
- |<
- <
- 1
- >
- >|
-
Nayuta HIGA, Toshiaki AKAHANE, Seiya YOKOYAMA, Hajime YONEZAWA, Hiroyu ...2022 年 62 巻 9 号 p. 391-399
発行日: 2022/09/15
公開日: 2022/09/15
[早期公開] 公開日: 2022/08/27 ジャーナル オープンアクセス
ジャーナル オープンアクセス
電子付録Rapid technological advances in molecular biology, including next-generation sequencing, have identified key genetic alterations in central nervous system (CNS) tumors. Accordingly, the fifth edition of the World Health Organization (WHO) CNS tumor classification was published in 2021. We analyzed 303 patients with diffuse glioma using an amplicon-based glioma-tailored gene panel for detecting 1p/19q codeletion and driver gene mutations such as IDH1/2, TERTp, EGFR, and CDKN2A/B on a single platform. Within glioblastomas (GBMs), the most commonly mutated genes were TERTp, TP53, PTEN, NF1, and PDGFRA, which was the most frequently mutated tyrosine kinase receptor in GBM, followed by EGFR. The genes that most commonly showed evidence of loss were PTEN, CDKN2A/B, and RB1, whereas the genes that most commonly showed evidence of gain/amplification were EGFR, PDGFRA, and CDK4. In 22 grade III oligodendroglial tumors, 3 (14%) patients had CDKN2A/B homozygous deletion, and 4 (18%) patients had ARID1A mutation. In grade III oligodendroglial tumors, an ARID1A mutation was associated with worse progression-free survival. Reclassification based on the WHO 2021 classification resulted in 62.5% of grade II/III isocitrate dehydrogenase (IDH) -wildtype astrocytomas being classified as IDH-wildtype GBM and 37.5% as not elsewhere classified. In summary, our glioma-tailored gene panel was applicable for molecular diagnosis in the WHO 2021 classification. In addition, we successfully reclassified the 303 diffuse glioma cases based on the WHO 2021 classification and clarified the genetic profile of diffuse gliomas in the Japanese population.
抄録全体を表示PDF形式でダウンロード (2067K) -
Misao NISHIKAWA, Paolo A. BOLOGNESE, Toru YAMAGATA, Kentarou NAITO, Hi ...2022 年 62 巻 9 号 p. 400-415
発行日: 2022/09/15
公開日: 2022/09/15
[早期公開] 公開日: 2022/08/27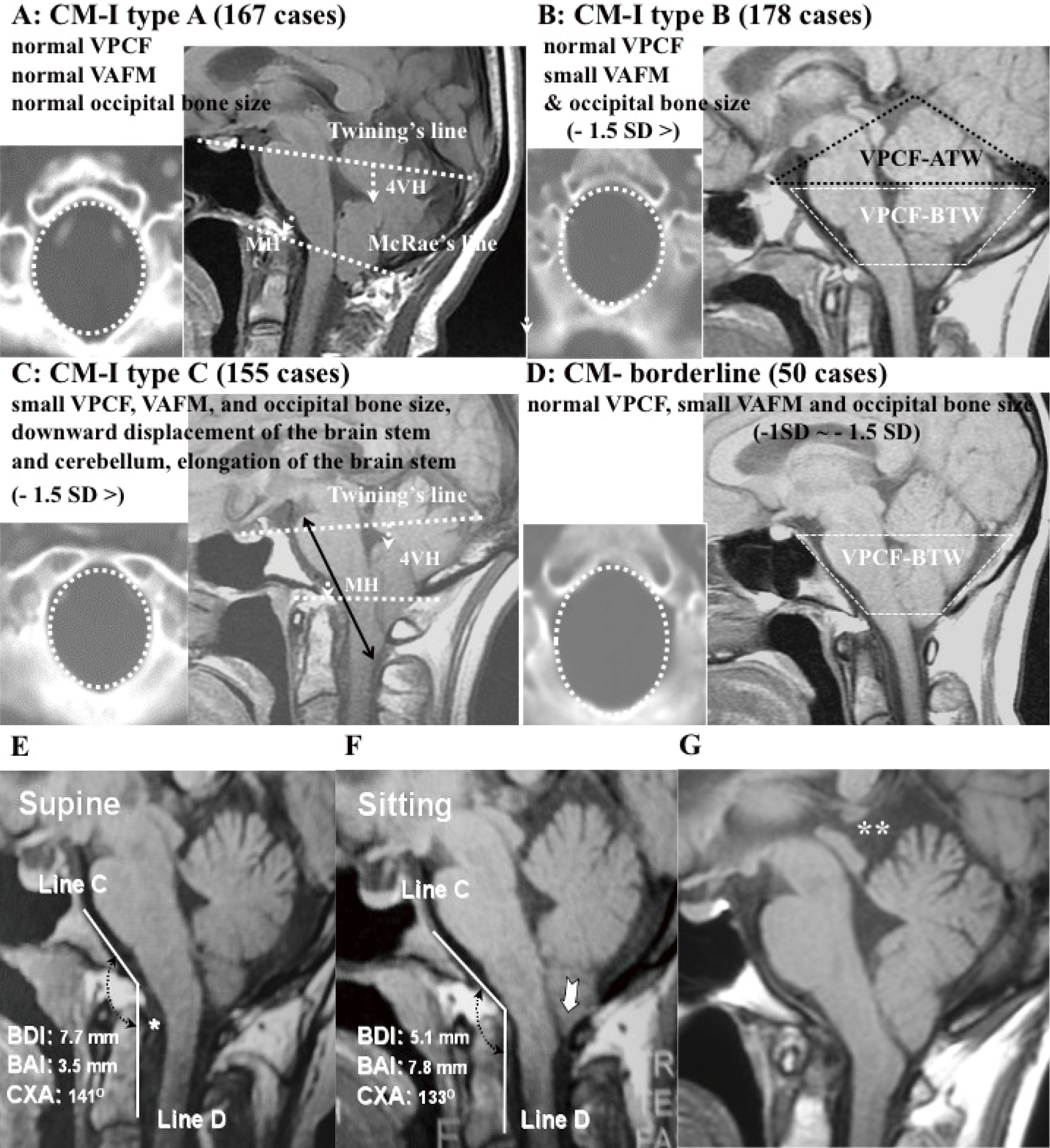 ジャーナル オープンアクセス
ジャーナル オープンアクセスWe investigated the mechanism underlying Chiari malformation type I (CM-I) and classified it according to the morphometric analyses of posterior cranial fossa (PCF) and craniocervical junction (CCJ). Three independent subtypes of CM-I were confirmed (CM-I types A, B, and C) for 484 cases and 150 normal volunteers by multiple analyses. CM-I type A had normal volume of PCF (VPCF) and occipital bone size. Type B had normal VPCF and small volume of the area surrounding the foramen magnum (VAFM) and occipital bone size. Type C had small VPCF, VAFM, and occipital bone size. Morphometric analyses during craniocervical traction test demonstrated instability of CCJ. Foramen magnum decompression (FMD) was performed in 302 cases. Expansive suboccipital cranioplasty (ESCP) was performed in 102 cases. Craniocervical posterolateral fixation (CCF) was performed for CCJ instability in 70 cases. Both ESCP and FMD showed a high improvement rate of neurological symptoms and signs (84.4%) and a high recovery rate of the Japanese Orthopaedic Association (JOA) score (58.5%). CCF also showed a high recovery rate of the JOA score (69.7%), with successful joint stabilization (84.3%). CM-I type A was associated with other mechanisms that caused ptosis of the brainstem and cerebellum (CCJ instability and traction and pressure dissociation between the intracranial cavity and spinal canal cavity), whereas CM-I types B and C demonstrated underdevelopment of the occipital bone. For CM-I types B and C, PCF decompression should be performed, whereas for small VPCF, ESCP should be performed. CCF for CCJ instability (including CM-I type A) was safe and effective.
抄録全体を表示PDF形式でダウンロード (1913K) -
Young-Soo PARK2022 年 62 巻 9 号 p. 416-430
発行日: 2022/09/15
公開日: 2022/09/15
[早期公開] 公開日: 2022/08/27 ジャーナル オープンアクセス
ジャーナル オープンアクセスTreatment for pediatric hydrocephalus aims not only to shrink the enlarged ventricle morphologically but also to create an intracranial environment that provides the best neurocognitive development and to deal with various treatment-related problems over a long period of time. Although the primary diseases that cause hydrocephalus are diverse, the ventricular peritoneal shunt has been introduced as the standard treatment for several decades. Nevertheless, complications such as shunt infection and shunt malfunction are unavoidable; the prognosis of neurological function is severely affected by such factors, especially in newborns and infants.
In recent years, treatment concepts have been attempted to avoid shunting, mainly in the context of pediatric cases. In this review, the current role of neuroendoscopic third ventriculostomy for noncommunicating hydrocephalus is discussed and a new therapeutic concept for post intraventricular hemorrhagic hydrocephalus in preterm infants is documented. To avoid shunt placement and achieve good neurodevelopmental outcomes for pediatric hydrocephalus, treatment modalities must be developed.
抄録全体を表示PDF形式でダウンロード (3377K)
-
Takashi SUGAWARA, Daisuke KOBAYASHI, Taketoshi MAEHARA2022 年 62 巻 9 号 p. 431-437
発行日: 2022/09/15
公開日: 2022/09/15
[早期公開] 公開日: 2022/08/10 ジャーナル オープンアクセス
ジャーナル オープンアクセス
電子付録No previous study has histopathologically investigated whether a meningioma capsule presents with tumor cells. We investigated which types of tumor capsules (TCs) included tumor cells to help intraoperatively determine those TCs that do not need to be removed and have a low recurrence risk. We investigated 22 specimens of 14 newly diagnosed meningiomas from February 2011 to June 2021. The capsules were classified into three types: TC, capsule-like thickened arachnoid membrane (CAM), and extended membrane (EM). Capsule properties were scored by hardness (soft = 1, medium = 2, hard = 3) and transparency (high = 1, medium = 2, low = 3). The hardness, transparency, and score sums were compared between capsules with and without tumor invasion in the CAM and EM types. The mean follow-up duration was 40.6 months, and there was only one recurrence in a remote location from the residual capsule. Nine capsules were classified as TC, seven as CAM, and six as EM. The tumor cells invaded 88.9% of TCs, 42.9% of CAMs, and 50% of EMs. The hardness, transparency, and score sums for CAMs with tumor invasion were lower than those for CAMs without tumor invasion, although not significant (P = 0.114, P = 0.114, P = 0.057, respectively). A thickened TC or soft and highly transparent CAM indicated a high risk for tumor cell invasion; thus, such cases require a careful and long-term follow-up. Hard and low transparent residual CAMs may have had a low risk for tumor invasion; therefore, leaving such capsules that tightly adhere to the eloquent cortex can be theoretically justified to avoid damaging the brain surface.
抄録全体を表示PDF形式でダウンロード (1449K)
-
Yuichiro TSUJI, Yusuke FUKUO, Takuya KANEMITSU, Yoshihide KATAYAMA, Ry ...2022 年 62 巻 9 号 p. 438-443
発行日: 2022/09/15
公開日: 2022/09/15
[早期公開] 公開日: 2022/08/27 ジャーナル オープンアクセス
ジャーナル オープンアクセスGiant cell tumor (GCT) of bone is essentially benign but locally aggressive, and the rate of local recurrence is high when the resection is not enough. En bloc resection is recommended as an ideal solution for GCT to decrease the risk of local recurrence, but it remains challenging for cervical GCT. In this technical case report, we present a case of extensively infiltrating GCT of the cervical spine completely encasing the vertebral artery (VA) on one side. The tumor was distributed to layers A-D, sectors 3-8 based on the Weinstein-Boriani-Biagini staging. Combined posterior and anterior surgical approach for the cervical spine was successfully performed and followed by postoperative adjuvant pharmacological therapy. This kind of multimodal management may be one of the solutions for advanced cervical GCT.
抄録全体を表示PDF形式でダウンロード (1073K)
-
2022 年 62 巻 9 号 p. EC17-EC18
発行日: 2022年
公開日: 2022/09/15
ジャーナル オープンアクセスPDF形式でダウンロード (53K)
- |<
- <
- 1
- >
- >|