (P < 0.001), and 0.625 (P < 0.001), respectively, while the cutoff values of the ΔGonion-C2 distance for predicting > 10° in the ΔO-C2 angle were 9.3 mm for the neutral flexion change (sensitivity: 0.435, specificity: 0.882) and 8.3 mm for the extension-neutral change (sensitivity: 0.712, specificity: 0.909). The O-C2 angle and Gonion-C2 distances correlated; however, this correlation was weaker in the flexed position. Nevertheless, the ΔGonion-C2 distance can be used as a warning sign for postoperative complications after posterior occipital bone fusion surgery, because a decrease of > 10° in the ΔO-C2 angle can be predicted with high specificity.
抄録全体を表示PDF形式でダウンロード (408K) -
Daijiro MORIMOTO, Kyongsong KIM, Rinko KOKUBO, Takao KITAMURA, Toyohik ...2023 年 63 巻 5 号 p. 206-212
発行日: 2023/05/15
公開日: 2023/05/15
[早期公開] 公開日: 2023/04/06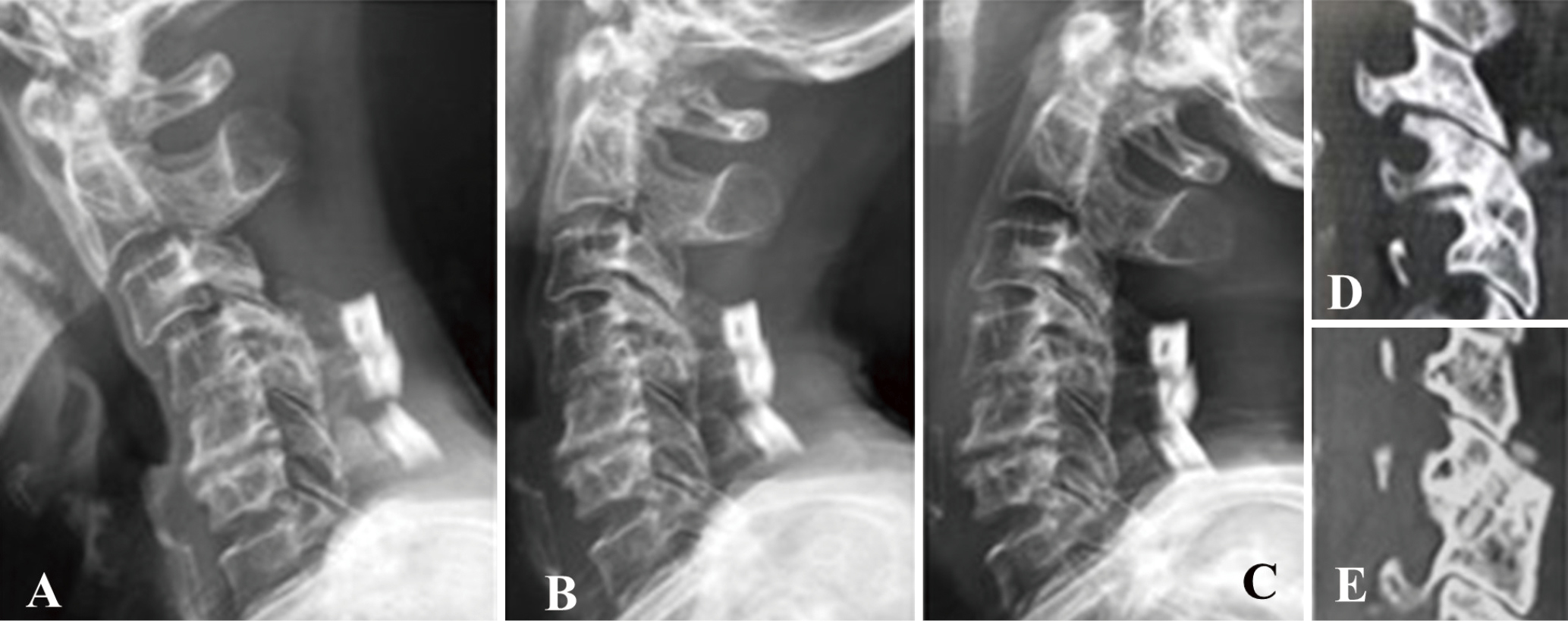 ジャーナル オープンアクセス
ジャーナル オープンアクセスTransarticular screw fixation is a method for posterior cervical fixation. It is ergonomic because neither connectors nor rods are needed. Biomechanical studies have shown that its fixation force is not inferior to that of lateral mass screws. More information is needed on the surgical outcome of procedures using bioabsorptive screws. We investigated the long-term surgical and radiological outcomes of posterior cervical decompression and fusion using bioabsorptive screws for transarticular fixation.
Of 10 patients who underwent cervical spine transarticular fixation using bioabsorptive screws, nine presented with cervical degenerative spondylosis and one with a traumatic cervical spine injury. The mean postoperative follow-up period was 57.1 months. Transarticular screw fixation was successful in all 10 patients; no intraoperative complications were encountered. Bilateral screw breakage was discovered in a patient with cervical spine instability and associated dystonia due to cerebral palsy; there was no symptom deterioration, facet joint breakage, or instability exacerbation. Facet fusion was obtained in the nine other patients. At the patients' last visit, their clinical symptoms were significantly improved. Whole cervical spine alignment (−4.21 ± 7.2 to −5.2 ± 8.7) and the fused segment angle (mean, −0.1 ± 9.9 to −1.2 ± 13.7) did not significantly worsen postoperatively (mean: −0.1 ± 9.9 to −1.2 ± 13.7). Transarticular fixation using bioabsorptive screws is safe and associated with good long-term outcomes. In patients with exacerbation of local instability after posterior decompression, additional transarticular fixation using bioabsorbable screws is a treatment option.
抄録全体を表示PDF形式でダウンロード (713K)
-
Fumihiro HIRAOKA, Shigetoshi YANO, Hiroya MORITA, Kousei MARUYAMA, Kai ...2023 年 63 巻 5 号 p. 213-219
発行日: 2023/05/15
公開日: 2023/05/15
[早期公開] 公開日: 2023/02/08 ジャーナル オープンアクセス
ジャーナル オープンアクセスWe describe a three-step, simple binostril approach to endoscopic endonasal transsphenoidal surgery in cases of sellar/parasellar lesions. In the first step, the mucosa of the lower third of the ethmoid bulla on the outside was coagulated with monopolar microdissection needle and opened to create space on the outside of the middle turbinate. The middle turbinate was moved outward using this space, and the natural ostium of the sphenoid sinus could be confirmed easily. In the second step, a less than 10 mm incision was made from the right natural ostium of the sphenoid sinus to the right nasal septal mucosa. The anterior wall of the sphenoid sinus was removed to free the sphenoid sinus. In the third step, the instrument was inserted through the left nostril using a hole connected to the natural ostium of the sphenoid sinus to reach the sellar floor via both nostrils. It took longer for the trainee than for the instructor to reach the sellar floor in the first four cases. However, there was no significant difference in the approach time after the fifth case. Approach-related postoperative complications were observed in 52 cases of sellar/parasellar lesions performed. This approach was considered to provide sufficient space and was simple and less burdensome to the patient.
抄録全体を表示PDF形式でダウンロード (458K)
-
2023 年 63 巻 5 号 p. 220
発行日: 2023/05/15
公開日: 2023/05/15
ジャーナル オープンアクセスPDF形式でダウンロード (39K)
-
2023 年 63 巻 5 号 p. EC9-EC10
発行日: 2023/05/15
公開日: 2023/05/15
ジャーナル オープンアクセスPDF形式でダウンロード (54K)
- |<
- <
- 1
- >
- >|